Ventilating the Sick Lung Mike Dougherty RRT-NPS
|
|
|
- Millicent Morgan
- 5 years ago
- Views:
Transcription
1 Ventilating the Sick Lung 2018 Mike Dougherty RRT-NPS
2 Goals and Objectives Discuss some Core Principles of Ventilation relevant to mechanical ventilation moving forward. Compare and Contrast High MAP strategies of ventilation. Familiarize clinicians with some of the key papers impacting ventilation strategy today.
3 Peep and FRC
4 FRC Functional Residual Capacity 30ml/kg 2100 ml in an 70 kg male 70 kg 6cc-8cc vt

5 Peep is Volume


6 Peep Needed? L Mid lobe Pneumonia ARDS
7 ArdsnetVT Goal 6ml/kg What About Peep?
8 High or Low Peep? 2004 Higher versus Lower Positive End-Expiratory Pressures in Patients with the Acute Respiratory Distress Syndrome The National Heart, Lung, and Blood Institute ARDS Clinical Trials Network* N Engl J Med 2004; 351: Conclusions These results suggest that in patients with acute lung injury and ARDS who receive mechanical ventilation with a tidal-volume goal of 6 ml per kilogram of predicted body weight and an end-inspiratory plateau-pressure limit of 30 cm of water, clinical outcomes are similar whether lower or higher PEEP levels are used.
9 High vs Low Peep? 2017 In conclusion, we have performed an updated meta-analysis of clinical trials comparing higher PEEP to lower PEEP strategies among patients with ARDS Conclusions: Use of higher PEEP is unlikely to improve clinical outcomes among unselected patients with ARDS. Walkey, Del Sorbo, Hodgson, et al.: PEEP in ARDS AnnalsATS Volume 14 Supplement 4 October 2017

10 What Does it all Mean?


11 Amato et al NEJM 2015 METHODS: Using a statistical tool known as multilevel mediation analysis to analyze individual data from 3562 patients with ARDS enrolled in nine previously reported randomized trials, we examined P as an independent variable associated with survival. In the mediation analysis, we estimated the isolated effects of changes in P resulting from randomized ventilator settings while minimizing confounding due to the baseline severity of lung disease. CONCLUSIONSWe found that P was the ventilation variable that best stratified risk. Decreases in P owing to changes in ventilator settings were strongly associated with increased survival. N Engl J Med 2015;372:

12 Driving pressure: a marker of severity, a safety limit, or a goal for mechanical ventilation? Although there is insufficient evidence to suggest a specific cutoff value for driving pressure, we propose 15 cm H2O, not as a target, but as a safety limit. Driving pressure may be a valuable tool to set PEEP. Independent of the strategy used to titrate PEEP, changes in PEEP levels should consider the impact on driving pressure, besides other variables such as gas exchange and hemodynamics [3, 32, 33]. A decrease in driving pressure after increasing PEEP will necessarily reflect recruitment and a decrease in cyclic strain. On the contrary, an increase in driving pressure will suggest a non-recruitable lung Bugedo et al. Critical Care (2017) 21:199
13 Driving Pressure Plateau Peep = Driving pressure ( P) 22 7 = 15
14 High MAP Strategies APRV? Peep? HFO? Inverse I:E

15 Inverse I:E

16 Traditional vs Inverse I:E What Changes? 1-2 I:E 2-1 I:E
17 Neuromuscular Blockers in Early Acute Respiratory Distress Laurent Papazian, M.D., Ph.D., Jean-Marie Forel, M.D., Arnaud Gacouin, M.D et al. ACURASYS Trial Multicenter, double-blind trial, 340 patients presenting to the intensive care unit (ICU) with an onset of severe ARDS within the previous 48 hours were randomly assigned to receive, for 48 hours, either cisatracurium besylate (178 patients) or placebo (162 patients). The primary outcome was the proportion of patients who died either before hospital discharge or within 90 days after study enrollment Treated with volume assist-control mode of ventilation, tidal volumes of 6-8ml/kg of predicted body weight. Target SpO % or PaO mmHg. FiO2 and PEEP adjusted according to ARMA trial protocol. In patients with severe ARDS, early administration of a neuromuscular blocking agent improved the adjusted 90-day survival and increased the time off the ventilator without increasing muscle weakness. N Engl J Med 2010; 363:


18 APRV vs Inverse I:E Both Are PC With Extended I Time

19 Airway Pressure Release Ventilation
20 APRV in 2018 Remains Controversial 1) APRV is a mode of mechanical ventilation that has generated enough controversy to fuel a war. Journal ListJ Thorac Disv.10(Suppl 9); ) APRV is the Devil s Spawn. I'll let that hyperbole be published. Rich Kallet Respiratory Care June 2016 Should Airway Pressure Release Ventilation Be the Primary Mode in ARDS? 3) Early application of airway pressure release ventilation may reduce the duration of mechanical ventilation in acute respiratory distress syndrome Intensive Care Med. 2017; 43(11):


21 Note Peak expiratory Flow Assure that flow does not return to 0 on exhalation Capture between 75-50% of PEF Reassess Frequently


22


23 2008 OPEN FORUM Abstracts MEASUREMENT OF EXPIRATORY VALVE RESISTANCE AND ITS EFFECT ON T LOW USING APRV MODE AND A LOWCOMPLIANCE LUNG MODEL. Misty Starnes, Aaron Light, Doug Pursley, Monica Hall, Jodie Ketterman, Megan Saviello Observed the T low needed to achieve 50% of PEFR in a lung model. Avea = 0.7 s 840 = 0.63 s Drager XL = 0.6 s Servo i = 0.4 s. 08_245 12/3/2010


