VENTILATION AND PERFUSION IN HEALTH AND DISEASE. Dr.HARIPRASAD VS
|
|
|
- Dwayne Goodman
- 6 years ago
- Views:
Transcription

1 VENTILATION AND PERFUSION IN HEALTH AND DISEASE Dr.HARIPRASAD VS

2 Ventilation Total ventilation - total rate of air flow in and out of the lung during normal tidal breathing. Alveolar ventilation -represents the amount of fresh inspired air available for gas exchange in alveolar gas compartment V A =V E -V D V A x n=v T x n-v D x n Also; V CO2 = V A xf CO2 V A = V CO2 /P CO2
3
4 Alveolar gas equation pao2 FIO2 PATM ph2o paco2 The alveolar partial pressure of oxygen The fraction of inspired gas that is oxygen The prevailing atmospheric pressure The saturated vapour pressure of water at body temperature The arterial partial pressure of carbon dioxide (pco2) 107 mmhg.21 RER The respiratory exchange ratio mmhg 47 mmhg 40 mmhg
5 Anatomical Dead space Volume of the conducting airways. Usually 150 Ml. Increases with large breath. Measured by fowler s or N 2 wash out method.
6 Subject breaths though a valve box N2 concentration at the mouth is analyzed Following a single breath of pure O 2,N 2 conc increases as dead space gas is washed out by the alveolar gas, finally reaching a plateau.
7 Physiologic dead space Physiologic dead space is the volume of lung that does not eliminate CO2 In normal subjects, Anatomical D.S = Physiological DS patients with lung disease, the physiologic DS > Anatomical D.S inequality of blood flow and ventilation within the lung
8
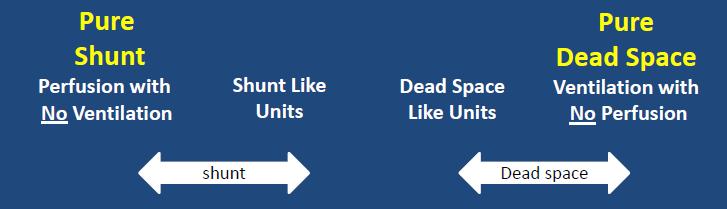
9 Dead space ventilation Pulmonary embolism Vascular obliteration ex. PAH Emphysema
10 Regional Differences in Ventilation change in volume per unit resting volume! lower regions of the lung ventilate better than do the upper zones. Supine position-ventilation of the lowermost (posterior) lung exceeds that of the uppermost (anterior) lung. Lateral position -the dependent lung is best ventilated.

11 Why? weight of the lung - lower portions of the lung requires a larger pressure below it than above it intrapleural pressure is less negative at the bottom. Basal region has a small resting volume, expanding pressure & placed on the steep part of the pressure volume curve. Paradox
12 At low lung volumes the intrapleural pressure at the base exceeds airway pressure. the lung at the base compressed, and ventilation is impossible until the intrapleural pressure falls apex of the lung is on a favourable part of the pressure-volume curve and ventilates well.
13 Airway Closure The compressed region of lung at the base does not have all its gas exhaled out. airways in the region of respiratory bronchioles close first trapping gas in the distal alveoli. 1. only at very low lung volumes in young normal subjects. 2. Elderly airway closure in the lowermost regions of the lung occurs at higher volumes Dependent regions of the lung may be only intermittently ventilated leading to defective gas exchange
14 Distribution of Blood Flow Blood flow within the lung is unequal.
15 On mild exercise, both upper and lower zone blood flows increase, and the regional differences become less pronounced. The uneven distribution of blood flow is due to the hydrostatic pressure differences within the blood vessels. difference in pressure between the top and bottom- 30 cm of H 2 O This is a large pressure difference for a lowpressure system as the pulmonary circulation J Appl Physiol 15:
16 No blood flow possible. Severe hemorrhage Positive pressure ventila Alveolar dead space.
 rises as lung volume decreases due to reduced radial tethering of the")
17 Zone 4 -can be seen at the lung bases at low lung volumes or in Pulmonary oedema. Pulmonary interstitial pressure (Pi) rises as lung volume decreases due to reduced radial tethering of the lung Parenchyma Pa > Pi > Pv > PA
18

19 Shunt blood that enters the arterial system without going through ventilated areas of the lung. Physiological thebesian veins Bronchial veins Pathological Intracardiac A-V malformations

20 Shunt equation Q T = total blood flow Qs= shunt blood flow CvO2= O2 concentration in shunted blood Cc O2= O2 concentration in end-capillary blood CaO 2 = O 2 concentration in the arterial blood
21 a 5% shunt for every 100 mm Hg decrease in Pao2 below 700 mm Hg while the patient is breathing 100%. If Pa O2 on Fi O2 1.0 is 200, the shunt is approximately ( )* 5 ie 25 %. Pure shunt does not respond to increase in Fi O2. ARDS 25-50% shunt, responds to PEEP.