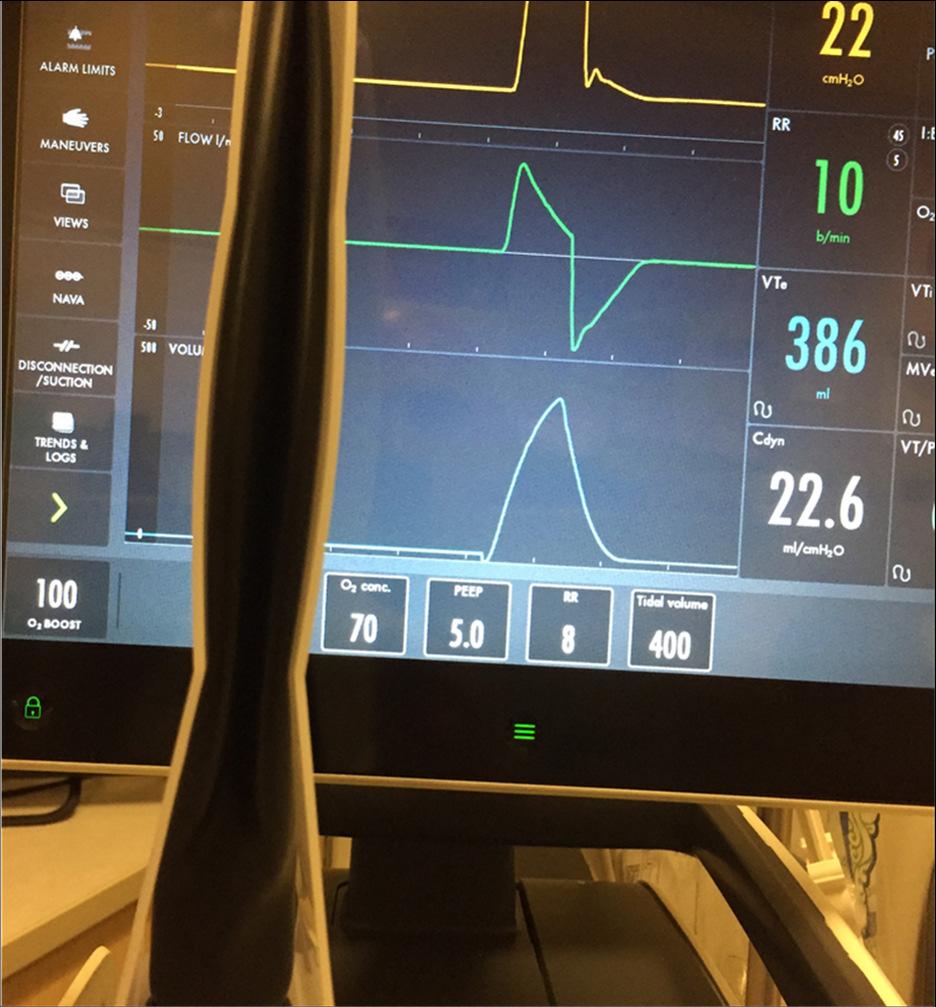
24 ARDSnet ARDSnet Low Peep

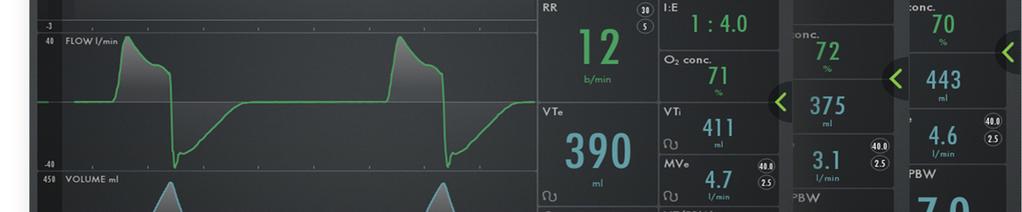
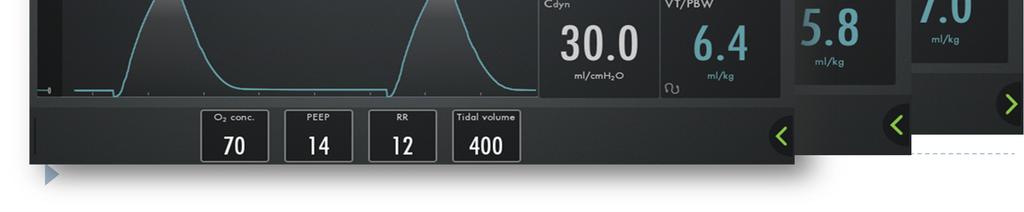
25 High MAP
26 Driving Pressure Peep 14 Peep 5

27 Driving Pressure Driving Pressure 12 Driving Pressure 16 Note improved compliance with higher Peep
28 Pressure vs Volume Ventilation Volume: Set Flow, variable pressure RR/VT/FIO2/Peep 10/500/60 +5 Pressure: Set pressure, variable flow and tidal volume. RR/PIP/Peep/FIO2/I time 10 20/ I time

29

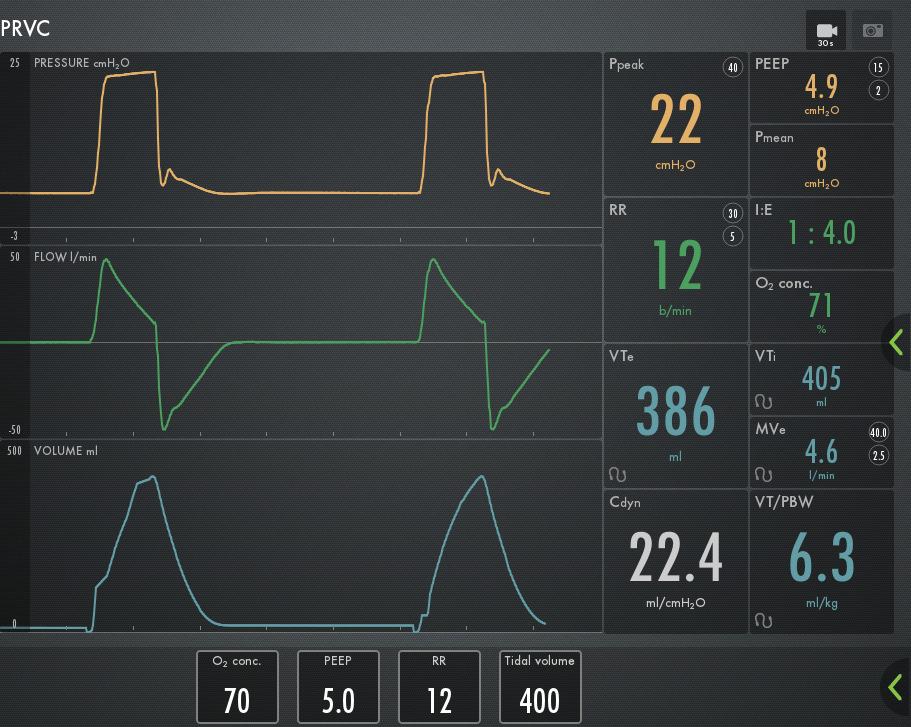
30 Volume and Pressure PRVC Pressure

31 Plateau Pressure Fixed Flow Volume Pressure
32 Dual Mode Commentary From Kallet 1. In a 6 month period I found 4 patients in overt shock with a peak pressure of The Rule of thumb is if your peak pressure on someone who is very sick is less than 20, you need to take a closer look. 3. If your peak pressures on a dual mode are in the mid 20s to 30s, I don t have a problem with it at all Paraphrased for length complete text page 84 Jan 2011 Resp Care
33 Bedside Approach Observe! 1. PIP 2. MAP (PMean)

34
35

36 What Do You Do? Traditional Volume Ventilation? Issue is that the patient is demanding a higher volume, limiting the volume will result in severe asynchrony. You can do it, but you will need to apply heavy sedation

37 What Do You Do Part 2 Pressure Ventilate Set Pressure to 20, you will then achieve a higher MAP. Note Driving pressure Note tidal volumes because they are variable
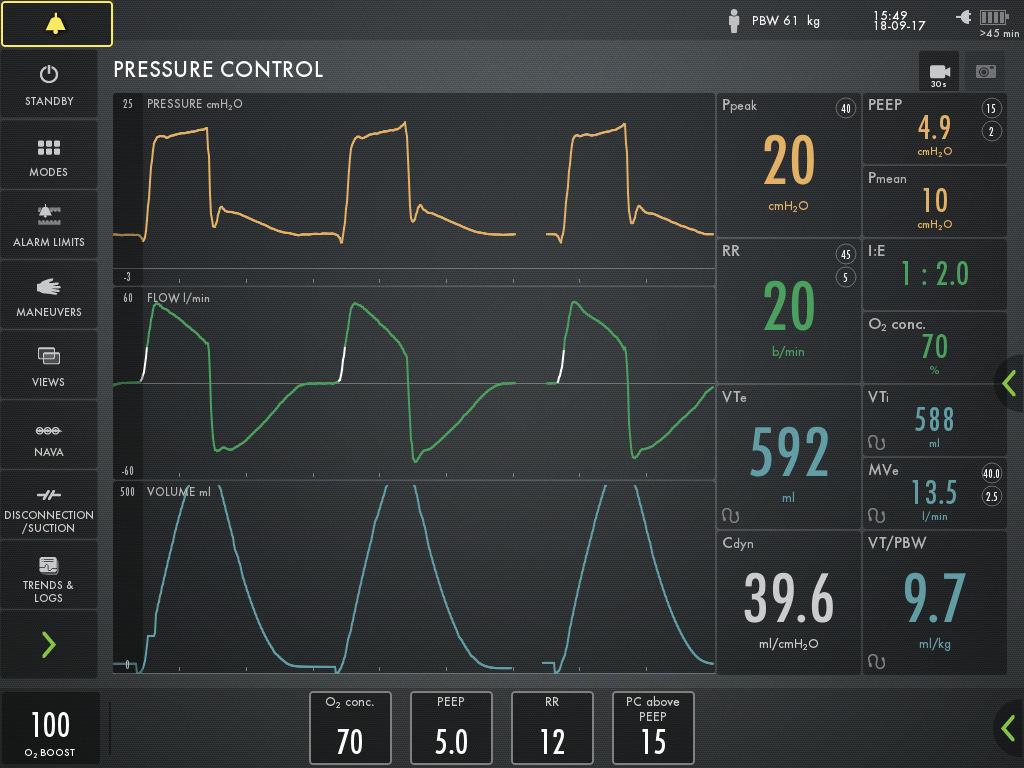
38
 NEJM")
 ARDS.")
39 Homework Print Out and Take Back This Evidence 1) NEJM Driving pressure and Survival ) ARDS.net Ventilator Protocol card

40 Summary Don t neglect MAP! Have A High MAP strategy you are comfortable with in your facility. Be sure to use enough Peep. Print and carry ARDSnet Be sure to track Vt per kg for your sicker patients. Embrace Driving pressure <15
Driving Pressure. What is it, and why should you care?
 Driving Pressure What is it, and why should you care? Jonathan Pak MD March 2, 2017 Lancet 1967; 290: 319-323 Traditional Ventilation in ARDS Tidal Volume (V T ) = 10-15 ml/kg PBW PEEP = 5-12 cm H 2 O
Driving Pressure What is it, and why should you care? Jonathan Pak MD March 2, 2017 Lancet 1967; 290: 319-323 Traditional Ventilation in ARDS Tidal Volume (V T ) = 10-15 ml/kg PBW PEEP = 5-12 cm H 2 O
excellence in care Procedure Management of patients with difficult oxygenation. For Review Aug 2015
 Difficult Oxygenation HELI.CLI.12 Purpose This procedure describes the processes and procedures for a lung protective strategy in the mechanical ventilation of patients that are difficult to oxygenate
Difficult Oxygenation HELI.CLI.12 Purpose This procedure describes the processes and procedures for a lung protective strategy in the mechanical ventilation of patients that are difficult to oxygenate
Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X
 HELICOPTER OPERATING PROCEDURE HOP No: C/12 Issued: May 2011 Page: 1 of 5 Revision No: Original Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X TRIM No: 09/300 Document No: D10/9973 X
HELICOPTER OPERATING PROCEDURE HOP No: C/12 Issued: May 2011 Page: 1 of 5 Revision No: Original Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X TRIM No: 09/300 Document No: D10/9973 X
Why we should care (I)
") What the $*!# is Lung Protective Ventilation and Why Should I be Using it in the OR? Disclosures KATHERINE PALMIERI, MD, MBA 64 TH ANNUAL POSTGRADUATE SYMPOSIUM UNIVERSITY OF KANSAS MEDICAL CENTER DEPARTMENT
What the $*!# is Lung Protective Ventilation and Why Should I be Using it in the OR? Disclosures KATHERINE PALMIERI, MD, MBA 64 TH ANNUAL POSTGRADUATE SYMPOSIUM UNIVERSITY OF KANSAS MEDICAL CENTER DEPARTMENT
ONLINE DATA SUPPLEMENT. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg
 APPENDIX 1 Appendix 1. Complete respiratory protocol. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg predicted body weight (PBW)) (NEJM 2000; 342
APPENDIX 1 Appendix 1. Complete respiratory protocol. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg predicted body weight (PBW)) (NEJM 2000; 342
APRV: Moving beyond ARDSnet
 APRV: Moving beyond ARDSnet Matthew Lissauer, MD Associate Professor of Surgery Medical Director, Surgical Critical Care Rutgers, The State University of New Jersey What is APRV? APRV is different from
APRV: Moving beyond ARDSnet Matthew Lissauer, MD Associate Professor of Surgery Medical Director, Surgical Critical Care Rutgers, The State University of New Jersey What is APRV? APRV is different from
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES
 INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES") INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
Mechanical Ventilation. Which of the following is true regarding ventilation? Basics of Ventilation
 Mechanical Ventilation Jeffrey L. Wilt, MD, FACP, FCCP Associate Professor of Medicine Michigan State University Associate Program Director MSU-Grand Rapids Internal Medicine Residency Which of the following
Mechanical Ventilation Jeffrey L. Wilt, MD, FACP, FCCP Associate Professor of Medicine Michigan State University Associate Program Director MSU-Grand Rapids Internal Medicine Residency Which of the following
Pressure Controlled Modes of Mechanical Ventilation
 Pressure Controlled Modes of Mechanical Ventilation Christopher Junker Department of Anesthesiology & Critical Care Medicine George Washington University Saturday, August 20, 2011 Assist Control Hypoxemic
Pressure Controlled Modes of Mechanical Ventilation Christopher Junker Department of Anesthesiology & Critical Care Medicine George Washington University Saturday, August 20, 2011 Assist Control Hypoxemic
What is Lung Protective Ventilation? NBART 2016
 What is Lung Protective Ventilation? NBART 2016 Disclosure Full time employee of Draeger Outline 1. Why talk about Lung Protective Ventilation? 2. What is Lung Protective Ventilation? 3. How to apply Lung
What is Lung Protective Ventilation? NBART 2016 Disclosure Full time employee of Draeger Outline 1. Why talk about Lung Protective Ventilation? 2. What is Lung Protective Ventilation? 3. How to apply Lung
Mechanical Ventilation of the Patient with ARDS
 1 Mechanical Ventilation of the Patient with ARDS Dean Hess, PhD, RRT, FAARC Assistant Professor of Anesthesia Harvard Medical School Assistant Director of Respiratory Care Massachusetts General Hospital
1 Mechanical Ventilation of the Patient with ARDS Dean Hess, PhD, RRT, FAARC Assistant Professor of Anesthesia Harvard Medical School Assistant Director of Respiratory Care Massachusetts General Hospital
Using Common Ventilator Graphics to Provide Optimal Ventilation
 Using Common Ventilator Graphics to Provide Optimal Ventilation David Vines, MHS, RRT, FAARC Associate Professor Chair / Program Director Department of Respiratory Care RUSH UNIVERSITY MEDICAL CENTER Disclosure
Using Common Ventilator Graphics to Provide Optimal Ventilation David Vines, MHS, RRT, FAARC Associate Professor Chair / Program Director Department of Respiratory Care RUSH UNIVERSITY MEDICAL CENTER Disclosure
Mechanical Ventilation
 Mechanical Ventilation Understanding Modes Rob Chatburn, RRT-NPS, FAARC Research Manager Respiratory Therapy Cleveland Clinic Associate Professor Case Western Reserve University 1 Overview Characteristics
Mechanical Ventilation Understanding Modes Rob Chatburn, RRT-NPS, FAARC Research Manager Respiratory Therapy Cleveland Clinic Associate Professor Case Western Reserve University 1 Overview Characteristics
Initiation and Management of Airway Pressure Release Ventilation (APRV)
") Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Advanced Ventilator Modes. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine
 Advanced Ventilator Modes Shekhar T. Venkataraman M.D. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Advanced modes Pressure-Regulated
Advanced Ventilator Modes Shekhar T. Venkataraman M.D. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Advanced modes Pressure-Regulated
SUPPLEMENTARY APPENDIX. Ary Serpa Neto MD MSc, Fabienne D Simonis MD, Carmen SV Barbas MD PhD, Michelle Biehl MD, Rogier M Determann MD PhD, Jonathan
 1 LUNG PROTECTIVE VENTILATION WITH LOW TIDAL VOLUMES AND THE OCCURRENCE OF PULMONARY COMPLICATIONS IN PATIENTS WITHOUT ARDS: a systematic review and individual patient data metaanalysis SUPPLEMENTARY APPENDIX
1 LUNG PROTECTIVE VENTILATION WITH LOW TIDAL VOLUMES AND THE OCCURRENCE OF PULMONARY COMPLICATIONS IN PATIENTS WITHOUT ARDS: a systematic review and individual patient data metaanalysis SUPPLEMENTARY APPENDIX
Underlying Principles of Mechanical Ventilation: An Evidence-Based Approach
 Underlying Principles of Mechanical Ventilation: An Evidence-Based Approach Ira M. Cheifetz, MD, FCCM, FAARC Professor of Pediatrics and Anesthesiology Chief Medical Officer, Children s Services Associate