22 Ventilation-Perfusion Ratio What determines the concentration of dye? rate at which the dye is added (ventilation) rate at which water is pumped (blood flow)
23 Alterations in the Ventilation- Perfusion Ratio
24 O2-CO2 diagram
25 Regional changes in V-Q Ventilation increases slowly from top to bottom of the lung and blood flow increases more rapidly. V-Q ratio is abnormally high at the top of the lung and much lower at the bottom

26 Regional differences in gas exchange down the normal lung
27 Po2 at the apex is higher than at the base of the lung. However, the major share of the blood leaving the lung comes from the lower zones, where the Po2 is low. This depresses the arterial oxygen saturation.
28 V-Q mismatch in disease state.
29
30 Low V-Q ratio.
31
32 Units with high V-Q ratio add little oxygen to the blood, compared the decrement caused by the alveoli with the low ratio. The net result of these mechanisms is a depression of the arterial Po2 below that of the mixed alveolar Po2 alveolar-arterial O2 difference. Normal-4

33 CO2 dissociation curve is linear Although the elimination of CO2 is impaired by V/Q inequality, this can be corrected by increasing the ventilation to the alveoli.
34 Distributions of Ventilation- Perfusion Ratios All the ventilation and blood flow goes to compartments with normal V-Q ratio of 1.0. no blood flow to the unventilated compartment (shunt).
35 V-Q distribution in COPD large amount of ventilation to lung units with high V-Q ratios. Physiologic dead space excessive ventilation to high V-Q units constitute wasted ventilation. There is little blood flow to units with an abnormally low VA /Q, causing hypoxemia.
36 Increase in ventilation to high VA /Q units physiologic dead space. large amounts of blood flow to low VA /Q units physiologic shunt severe hypoxemia type B disease.
37 Hypoxic vasoconstriction Alveolar hypoxia constricts small pulmonary arteries direct effect of the low PO2 on vascular smooth muscle Directs blood flow away from poorly ventilated areas minimizing the arterial hypoxemia. Bronchodilators can abolish this mechanism and cause mild hypoxia by increasing the blood flow to poorly ventilated areas.
38 V-Q mismatch in Asthma considerable amount of the total blood flow to units with a low VA /Q mild hypoxemia
39 Bronchodilators increase the hypoxemia, by abolishing the HPV and, increasing the blood flow to lung units with low V/Q ratio s
40 V-Q mismatch in Pulmonary Edema abnormal accumulation of fluid in the extravascular spaces and tissues. severe hypoxemia results from; Shunt - > 50 % Blood flow to low V- Q areas
41
42 Pulmonary Embolism Moderate hypoxemia without carbon dioxide retention diffusion impairment opening up of latent pulmonary a-v anastomoses V-Q inequality-areas with High V-Q ratios dead space ventilation Shunting
43 blood flow is greatly reduced but not completely absent, leading to areas with high V-Q ratio s. Shunt occurs due to blood flow through the areas with hemorrhagic atelectasis, in which the alveoli are not functional.
44 The large physiological dead space in pulmonary embolism can cause hypercapnia, however the substantial increase in ventilation maintains the Paco 2 at a normal level. In the setting of acute PE, hypercapnia reflects massive embolism as the ventilatory muscles are unable to sustain the marked increase of minute ventilation needed to maintain normal arterial Paco2
45 Interstitial Pulmonary Fibrosis Basic pathology -thickening of the interstitium of the alveolar wall Spirometry -restrictive pattern Characterized by hypoxia and hypocapnia at rest. mild hypoxia at rest, worsened by exercise.
46 Cause of hypoxia? Rest V-Q Inequality Major factor during rest D.I minor factor, as lung as enormous reserves of diffusion at rest. Exercise Diffusion impairment Major factor during exercise Exercise - time for RBC S in pulmonary circulation Further worsens hypoxia V-Q Inequality Inadequate in Cardiac output ( PaO2 in mixed blood, PVR ) Inappropriately high
47 hypoxemia can be explained by the degree of VA /Q inequality at rest. Measured PaO2 below predicted in exercise! Additional hypoxemia is due to D.I
48 DL Co as a diagnostic test? Dlco is strikingly reduced in ILD Remains low in exercise, normal- 2-3 fold. Etiology- thickening of the blood gas barrier blood volume because of obliterated of blood vessels by the fibrotic process if the Dlco is not low, the diagnosis of ILDshould be regarded with suspicion.
49 Diseases of the Chest Wall Scoliosis -lateral curvature of the spine More serious kyphosis - posterior curvature. Restrictive lung disease! Hypoxemia due to : V-Q inequality Atelectasis & compression of dependent areas Airway closure
50 Hypercapnia Due to W.O.B caused by Stiff chest wall respiratory muscles operating at mechanical disadvantage reduced ventilatory response to CO2
51 Take home points! V-Q matching is required for maintaining normal PO2 and PCO2 levels in blood. V-Q mismatching is one of the most common causes of hypoxia and rarely hypercapnia in most of the lung diseases. Shunt and dead space ventilation are the two ends of the spectrum of V-Q mismatch.
Respiratory System. Prepared by: Dorota Marczuk-Krynicka, MD, PhD
 Respiratory System Prepared by: Dorota Marczuk-Krynicka, MD, PhD Lungs: Ventilation Perfusion Gas Exchange - Diffusion 1. Airways and Airway Resistance (AWR) 2. Mechanics of Breathing and Lung (Elastic)
Respiratory System Prepared by: Dorota Marczuk-Krynicka, MD, PhD Lungs: Ventilation Perfusion Gas Exchange - Diffusion 1. Airways and Airway Resistance (AWR) 2. Mechanics of Breathing and Lung (Elastic)
CHAPTER 6. Oxygen Transport. Copyright 2008 Thomson Delmar Learning
 CHAPTER 6 Oxygen Transport Normal Blood Gas Value Ranges Table 6-1 OXYGEN TRANSPORT Oxygen Dissolved in the Blood Plasma Dissolve means that the gas maintains its precise molecular structure About.003
CHAPTER 6 Oxygen Transport Normal Blood Gas Value Ranges Table 6-1 OXYGEN TRANSPORT Oxygen Dissolved in the Blood Plasma Dissolve means that the gas maintains its precise molecular structure About.003
Respiration (revised 2006) Pulmonary Mechanics
 Pulmonary Mechanics") Respiration (revised 2006) Pulmonary Mechanics PUL 1. Diagram how pleural pressure, alveolar pressure, airflow, and lung volume change during a normal quiet breathing cycle. Identify on the figure the
Respiration (revised 2006) Pulmonary Mechanics PUL 1. Diagram how pleural pressure, alveolar pressure, airflow, and lung volume change during a normal quiet breathing cycle. Identify on the figure the
Unit II Problem 4 Physiology: Diffusion of Gases and Pulmonary Circulation
 Unit II Problem 4 Physiology: Diffusion of Gases and Pulmonary Circulation - Physical principles of gases: Pressure of a gas is caused by the movement of its molecules against a surface (more concentration
Unit II Problem 4 Physiology: Diffusion of Gases and Pulmonary Circulation - Physical principles of gases: Pressure of a gas is caused by the movement of its molecules against a surface (more concentration
Pulmonary Circulation
 Pulmonary Circulation resin cast of pulmonary arteries resin cast of pulmonary veins Blood Flow to the Lungs Pulmonary Circulation Systemic Circulation Blood supply to the conducting zone provided by the
Pulmonary Circulation resin cast of pulmonary arteries resin cast of pulmonary veins Blood Flow to the Lungs Pulmonary Circulation Systemic Circulation Blood supply to the conducting zone provided by the
Lung Volumes and Capacities
 Lung Volumes and Capacities Normally the volume of air entering the lungs during a single inspiration is approximately equal to the volume leaving on the subsequent expiration and is called the tidal volume.
Lung Volumes and Capacities Normally the volume of air entering the lungs during a single inspiration is approximately equal to the volume leaving on the subsequent expiration and is called the tidal volume.
Section Two Diffusion of gases
 Section Two Diffusion of gases Lecture 5: Partial pressure and the composition of gasses in air. Factors affecting diffusion of gases. Ventilation perfusion ratio effect on alveolar gas concentration.
Section Two Diffusion of gases Lecture 5: Partial pressure and the composition of gasses in air. Factors affecting diffusion of gases. Ventilation perfusion ratio effect on alveolar gas concentration.
RESPIRATORY PHYSIOLOGY. Anaesthesiology Block 18 (GNK 586) Prof Pierre Fourie
 Prof Pierre Fourie") RESPIRATORY PHYSIOLOGY Anaesthesiology Block 18 (GNK 586) Prof Pierre Fourie Outline Ventilation Diffusion Perfusion Ventilation-Perfusion relationship Work of breathing Control of Ventilation 2 This image
RESPIRATORY PHYSIOLOGY Anaesthesiology Block 18 (GNK 586) Prof Pierre Fourie Outline Ventilation Diffusion Perfusion Ventilation-Perfusion relationship Work of breathing Control of Ventilation 2 This image
Pulmonary Circulation Linda Costanzo Ph.D.