Underlying Principles of Mechanical Ventilation: An Evidence-Based Approach Ira M. Cheifetz, MD, FCCM, FAARC Professor of Pediatrics and Anesthesiology Chief Medical Officer, Children s Services Associate
VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL
 VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National
VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National
Basics of Mechanical Ventilation. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of Mechanical Ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Overview of topics 1. Goals 2. Settings 3. Modes 4. Advantages and disadvantages
Basics of Mechanical Ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Overview of topics 1. Goals 2. Settings 3. Modes 4. Advantages and disadvantages
Selecting the Ventilator and the Mode. Chapter 6
 Selecting the Ventilator and the Mode Chapter 6 Criteria for Ventilator Selection Why does the patient need ventilatory support? Does the ventilation problem require a special mode? What therapeutic goals
Selecting the Ventilator and the Mode Chapter 6 Criteria for Ventilator Selection Why does the patient need ventilatory support? Does the ventilation problem require a special mode? What therapeutic goals
Lung recruitment maneuvers
 White Paper Lung recruitment maneuvers Assessment of lung recruitability and performance of recruitment maneuvers using the P/V Tool Pro Munir A Karjaghli RRT, Clinical Application Specialist, Hamilton
White Paper Lung recruitment maneuvers Assessment of lung recruitability and performance of recruitment maneuvers using the P/V Tool Pro Munir A Karjaghli RRT, Clinical Application Specialist, Hamilton
Invasive Ventilation: State of the Art
 ARDSnet NEJM 2000;342:1301 9-30-17 Cox Invasive Ventilation: State of the Art Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts A V T of 6 ml/kg PBW results
ARDSnet NEJM 2000;342:1301 9-30-17 Cox Invasive Ventilation: State of the Art Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts A V T of 6 ml/kg PBW results
Sumit Ray Senior Consultant & Vice-Chair Critical Care & Emergency Medicine Sir Ganga Ram Hospital
 Sumit Ray Senior Consultant & Vice-Chair Critical Care & Emergency Medicine Sir Ganga Ram Hospital ARDS pathophysiology B Taylor Thompson et al. NEJM 2017;377:562-72. Outcome Australian Epidemiologic
Sumit Ray Senior Consultant & Vice-Chair Critical Care & Emergency Medicine Sir Ganga Ram Hospital ARDS pathophysiology B Taylor Thompson et al. NEJM 2017;377:562-72. Outcome Australian Epidemiologic
Automatic Transport Ventilator
 Automatic Transport Ventilator David M. Landsberg, MD, FACP, FCCP, EMT-P Luke J. Gasowski, RRT, NPS, ACCS, CCP-C, FP-C Christopher J. Fullagar, MD, FACEP, EMT-P Stan Goettel, MS, EMT-P Author credits /
Automatic Transport Ventilator David M. Landsberg, MD, FACP, FCCP, EMT-P Luke J. Gasowski, RRT, NPS, ACCS, CCP-C, FP-C Christopher J. Fullagar, MD, FACEP, EMT-P Stan Goettel, MS, EMT-P Author credits /
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Talmor D, Sarge T, Malhotra A, et al. Mechanical ventilation
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Talmor D, Sarge T, Malhotra A, et al. Mechanical ventilation
Mechanical Ventilation
 Mechanical Ventilation Chapter 4 Mechanical Ventilation Equipment When providing mechanical ventilation for pediatric casualties, it is important to select the appropriately sized bag-valve mask or endotracheal
Mechanical Ventilation Chapter 4 Mechanical Ventilation Equipment When providing mechanical ventilation for pediatric casualties, it is important to select the appropriately sized bag-valve mask or endotracheal
Mechanical Ventilation. Mechanical Ventilation is a Drug!!! is a drug. MV: Indications for use. MV as a Drug: Outline. MV: Indications for use
 Mechanical Ventilation is a Drug!!! Mechanical Ventilation is a drug I am an employee of Philips Healthcare Hospital Respiratory Care Group and they help me pay for my kids education Jim Laging, RRT, RCP
Mechanical Ventilation is a Drug!!! Mechanical Ventilation is a drug I am an employee of Philips Healthcare Hospital Respiratory Care Group and they help me pay for my kids education Jim Laging, RRT, RCP
Alveolar Recruiment for ARDS Trial
 Alveolar Recruiment for ARDS Trial Alexandre Biasi Cavalcanti HCor Research Institute For the ART Investigators Trial Organization Coordination: HCor Research Institute (Sao Paulo, Brazil). Support: Brazilian
Alveolar Recruiment for ARDS Trial Alexandre Biasi Cavalcanti HCor Research Institute For the ART Investigators Trial Organization Coordination: HCor Research Institute (Sao Paulo, Brazil). Support: Brazilian
Potential Conflicts of Interest Received research grants from Hamilton, Covidien, Drager, General lel Electric, Newport, and Cardinal Medical Received
 How Does a Mechanical Ventilator t 6-22-10 Spain Work? Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts Potential Conflicts of Interest Received research
How Does a Mechanical Ventilator t 6-22-10 Spain Work? Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts Potential Conflicts of Interest Received research
Neonatal tidal volume targeted ventilation
 Neonatal tidal volume targeted ventilation Colin Morley Retired Professor of Neonatal Medicine, Royal Women s Hospital, Melbourne, Australia. Honorary Visiting Fellow, Dept Obstetrics and Gynaecology,
Neonatal tidal volume targeted ventilation Colin Morley Retired Professor of Neonatal Medicine, Royal Women s Hospital, Melbourne, Australia. Honorary Visiting Fellow, Dept Obstetrics and Gynaecology,
Mechanical Ventilation. Flow-Triggering. Flow-Triggering. Advanced Concepts. Advanced Concepts in Mechanical Ventilation
 Mechanical Ventilation Advanced Concepts in Mechanical Ventilation Flow-Triggering Trigger = the variable that causes the vent to begin the inspiratory phase Common triggers 1-2- 3- Effort required to
Mechanical Ventilation Advanced Concepts in Mechanical Ventilation Flow-Triggering Trigger = the variable that causes the vent to begin the inspiratory phase Common triggers 1-2- 3- Effort required to
Key words: intrahospital transport; manual ventilation; patient-triggered ventilation; respiratory failure
 Intrahospital Transport of Critically Ill Patients Using Ventilator With Patient- Triggering Function* Toshiaki Nakamura, MD; Yuji Fujino, MD; Akinori Uchiyama, MD; Takashi Mashimo, MD; and Masaji Nishimura,
Intrahospital Transport of Critically Ill Patients Using Ventilator With Patient- Triggering Function* Toshiaki Nakamura, MD; Yuji Fujino, MD; Akinori Uchiyama, MD; Takashi Mashimo, MD; and Masaji Nishimura,
Accumulation of EEV Barotrauma Affect hemodynamic Hypoxemia Hypercapnia Increase WOB Unable to trigger MV
 Complicated cases during mechanical ventilation Pongdhep Theerawit M.D. Pulmonary and Critical Care Division Ramathibodi Hospital Case I Presentation Male COPD 50 YO, respiratory failure, on mechanical
Complicated cases during mechanical ventilation Pongdhep Theerawit M.D. Pulmonary and Critical Care Division Ramathibodi Hospital Case I Presentation Male COPD 50 YO, respiratory failure, on mechanical
PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: INSTRUCTOR:
 PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: 1. **Identify and name the filters on the 7200ae. 2. **Explain how each filter is sterilized. 3. **Trace the gas flow through the ventilator
PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: 1. **Identify and name the filters on the 7200ae. 2. **Explain how each filter is sterilized. 3. **Trace the gas flow through the ventilator
Mechanical Ventilation Guided by Esophageal Pressure in Acute Lung Injury *
 A teaching hospital of Harvard Medical School Mechanical Ventilation Guided by Esophageal Pressure in Acute Lung Injury * Ray Ritz BA RRT FAARC Beth Israel Deaconess Medical Center Boston MA * n engl j
A teaching hospital of Harvard Medical School Mechanical Ventilation Guided by Esophageal Pressure in Acute Lung Injury * Ray Ritz BA RRT FAARC Beth Israel Deaconess Medical Center Boston MA * n engl j
Flight Medical presents the F60
 Flight Medical presents the F60 Reliable Ventilation Across the Spectrum of Care Adult & Pediatric Pressure/Volume Control Basic/Advanced Modes Invasive/NIV High Pressure/Low Flow O2 Up to 12 hours batteries
Flight Medical presents the F60 Reliable Ventilation Across the Spectrum of Care Adult & Pediatric Pressure/Volume Control Basic/Advanced Modes Invasive/NIV High Pressure/Low Flow O2 Up to 12 hours batteries
Volume Diffusion Respiration (VDR)
") Volume Diffusion Respiration (VDR) A therapy with many uses Jeffrey Pietz, MD April 15, 2016 VDR ventilation has been used to treat patients with: ARDS Meconium Aspiration Burn and Inhalation Injury RDS
Volume Diffusion Respiration (VDR) A therapy with many uses Jeffrey Pietz, MD April 15, 2016 VDR ventilation has been used to treat patients with: ARDS Meconium Aspiration Burn and Inhalation Injury RDS
6 th Accredited Advanced Mechanical Ventilation Course for Anesthesiologists. Course Test Results for the accreditation of the acquired knowledge
 6 th Accredited Advanced Mechanical Ventilation Course for Anesthesiologists Course Test Results for the accreditation of the acquired knowledge Q. Concerning the mechanics of the newborn s respiratory
6 th Accredited Advanced Mechanical Ventilation Course for Anesthesiologists Course Test Results for the accreditation of the acquired knowledge Q. Concerning the mechanics of the newborn s respiratory
Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo
 Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo Link full download: http://testbankcollection.com/download/pilbeams-mechanicalventilation-physiological-and-clinical-applications-5th-edition-test-bank-cairo
Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo Link full download: http://testbankcollection.com/download/pilbeams-mechanicalventilation-physiological-and-clinical-applications-5th-edition-test-bank-cairo
Respiratory Failure & Mechanical Ventilation. Denver Health Medical Center Department of Surgery and the University Of Colorado Denver
 Respiratory Failure & Mechanical Ventilation Denver Health Medical Center Department of Surgery and the University Of Colorado Denver + + Failure of the Respiratory Pump 1. Lack of patent airway 2. Bronchospasm
Respiratory Failure & Mechanical Ventilation Denver Health Medical Center Department of Surgery and the University Of Colorado Denver + + Failure of the Respiratory Pump 1. Lack of patent airway 2. Bronchospasm
Description: Percentage of cases with median tidal volumes less than or equal to 8 ml/kg.
 Measure Abbreviation: PUL 02 Description: Percentage of cases with median tidal volumes less than or equal to 8 ml/kg. NQS Domain: Patient Safety Measure Type: Process Scope: Calculated on a per case basis.
Measure Abbreviation: PUL 02 Description: Percentage of cases with median tidal volumes less than or equal to 8 ml/kg. NQS Domain: Patient Safety Measure Type: Process Scope: Calculated on a per case basis.
RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Pulmonary Function and
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Pulmonary Function and
Conflict of Interest Disclosure Robert M Kacmarek
 The Impact of Asynchrony on Patient Outcomes Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 6-1-15 CSRT Conflict of Interest Disclosure Robert M Kacmarek
The Impact of Asynchrony on Patient Outcomes Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 6-1-15 CSRT Conflict of Interest Disclosure Robert M Kacmarek
evolution 3e Ventilators
 evolution 3e Ventilators A new paradigm in blower-based ventilators, delivering ICU ventilator care anywhere, anytime. Comprehensive graphics and trending High performance PSOL and active exhalation Servo
evolution 3e Ventilators A new paradigm in blower-based ventilators, delivering ICU ventilator care anywhere, anytime. Comprehensive graphics and trending High performance PSOL and active exhalation Servo
The Basics of Ventilator Management. Overview. How we breath 3/23/2019
 The Basics of Ventilator Management What are we really trying to do here Peter Lutz, MD Pulmonary and Critical Care Medicine Pulmonary Associates, Mobile, Al Overview Approach to the physiology of the
The Basics of Ventilator Management What are we really trying to do here Peter Lutz, MD Pulmonary and Critical Care Medicine Pulmonary Associates, Mobile, Al Overview Approach to the physiology of the
NSQIP showed that the University of Utah was a high outlier in for patients receiving >48 cumulative hours of mechanical ventilation.
 A multidisciplinary quality improvement approach to ventilator management results in decreased ventilator times and a reduction in ventilator associated pneumonia Gillian eton MD, teven Johnson MBA, Gabriele
A multidisciplinary quality improvement approach to ventilator management results in decreased ventilator times and a reduction in ventilator associated pneumonia Gillian eton MD, teven Johnson MBA, Gabriele
The ARDSnet and Lung Protective Ventilation: Where Are We Today
 The ARDSnet and Lung Protective Ventilation: Where Are We Today 4-16-12 RCSW Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Disclosure
The ARDSnet and Lung Protective Ventilation: Where Are We Today 4-16-12 RCSW Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Disclosure
Mechanical power and opening pressure. Fellowship training program Intensive Care Radboudumc, Nijmegen
 Mechanical power and opening pressure Fellowship training program Intensive Care Radboudumc, Nijmegen Mechanical power Energy applied to the lung: Ptp * V (Joule) Power = Energy per minute (J/min) Power
Mechanical power and opening pressure Fellowship training program Intensive Care Radboudumc, Nijmegen Mechanical power Energy applied to the lung: Ptp * V (Joule) Power = Energy per minute (J/min) Power
Work of Breathing in Adaptive Pressure Control Continuous Mandatory Ventilation
 Work of Breathing in Adaptive Pressure Control Continuous Mandatory Ventilation Eduardo Mireles-Cabodevila MD and Robert L Chatburn RRT-NPS FAARC BACKGROUND: Adaptive pressure control is a mode of mechanical
Work of Breathing in Adaptive Pressure Control Continuous Mandatory Ventilation Eduardo Mireles-Cabodevila MD and Robert L Chatburn RRT-NPS FAARC BACKGROUND: Adaptive pressure control is a mode of mechanical
High Frequency Ventilation. Neil MacIntyre MD Duke University Medical Center Durham NC USA
 High Frequency Ventilation Neil MacIntyre MD Duke University Medical Center Durham NC USA High frequency ventilation Concept of ventilator induced lung injury and lung protective ventilatory strategies