 Pulmonary Circulation Linda Costanzo Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The differences between pressures in the pulmonary and systemic circulations. 2. How
Pulmonary Circulation Linda Costanzo Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The differences between pressures in the pulmonary and systemic circulations. 2. How
Respiratory Medicine. A-A Gradient & Alveolar Gas Equation Laboratory Diagnostics. Alveolar Gas Equation. See online here
 Respiratory Medicine A-A Gradient & Alveolar Gas Equation Laboratory Diagnostics See online here Alveolar gas equation helps to calculate the partial pressure of oxygen in alveoli and A-a gradient is the
Respiratory Medicine A-A Gradient & Alveolar Gas Equation Laboratory Diagnostics See online here Alveolar gas equation helps to calculate the partial pressure of oxygen in alveoli and A-a gradient is the
I Physical Principles of Gas Exchange
 Respiratory Gases Exchange Dr Badri Paudel, M.D. 2 I Physical Principles of Gas Exchange 3 Partial pressure The pressure exerted by each type of gas in a mixture Diffusion of gases through liquids Concentration
Respiratory Gases Exchange Dr Badri Paudel, M.D. 2 I Physical Principles of Gas Exchange 3 Partial pressure The pressure exerted by each type of gas in a mixture Diffusion of gases through liquids Concentration
Chapter 4: Ventilation Test Bank MULTIPLE CHOICE
 Instant download and all chapters Test Bank Respiratory Care Anatomy and Physiology Foundations for Clinical Practice 3rd Edition Will Beachey https://testbanklab.com/download/test-bank-respiratory-care-anatomy-physiologyfoundations-clinical-practice-3rd-edition-will-beachey/
Instant download and all chapters Test Bank Respiratory Care Anatomy and Physiology Foundations for Clinical Practice 3rd Edition Will Beachey https://testbanklab.com/download/test-bank-respiratory-care-anatomy-physiologyfoundations-clinical-practice-3rd-edition-will-beachey/
By: Aseel Jamil Al-twaijer. Lec : physical principles of gas exchange
 By: Aseel Jamil Al-twaijer Lec : physical principles of gas exchange Date:30 /10/2017 this lecture is about the exchange of gases between the blood and the alveoli. I might add some external definitions
By: Aseel Jamil Al-twaijer Lec : physical principles of gas exchange Date:30 /10/2017 this lecture is about the exchange of gases between the blood and the alveoli. I might add some external definitions
Lung Volumes and Ventilation
 Respiratory System ssrisuma@rics.bwh.harvard.edu Lung Volumes and Ventilation Minute ventilation Volume of an inspired or expired air per minute = tidal volume (V T ) x respiratory rate Dead space ventilation
Respiratory System ssrisuma@rics.bwh.harvard.edu Lung Volumes and Ventilation Minute ventilation Volume of an inspired or expired air per minute = tidal volume (V T ) x respiratory rate Dead space ventilation
Respiratory Physiology. ED Primary Teaching
 Respiratory Physiology ED Primary Teaching Functions of the respiratory system Gas exchange with O2 and CO2 Surfactant production Defence - IgA and macrophages Filer - pollutants and thromboembolism Metabolises
Respiratory Physiology ED Primary Teaching Functions of the respiratory system Gas exchange with O2 and CO2 Surfactant production Defence - IgA and macrophages Filer - pollutants and thromboembolism Metabolises
Rodney Shandukani 14/03/2012
 Rodney Shandukani 14/03/2012 OXYGEN THERAPY Aerobic metabolism accounts for 90% of Oxygen consumption by tissues. generates ATP by oxidative phosphorylation. Oxygen cascade: Oxygen exerts a partial pressure,
Rodney Shandukani 14/03/2012 OXYGEN THERAPY Aerobic metabolism accounts for 90% of Oxygen consumption by tissues. generates ATP by oxidative phosphorylation. Oxygen cascade: Oxygen exerts a partial pressure,
RESPIRATORY GAS EXCHANGE
 RESPIRATORY GAS EXCHANGE Alveolar PO 2 = 105 mmhg; Pulmonary artery PO 2 = 40 mmhg PO 2 gradient across respiratory membrane 65 mmhg (105 mmhg 40 mmhg) Results in pulmonary vein PO 2 ~100 mmhg Partial
RESPIRATORY GAS EXCHANGE Alveolar PO 2 = 105 mmhg; Pulmonary artery PO 2 = 40 mmhg PO 2 gradient across respiratory membrane 65 mmhg (105 mmhg 40 mmhg) Results in pulmonary vein PO 2 ~100 mmhg Partial
PICU Resident Self-Study Tutorial The Basic Physics of Oxygen Transport. I was told that there would be no math!