High Frequency Ventilation Neil MacIntyre MD Duke University Medical Center Durham NC USA High frequency ventilation Concept of ventilator induced lung injury and lung protective ventilatory strategies
Disclosures. The Pediatric Challenge. Topics for Discussion. Traditional Anesthesia Machine. Tidal Volume = mls/kg 2/13/14
 2/13/14 Disclosures Optimal Ventilation of the Pediatric Patient in the OR Consulting Draeger Medical Jeffrey M. Feldman, MD, MSE Division Chief, General Anesthesia Dept. of Anesthesiology and Critical
2/13/14 Disclosures Optimal Ventilation of the Pediatric Patient in the OR Consulting Draeger Medical Jeffrey M. Feldman, MD, MSE Division Chief, General Anesthesia Dept. of Anesthesiology and Critical
Mechanical ven3la3on. Neonatal Mechanical Ven3la3on. Mechanical ven3la3on. Mechanical ven3la3on. Mechanical ven3la3on 8/25/11. What we need to do"
 8/25/11 Mechanical ven3la3on Neonatal Mechanical Ven3la3on Support oxygen delivery, CO2 elimination" Prevent added injury, decrease ongoing injury" Enhance normal development" Mark C Mammel, MD University
8/25/11 Mechanical ven3la3on Neonatal Mechanical Ven3la3on Support oxygen delivery, CO2 elimination" Prevent added injury, decrease ongoing injury" Enhance normal development" Mark C Mammel, MD University
Managing Patient-Ventilator Interaction in Pediatrics
 Managing Patient-Ventilator Interaction in Pediatrics Robert L. Chatburn, MHHS, RRT-NPS, FAARC Clinical Research Manager - Section of Respiratory Therapy Professor of Medicine Case Western Reserve University
Managing Patient-Ventilator Interaction in Pediatrics Robert L. Chatburn, MHHS, RRT-NPS, FAARC Clinical Research Manager - Section of Respiratory Therapy Professor of Medicine Case Western Reserve University
INTELLiVENT -ASV. The world s first Ventilation Autopilot
 INTELLiVENT -ASV The world s first Ventilation Autopilot Intelligent Ventilation since 1983 We live for ventilation technology We live for ventilation technology that helps caregivers improve the lives
INTELLiVENT -ASV The world s first Ventilation Autopilot Intelligent Ventilation since 1983 We live for ventilation technology We live for ventilation technology that helps caregivers improve the lives
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia and Critical Care Service Puerta de Hierro University Hospital Associate Professor.
 Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia and Critical Care Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM CV and Conflict of interest Chairman
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia and Critical Care Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM CV and Conflict of interest Chairman
What is an Optimal Paw Strategy?
 What is an Optimal Paw Strategy? A Physiological Rationale Anastasia Pellicano Neonatologist Royal Children s Hospital, Melbourne Acute injury sequence Barotrauma Volutrauma Atelectotrauma Biotrauma Oxidative
What is an Optimal Paw Strategy? A Physiological Rationale Anastasia Pellicano Neonatologist Royal Children s Hospital, Melbourne Acute injury sequence Barotrauma Volutrauma Atelectotrauma Biotrauma Oxidative
 http://www.priory.com/cmol/hfov.htm INTRODUCTION The vast majority of patients who are admitted to an Intensive Care Unit (ICU) will need artificial ventilation (Jones et al 1998). The usual means through
http://www.priory.com/cmol/hfov.htm INTRODUCTION The vast majority of patients who are admitted to an Intensive Care Unit (ICU) will need artificial ventilation (Jones et al 1998). The usual means through
Objectives. Respiratory Failure : Challenging Cases in Mechanical Ventilation. EM Knows Respiratory Failure!
 Respiratory Failure : Challenging Cases in Mechanical Ventilation Peter DeBlieux, MD, FAAEM, FACEP LSUHSC University Hospital Pulmonary and Critical Care Medicine Emergency Medicine pdebli@lsuhsc.edu Objectives
Respiratory Failure : Challenging Cases in Mechanical Ventilation Peter DeBlieux, MD, FAAEM, FACEP LSUHSC University Hospital Pulmonary and Critical Care Medicine Emergency Medicine pdebli@lsuhsc.edu Objectives
ARDS Network Investigators Response to the October 7, 2002 OHRP Letter
 ARDS Network Investigators Response to the October 7, 2002 OHRP Letter March 12, 2003 A. Concerns, questions, and allegations regarding the ARMA trial (ARDSNet Study 01): (1) OHRP is concerned that the
ARDS Network Investigators Response to the October 7, 2002 OHRP Letter March 12, 2003 A. Concerns, questions, and allegations regarding the ARMA trial (ARDSNet Study 01): (1) OHRP is concerned that the
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Indications for Mechanical Ventilation. Mechanical Ventilation. Indications for Mechanical Ventilation. Modes. Modes: Volume cycled
 Mechanical Ventilation Eric A. Libré, MD VCU School of Medicine Inova Fairfax Hospital and VHC Indications for Mechanical Ventilation Inadequate ventilatory effort Rising pco2 with resp acidosis (7.25)
Mechanical Ventilation Eric A. Libré, MD VCU School of Medicine Inova Fairfax Hospital and VHC Indications for Mechanical Ventilation Inadequate ventilatory effort Rising pco2 with resp acidosis (7.25)
UNDERSTANDING NEONATAL WAVEFORM GRAPHICS. Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services
 UNDERSTANDING NEONATAL WAVEFORM GRAPHICS Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services Disclosures Purpose: To enhance bedside staff s knowledge of ventilation and oxygenation
UNDERSTANDING NEONATAL WAVEFORM GRAPHICS Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services Disclosures Purpose: To enhance bedside staff s knowledge of ventilation and oxygenation
Introduction to Conventional Ventilation
 Introduction to Conventional Ventilation Dr Julian Eason Consultant Neonatologist Derriford Hospital Mechanics Inspiration diaphragm lowers and thorax expands Negative intrathoracic/intrapleural pressure
Introduction to Conventional Ventilation Dr Julian Eason Consultant Neonatologist Derriford Hospital Mechanics Inspiration diaphragm lowers and thorax expands Negative intrathoracic/intrapleural pressure
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate
 Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate
 Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Unassisted breathing and death as competing events in critical care trials
 Unassisted breathing and death as competing events in critical care trials William Checkley, MD, PhD Johns Hopkins University November 22, 2011 wcheckl1@jhmi.edu Objectives Jointly model the frequency
Unassisted breathing and death as competing events in critical care trials William Checkley, MD, PhD Johns Hopkins University November 22, 2011 wcheckl1@jhmi.edu Objectives Jointly model the frequency
Clinical Management Strategies for Airway Pressure Release Ventilation: A Survey of Clinical Practice
 Clinical Management Strategies for Airway Pressure Release Ventilation: A Survey of Clinical Practice Andrew G Miller RRT-ACCS RRT-NPS, Michael A Gentile RRT FAARC, John D Davies MA RRT FAARC, and Neil
Clinical Management Strategies for Airway Pressure Release Ventilation: A Survey of Clinical Practice Andrew G Miller RRT-ACCS RRT-NPS, Michael A Gentile RRT FAARC, John D Davies MA RRT FAARC, and Neil
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo
 Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
Presentation Overview. Monitoring Strategies for the Mechanically Ventilated Patient. Early Monitoring Strategies. Early Attempts To Monitor WOB
 Monitoring Strategies for the Mechanically entilated Patient Presentation Overview A look back into the future What works and what may work What s all the hype about the WOB? Are ventilator graphics really
Monitoring Strategies for the Mechanically entilated Patient Presentation Overview A look back into the future What works and what may work What s all the hype about the WOB? Are ventilator graphics really
Bunnell LifePulse HFV Quick Reference Guide # Bunnell Incorporated
 Bunnell Incorporated n www.bunl.com n 800-800-4358 (HFJV) n info@bunl.com 436 Lawndale Drive n Salt Lake City, Utah 84115 n intl 801-467-0800 n f 801-467-0867 Bunnell LifePulse HFV Quick Reference Guide
Bunnell Incorporated n www.bunl.com n 800-800-4358 (HFJV) n info@bunl.com 436 Lawndale Drive n Salt Lake City, Utah 84115 n intl 801-467-0800 n f 801-467-0867 Bunnell LifePulse HFV Quick Reference Guide
What can we learn from high-frequency ventilation?
 What can we learn from high-frequency ventilation? Dipartimento di Medicina Perioperatoria, Terapia Intensiva ed Emergenza Azienda Sanitaria Universitaria Integrata di Trieste Università degli Studi di
What can we learn from high-frequency ventilation? Dipartimento di Medicina Perioperatoria, Terapia Intensiva ed Emergenza Azienda Sanitaria Universitaria Integrata di Trieste Università degli Studi di
RESPIRATORY CARE POLICY AND PROCEDURE MANUAL. a) Persistent hypoxemia despite improved ventilatory pattern and elevated Fl02
 Persistent hypoxemia despite improved ventilatory pattern and elevated Fl02") The University of Mississippi AND PROCEDURE MANUAL Effective Date: June 30, 1990 Revised Date: December 2009 MANUAL CODE Page 1 of 5 PREPARED BY: Respiratory Care Policy and Procedure Review Committee
The University of Mississippi AND PROCEDURE MANUAL Effective Date: June 30, 1990 Revised Date: December 2009 MANUAL CODE Page 1 of 5 PREPARED BY: Respiratory Care Policy and Procedure Review Committee
Organis TestChest. Flight Simulator for Intensive Care Clinicians
 Organis TestChest Flight Simulator for Intensive Care Clinicians Organis TestChest Critical Care challenges Training on ventilation modes with simulation is crucial for patient safety The equipment and
Organis TestChest Flight Simulator for Intensive Care Clinicians Organis TestChest Critical Care challenges Training on ventilation modes with simulation is crucial for patient safety The equipment and
Guide to Understand Mechanical Ventilation Waveforms
 Do No Harm Ventilate Gently Guide to Understand Mechanical Ventilation Waveforms Middle East Critical Care Assembly 1/30/2015 Mazen Kherallah, MD, FCCP http://www.mecriticalcare.net Email: info@mecriticalcare.net
Do No Harm Ventilate Gently Guide to Understand Mechanical Ventilation Waveforms Middle East Critical Care Assembly 1/30/2015 Mazen Kherallah, MD, FCCP http://www.mecriticalcare.net Email: info@mecriticalcare.net
OPEN LUNG APPROACH CONCEPT OF MECHANICAL VENTILATION
 OPEN LUNG APPROACH CONCEPT OF MECHANICAL VENTILATION L. Rudo Mathivha Intensive Care Unit Chris Hani Baragwanath Aacademic Hospital & the University of the Witwatersrand OUTLINE Introduction Goals & Indications
OPEN LUNG APPROACH CONCEPT OF MECHANICAL VENTILATION L. Rudo Mathivha Intensive Care Unit Chris Hani Baragwanath Aacademic Hospital & the University of the Witwatersrand OUTLINE Introduction Goals & Indications
HFOV in the PICU and NICU setting
 in the PICU and NICU setting Courtesy from G. Niemann Peter C. Rimensberger, MD Associate Professor Pediatric and Neonatal Intensive Care University Hospital of Geneva Allowable V t depends on pathology
in the PICU and NICU setting Courtesy from G. Niemann Peter C. Rimensberger, MD Associate Professor Pediatric and Neonatal Intensive Care University Hospital of Geneva Allowable V t depends on pathology
How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital. Synopsis
 How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital Synopsis Definition of an oscillator Historical perspective Differences between HFOV and CMV Determinants
How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital Synopsis Definition of an oscillator Historical perspective Differences between HFOV and CMV Determinants
NAVA Neurally Adjusted Ventilatory Assist In Neonates
 NAVA Neurally Adjusted Ventilatory Assist In Neonates Howard Stein, M.D. Director Neonatology Toledo Children s Hospital Toledo, Ohio Disclaimers Dr Stein: Is on the speaker s bureau for Maquet Is discussing
NAVA Neurally Adjusted Ventilatory Assist In Neonates Howard Stein, M.D. Director Neonatology Toledo Children s Hospital Toledo, Ohio Disclaimers Dr Stein: Is on the speaker s bureau for Maquet Is discussing
Principles of mechanical ventilation. Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands
 Principles of mechanical ventilation Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands Disclosure Research grant Chiesi Pharmaceuticals Research grant CareFusion GA: 27 weeks,
Principles of mechanical ventilation Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands Disclosure Research grant Chiesi Pharmaceuticals Research grant CareFusion GA: 27 weeks,
VENTILATORS PURPOSE OBJECTIVES
 VENTILATORS PURPOSE To familiarize and acquaint the transfer Paramedic with the skills and knowledge necessary to adequately maintain a ventilator in the interfacility transfer environment. COGNITIVE OBJECTIVES
VENTILATORS PURPOSE To familiarize and acquaint the transfer Paramedic with the skills and knowledge necessary to adequately maintain a ventilator in the interfacility transfer environment. COGNITIVE OBJECTIVES
Ventilators. Dr Simon Walton Consultant Anaesthetist Eastbourne DGH KSS Basic Science Course
 Ventilators Dr Simon Walton Consultant Anaesthetist Eastbourne DGH KSS Basic Science Course Objectives Discuss Classification/ terminology Look at Modes of ventilation How some specific ventilators work
Ventilators Dr Simon Walton Consultant Anaesthetist Eastbourne DGH KSS Basic Science Course Objectives Discuss Classification/ terminology Look at Modes of ventilation How some specific ventilators work
Clinical Management Strategies for Airway Pressure Release Ventilation: A Survey of Clinical Practice
 Clinical Management Strategies for Airway Pressure Release Ventilation: A Survey of Clinical Practice Andrew G Miller RRT-ACCS RRT-NPS, Michael A Gentile RRT FAARC, John D Davies MA RRT FAARC, and Neil
Clinical Management Strategies for Airway Pressure Release Ventilation: A Survey of Clinical Practice Andrew G Miller RRT-ACCS RRT-NPS, Michael A Gentile RRT FAARC, John D Davies MA RRT FAARC, and Neil
VT PLUS HF performance verification of Bunnell Life-Pulse HFJV (High Frequency Jet Ventilator)
") VT PLUS HF performance verification of Bunnell Life-Pulse HFJV (High Frequency Jet Ventilator) VT PLUS HF provides a special mode for evaluating the performance of high frequency ventilators while connected
VT PLUS HF performance verification of Bunnell Life-Pulse HFJV (High Frequency Jet Ventilator) VT PLUS HF provides a special mode for evaluating the performance of high frequency ventilators while connected
Mechanical Ventilation 2016