 Physiology of Oxygen Transport PICU Resident Self-Study Tutorial I was told that there would be no math! INTRODUCTION Christopher Carroll, MD Although cells rely on oxygen for aerobic metabolism and viability,
Physiology of Oxygen Transport PICU Resident Self-Study Tutorial I was told that there would be no math! INTRODUCTION Christopher Carroll, MD Although cells rely on oxygen for aerobic metabolism and viability,
Table of Contents. By Adam Hollingworth
 By Adam Hollingworth Table of Contents Oxygen Cascade... 2 Diffusion... 2 Laws of Diffusion... 2 Diffusion & Perfusion Limitations... 3 Oxygen Uptake Along Pulmon Capillary... 4 Measurement of Diffusing
By Adam Hollingworth Table of Contents Oxygen Cascade... 2 Diffusion... 2 Laws of Diffusion... 2 Diffusion & Perfusion Limitations... 3 Oxygen Uptake Along Pulmon Capillary... 4 Measurement of Diffusing
Respiratory Physiology. Adeyomoye O.I
 Respiratory Physiology By Adeyomoye O.I Outline Introduction Hypoxia Dyspnea Control of breathing Ventilation/perfusion ratios Respiratory/barometric changes in exercise Intra-pulmonary & intra-pleural
Respiratory Physiology By Adeyomoye O.I Outline Introduction Hypoxia Dyspnea Control of breathing Ventilation/perfusion ratios Respiratory/barometric changes in exercise Intra-pulmonary & intra-pleural
UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION MUST, AT ALL TIMES, ACCEPT THE ENTIRE CARDIAC OUTPUT
 UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION MUST, AT ALL TIMES, ACCEPT THE ENTIRE CARDIAC OUTPUT UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION
UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION MUST, AT ALL TIMES, ACCEPT THE ENTIRE CARDIAC OUTPUT UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION
660 mm Hg (normal, 100 mm Hg, room air) Paco, (arterial Pc02) 36 mm Hg (normal, 40 mm Hg) % saturation 50% (normal, 95%-100%)
 Paco, (arterial Pc02) 36 mm Hg (normal, 40 mm Hg) % saturation 50% (normal, 95%-100%)") 148 PHYSIOLOGY CASES AND PROBLEMS Case 26 Carbon Monoxide Poisoning Herman Neiswander is a 65-year-old retired landscape architect in northern Wisconsin. One cold January morning, he decided to warm his
148 PHYSIOLOGY CASES AND PROBLEMS Case 26 Carbon Monoxide Poisoning Herman Neiswander is a 65-year-old retired landscape architect in northern Wisconsin. One cold January morning, he decided to warm his
Capnography in the Veterinary Technician Toolbox. Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA
 Capnography in the Veterinary Technician Toolbox Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA What are Respiration and Ventilation? Respiration includes all those chemical and physical
Capnography in the Veterinary Technician Toolbox Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA What are Respiration and Ventilation? Respiration includes all those chemical and physical
4. For external respiration to occur effectively, you need three parameters. They are:
 Self Assessment Module D Name: ANSWER KEY 1. Hypoxia should be assumed whenever the PaO 2 is below 45 mm Hg. 2. Name some clinical conditions that will result in hyperventilation (respiratory alkalosis).
Self Assessment Module D Name: ANSWER KEY 1. Hypoxia should be assumed whenever the PaO 2 is below 45 mm Hg. 2. Name some clinical conditions that will result in hyperventilation (respiratory alkalosis).