 Conflict of Interest Disclosure Robert M Kacmarek Lung Protective Ventilation: New Information RT s Neec to Know 5-6-17 FOCUS Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital
Conflict of Interest Disclosure Robert M Kacmarek Lung Protective Ventilation: New Information RT s Neec to Know 5-6-17 FOCUS Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital
PART EIGHT HIGH FREQUENCY PERCUSSIVE OSCILLATION (HFPOV )
") PART EIGHT HIGH FREQUENCY PERCUSSIVE OSCILLATION (HFPOV ) Note: For maximal comparative understanding, FIRST read PART SEVEN which defines the concept of High Frequency Oscillatory Ventilation (HFOV).
PART EIGHT HIGH FREQUENCY PERCUSSIVE OSCILLATION (HFPOV ) Note: For maximal comparative understanding, FIRST read PART SEVEN which defines the concept of High Frequency Oscillatory Ventilation (HFOV).
Principles of Mechanical Ventilation: A Graphics-Based Approach
 Principles of Mechanical Ventilation: A Graphics-Based Approach Steven M. Donn, MD, FAAP Professor of Pediatrics Neonatal-Perinatal Medicine C.S. Mott Children s Hospital University of Michigan Health
Principles of Mechanical Ventilation: A Graphics-Based Approach Steven M. Donn, MD, FAAP Professor of Pediatrics Neonatal-Perinatal Medicine C.S. Mott Children s Hospital University of Michigan Health
Pressure -Volume curves in ARDS. G. Servillo
 Pressure -Volume curves in ARDS G. Servillo Dipartimento di Scienze Chirurgiche, Anestesiologiche- Rianimatorie e dell Emergenza Facoltà di Medicina e Chirurgia Università degli Studi di Napoli Federico
Pressure -Volume curves in ARDS G. Servillo Dipartimento di Scienze Chirurgiche, Anestesiologiche- Rianimatorie e dell Emergenza Facoltà di Medicina e Chirurgia Università degli Studi di Napoli Federico
carefusion.com CareFusion Yorba Linda, CA CareFusion
 CareFusion 22745 Savi Ranch Parkway Yorba Linda, CA 92887 800.231.2466 toll-free 714.283.2228 tel 714.283.8493 fax CareFusion Germany 234 GmbH Leibnizstrasse 7 97204 Hoechberg Germany +49 931 4972-0 tel
CareFusion 22745 Savi Ranch Parkway Yorba Linda, CA 92887 800.231.2466 toll-free 714.283.2228 tel 714.283.8493 fax CareFusion Germany 234 GmbH Leibnizstrasse 7 97204 Hoechberg Germany +49 931 4972-0 tel
CCAT Mechanical Ventilation Clinical Practice Guideline
 CCAT Mechanical Ventilation Clinical Practice Guideline Initial publication date: Mar 2012 Last update: 22 Oct 2013 I. Background and Introductory Information A. Mechanical ventilation can injure the lung.
CCAT Mechanical Ventilation Clinical Practice Guideline Initial publication date: Mar 2012 Last update: 22 Oct 2013 I. Background and Introductory Information A. Mechanical ventilation can injure the lung.
THE PURITAN BENNETT 980 VENTILATOR CLINICAL APPLICATIONS LESSON PLAN
 THE PURITAN BENNETT 980 VENTILATOR CLINICAL APPLICATIONS LESSON PLAN OVERVIEW This guide is provided as a convenience companion document to the Operator s Manual. It is not intended to replace the Operator
THE PURITAN BENNETT 980 VENTILATOR CLINICAL APPLICATIONS LESSON PLAN OVERVIEW This guide is provided as a convenience companion document to the Operator s Manual. It is not intended to replace the Operator
Prof. Javier García Fernández MD, Ph.D, MBA.
 Prof. Javier García Fernández MD, Ph.D, MBA. Chairman of Anesthesia & Perioperative Medicine Department Puerta de Hierro Universitary Hospital Prof. of Anaesthesia and Perioperative Medicine. Autonoma
Prof. Javier García Fernández MD, Ph.D, MBA. Chairman of Anesthesia & Perioperative Medicine Department Puerta de Hierro Universitary Hospital Prof. of Anaesthesia and Perioperative Medicine. Autonoma
WHAT IS SAFE VENTILATION? Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine
 WHAT IS SAFE VENTILATION? Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine holets.steven@mayo.edu DISCLOSURES Past and present Advisory Boards: Resmed Philips/Respironics
WHAT IS SAFE VENTILATION? Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine holets.steven@mayo.edu DISCLOSURES Past and present Advisory Boards: Resmed Philips/Respironics
Understanding and comparing modes of ventilation
 Understanding and comparing modes of ventilation Löwenstein Medical GmbH & Co. KG Content Volume-Controlled Ventilation Modes VCV PLV VC-SIMV Optional VCV Flexible VCV Pressure-Controlled Ventilation Modes
Understanding and comparing modes of ventilation Löwenstein Medical GmbH & Co. KG Content Volume-Controlled Ventilation Modes VCV PLV VC-SIMV Optional VCV Flexible VCV Pressure-Controlled Ventilation Modes
Leader: Anne Coble Voss, PhD, RD, LD, Abbott Nutrition, Columbus, OH
 Discussion Leader: Anne Coble Voss, PhD, RD, LD, Abbott Nutrition, Columbus, OH Dr Tisdale: Dr Bosaeus, you suggested that the drive to synthesize acute-phase proteins by the liver was actually driving
Discussion Leader: Anne Coble Voss, PhD, RD, LD, Abbott Nutrition, Columbus, OH Dr Tisdale: Dr Bosaeus, you suggested that the drive to synthesize acute-phase proteins by the liver was actually driving
Panther 5 Acute Care Ventilator
 1 HIGHLIGHTS High performance and advanced features target the ICU environment Utilizes an internal blower with a specially designed flow control valve removing the need for using compressed air without
1 HIGHLIGHTS High performance and advanced features target the ICU environment Utilizes an internal blower with a specially designed flow control valve removing the need for using compressed air without
 C CONFERENCIAS MAGISTRALES Vol. 34. Supl. 1 Abril-Junio 211 pp S293-S31 Perioperative ventilator management: Why it makes a difference Daniel R. Brown, PhD, MD, FCCM Chair, Division of Critical Care Medicine.
C CONFERENCIAS MAGISTRALES Vol. 34. Supl. 1 Abril-Junio 211 pp S293-S31 Perioperative ventilator management: Why it makes a difference Daniel R. Brown, PhD, MD, FCCM Chair, Division of Critical Care Medicine.
Astral in AirView: Improving patient care through connectivity. ResMed.com
 Astral in AirView: Improving patient care through connectivity ResMed.com Using Astral in AirView via the ResMed Connectivity Module (RCM) Astral is ResMed s portable, invasive and non-invasive life support
Astral in AirView: Improving patient care through connectivity ResMed.com Using Astral in AirView via the ResMed Connectivity Module (RCM) Astral is ResMed s portable, invasive and non-invasive life support
EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES
 GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
The Time Constant of The Respiratory System
 The Time Constant of The Respiratory System by Enrico Bulleri Today s post aims to facilitate the understanding of a difficult but fascinating concept of mechanical ventilation: the time constant. In the
The Time Constant of The Respiratory System by Enrico Bulleri Today s post aims to facilitate the understanding of a difficult but fascinating concept of mechanical ventilation: the time constant. In the
Astral in AirView: Improving patient care through connectivity. ResMed.com
 Astral in AirView: Improving patient care through connectivity ResMed.com This guide will assist you with: Setting up the ResMed Connectivity Module for Astral 2 Troubleshooting the ResMed Connectivity
Astral in AirView: Improving patient care through connectivity ResMed.com This guide will assist you with: Setting up the ResMed Connectivity Module for Astral 2 Troubleshooting the ResMed Connectivity