Circulatory And Respiration
 Circulatory And Respiration Composition Of Blood Blood Heart 200mmHg 120mmHg Aorta Artery Arteriole 50mmHg Capillary Bed Venule Vein Vena Cava Heart Differences Between Arteries and Veins Veins transport
Circulatory And Respiration Composition Of Blood Blood Heart 200mmHg 120mmHg Aorta Artery Arteriole 50mmHg Capillary Bed Venule Vein Vena Cava Heart Differences Between Arteries and Veins Veins transport
The Physiologic Basis of DLCO testing. Brian Graham Division of Respirology, Critical Care and Sleep Medicine University of Saskatchewan
 The Physiologic Basis of DLCO testing Brian Graham Division of Respirology, Critical Care and Sleep Medicine University of Saskatchewan Objectives Review gas transport from inhaled gas to the rest of the
The Physiologic Basis of DLCO testing Brian Graham Division of Respirology, Critical Care and Sleep Medicine University of Saskatchewan Objectives Review gas transport from inhaled gas to the rest of the
Collin County Community College. Lung Physiology
 Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 9 Respiratory System 1 Lung Physiology Factors affecting Ventillation 1. Airway resistance Flow = Δ P / R Most resistance is encountered
Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 9 Respiratory System 1 Lung Physiology Factors affecting Ventillation 1. Airway resistance Flow = Δ P / R Most resistance is encountered
PROBLEM SET 9. SOLUTIONS April 23, 2004
 Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Deborah Dewaay MD Division of General Internal Medicine and Geriatrics Hospital Medicine Acknowledgment: Antine Stenbit MD
 Deborah Dewaay MD Division of General Internal Medicine and Geriatrics Hospital Medicine 2013 Acknowledgment: Antine Stenbit MD Objectives Knowledge: Understand the difference between hypoxia and hypoxemia
Deborah Dewaay MD Division of General Internal Medicine and Geriatrics Hospital Medicine 2013 Acknowledgment: Antine Stenbit MD Objectives Knowledge: Understand the difference between hypoxia and hypoxemia
Section Three Gas transport
 Section Three Gas transport Lecture 6: Oxygen transport in blood. Carbon dioxide in blood. Objectives: i. To describe the carriage of O2 in blood. ii. iii. iv. To explain the oxyhemoglobin dissociation
Section Three Gas transport Lecture 6: Oxygen transport in blood. Carbon dioxide in blood. Objectives: i. To describe the carriage of O2 in blood. ii. iii. iv. To explain the oxyhemoglobin dissociation
Respiratory System Physiology. Dr. Vedat Evren
 Respiratory System Physiology Dr. Vedat Evren Respiration Processes involved in oxygen transport from the atmosphere to the body tissues and the release and transportation of carbon dioxide produced in
Respiratory System Physiology Dr. Vedat Evren Respiration Processes involved in oxygen transport from the atmosphere to the body tissues and the release and transportation of carbon dioxide produced in
Blood gas adventures at various altitudes. Friedrich Luft Experimental and Clinical Research Center, Berlin-Buch
 Blood gas adventures at various altitudes Friedrich Luft Experimental and Clinical Research Center, Berlin-Buch Mount Everest 8848 M Any point in bird watching here? Respiration is gas exchange: the process
Blood gas adventures at various altitudes Friedrich Luft Experimental and Clinical Research Center, Berlin-Buch Mount Everest 8848 M Any point in bird watching here? Respiration is gas exchange: the process
exchange of carbon dioxide and of oxygen between the blood and the air in
 M. M. HENRY WILLIAMS, JR.*Cardiorespiratory Laboratory, Grasslands WILLIAMS, JR.* Hospital, Valhalla, New York SOME APPLICATIONS OF PULMONARY PHYSIOLOGY TO CLINICAL MEDICINE During the past ten years a
M. M. HENRY WILLIAMS, JR.*Cardiorespiratory Laboratory, Grasslands WILLIAMS, JR.* Hospital, Valhalla, New York SOME APPLICATIONS OF PULMONARY PHYSIOLOGY TO CLINICAL MEDICINE During the past ten years a
Gas exchange and ventilation perfusion relationships in the lung
 ERJ Express. Published on July 28, 214 as doi: 1.1183/931936.3714 REVIEW IN PRESS CORRECTED PROOF Gas exchange and ventilation perfusion relationships in the lung Johan Petersson 1,2 and Robb W. Glenny
ERJ Express. Published on July 28, 214 as doi: 1.1183/931936.3714 REVIEW IN PRESS CORRECTED PROOF Gas exchange and ventilation perfusion relationships in the lung Johan Petersson 1,2 and Robb W. Glenny
Chapter 13 The Respiratory System
 Chapter 13 The Respiratory System by Dr. Jay M. Templin Brooks/Cole - Thomson Learning Atmosphere Tissue cell External respiration Alveoli of lungs 1 Ventilation or gas exchange between the atmosphere
Chapter 13 The Respiratory System by Dr. Jay M. Templin Brooks/Cole - Thomson Learning Atmosphere Tissue cell External respiration Alveoli of lungs 1 Ventilation or gas exchange between the atmosphere
Respiratory physiology II.
 Respiratory physiology II. Learning objectives: 29. Pulmonary gas exchange. 30. Oxygen transport in the blood. 31. Carbon-dioxide transport in the blood. 1 Pulmonary gas exchange The transport mechanism
Respiratory physiology II. Learning objectives: 29. Pulmonary gas exchange. 30. Oxygen transport in the blood. 31. Carbon-dioxide transport in the blood. 1 Pulmonary gas exchange The transport mechanism
Gas exchange. Tissue cells CO2 CO 2 O 2. Pulmonary capillary. Tissue capillaries
 Gas exchange Pulmonary gas exchange Tissue gas exchange CO 2 O 2 O 2 Tissue cells CO2 CO 2 Pulmonary capillary O 2 O 2 CO 2 Tissue capillaries Physical principles of gas exchange Diffusion: continuous
Gas exchange Pulmonary gas exchange Tissue gas exchange CO 2 O 2 O 2 Tissue cells CO2 CO 2 Pulmonary capillary O 2 O 2 CO 2 Tissue capillaries Physical principles of gas exchange Diffusion: continuous
Alveolus and Respiratory Membrane
 Alveolus and Respiratory Membrane thin membrane where gas exchange occurs in the lungs, simple squamous epithelium (Squamous cells have the appearance of thin, flat plates. They fit closely together in
Alveolus and Respiratory Membrane thin membrane where gas exchange occurs in the lungs, simple squamous epithelium (Squamous cells have the appearance of thin, flat plates. They fit closely together in
Physical Chemistry of Gases: Gas Exchange Linda Costanzo, Ph.D.
 Physical Chemistry of Gases: Gas Exchange Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. Application of the gas laws to pulmonary physiology. 2. How to
Physical Chemistry of Gases: Gas Exchange Linda Costanzo, Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. Application of the gas laws to pulmonary physiology. 2. How to
EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES
 GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation.
, Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation.") Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation. Paradoxical breathing Hyper-resonance on percussion:
Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation. Paradoxical breathing Hyper-resonance on percussion:
Respiratory System. Part 2
 Respiratory System Part 2 Respiration Exchange of gases between air and body cells Three steps 1. Ventilation 2. External respiration 3. Internal respiration Ventilation Pulmonary ventilation consists
Respiratory System Part 2 Respiration Exchange of gases between air and body cells Three steps 1. Ventilation 2. External respiration 3. Internal respiration Ventilation Pulmonary ventilation consists
- How do the carotid bodies sense arterial blood gases? o The carotid bodies weigh 25mg, yet they have their own artery. This means that they have
 - How do the carotid bodies sense arterial blood gases? o The carotid bodies weigh 25mg, yet they have their own artery. This means that they have the highest blood flow of all organs, which makes them
- How do the carotid bodies sense arterial blood gases? o The carotid bodies weigh 25mg, yet they have their own artery. This means that they have the highest blood flow of all organs, which makes them
For more information about how to cite these materials visit
 Author(s): John G. Younger, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Author(s): John G. Younger, M.D., 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike 3.0 License: http://creativecommons.org/licenses/by-sa/3.0/
Respiratory Anatomy and Physiology. Respiratory Anatomy. Function of the Respiratory System
 Respiratory Anatomy and Physiology Michaela Dixon Clinical Development Nurse PICU BRHFC Respiratory Anatomy Function of the Respiratory System - In conjunction with the cardiovascular system, to supply
Respiratory Anatomy and Physiology Michaela Dixon Clinical Development Nurse PICU BRHFC Respiratory Anatomy Function of the Respiratory System - In conjunction with the cardiovascular system, to supply
Physiological Basis of Mechanical Ventilation
 Physiological Basis of Mechanical Ventilation Wally Carlo, M.D. University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu Fine Tuning Mechanical Ventilation
Physiological Basis of Mechanical Ventilation Wally Carlo, M.D. University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu Fine Tuning Mechanical Ventilation
Respiration - Human 1
 Respiration - Human 1 At the end of the lectures on respiration you should be able to, 1. Describe events in the respiratory processes 2. Discuss the mechanism of lung ventilation in human 3. Discuss the
Respiration - Human 1 At the end of the lectures on respiration you should be able to, 1. Describe events in the respiratory processes 2. Discuss the mechanism of lung ventilation in human 3. Discuss the
Introduction. Respiration. Chapter 10. Objectives. Objectives. The Respiratory System
 Introduction Respiration Chapter 10 The Respiratory System Provides a means of gas exchange between the environment and the body Plays a role in the regulation of acidbase balance during exercise Objectives
Introduction Respiration Chapter 10 The Respiratory System Provides a means of gas exchange between the environment and the body Plays a role in the regulation of acidbase balance during exercise Objectives
Physiology Unit 4 RESPIRATORY PHYSIOLOGY
 Physiology Unit 4 RESPIRATORY PHYSIOLOGY In Physiology Today Respiration External respiration ventilation gas exchange Internal respiration cellular respiration gas exchange Respiratory Cycle Inspiration
Physiology Unit 4 RESPIRATORY PHYSIOLOGY In Physiology Today Respiration External respiration ventilation gas exchange Internal respiration cellular respiration gas exchange Respiratory Cycle Inspiration
Diffusion. Dr. Gyanendra Agrawal Senior Resident Deptt. of Pulmonary Medicine PGIMER, Chandigarh
 Diffusion Dr. Gyanendra Agrawal Senior Resident Deptt. of Pulmonary Medicine PGIMER, Chandigarh Diffusion Primary function of lung gas exchange Movement of gas across the blood gas interface is by simple
Diffusion Dr. Gyanendra Agrawal Senior Resident Deptt. of Pulmonary Medicine PGIMER, Chandigarh Diffusion Primary function of lung gas exchange Movement of gas across the blood gas interface is by simple
2. State the volume of air remaining in the lungs after a normal breathing.
 CLASS XI BIOLOGY Breathing And Exchange of Gases 1. Define vital capacity. What is its significance? Answer: Vital Capacity (VC): The maximum volume of air a person can breathe in after a forced expiration.
CLASS XI BIOLOGY Breathing And Exchange of Gases 1. Define vital capacity. What is its significance? Answer: Vital Capacity (VC): The maximum volume of air a person can breathe in after a forced expiration.
medical physiology :: Pulmonary Physiology in a Nutshell by:
 medical physiology :: Pulmonary Physiology in a Nutshell by: Johan H Koeslag Medical Physiology Stellenbosch University PO Box 19063 Tygerberg, 7505. South Africa Mail me INTRODUCTION The lungs are not
medical physiology :: Pulmonary Physiology in a Nutshell by: Johan H Koeslag Medical Physiology Stellenbosch University PO Box 19063 Tygerberg, 7505. South Africa Mail me INTRODUCTION The lungs are not
RESPIRATORY REGULATION DURING EXERCISE
 RESPIRATORY REGULATION DURING EXERCISE Respiration Respiration delivery of oxygen to and removal of carbon dioxide from the tissue External respiration ventilation and exchange of gases in the lung Internal
RESPIRATORY REGULATION DURING EXERCISE Respiration Respiration delivery of oxygen to and removal of carbon dioxide from the tissue External respiration ventilation and exchange of gases in the lung Internal
Indications for Mechanical Ventilation. Mechanical Ventilation. Indications for Mechanical Ventilation. Modes. Modes: Volume cycled
 Mechanical Ventilation Eric A. Libré, MD VCU School of Medicine Inova Fairfax Hospital and VHC Indications for Mechanical Ventilation Inadequate ventilatory effort Rising pco2 with resp acidosis (7.25)
Mechanical Ventilation Eric A. Libré, MD VCU School of Medicine Inova Fairfax Hospital and VHC Indications for Mechanical Ventilation Inadequate ventilatory effort Rising pco2 with resp acidosis (7.25)
AIIMS, New Delhi. Dr. K. K. Deepak, Prof. & HOD, Physiology AIIMS, New Delhi Dr. Geetanjali Bade, Asst. Professor AIIMS, New Delhi
 Course : PG Pathshala-Biophysics Paper 13 : Physiological Biophysics Module 17 : Gas transport and pulmonary circulation Principal Investigator: Co-Principal Investigator: Paper Coordinator: Content Writer:
Course : PG Pathshala-Biophysics Paper 13 : Physiological Biophysics Module 17 : Gas transport and pulmonary circulation Principal Investigator: Co-Principal Investigator: Paper Coordinator: Content Writer:
Recitation question # 05
 Recitation and Lab # 05 The goal of this recitations / labs is to review material related to the CV and respiratory lectures for the second test of this course. Info required to answer this recitation
Recitation and Lab # 05 The goal of this recitations / labs is to review material related to the CV and respiratory lectures for the second test of this course. Info required to answer this recitation
The physiological basis of pulmonary gas exchange: implications for clinical interpretation of arterial blood gases
 ERJ Express. Published on October 16, 214 as doi: 1.1183/931936.39214 REVIEW IN PRESS CORRECTED PROOF The physiological basis of pulmonary gas exchange: implications for clinical interpretation of arterial
ERJ Express. Published on October 16, 214 as doi: 1.1183/931936.39214 REVIEW IN PRESS CORRECTED PROOF The physiological basis of pulmonary gas exchange: implications for clinical interpretation of arterial
 Question 1: Define vital capacity. What is its significance? Vital capacity is the maximum volume of air that can be exhaled after a maximum inspiration. It is about 3.5 4.5 litres in the human body. It
Question 1: Define vital capacity. What is its significance? Vital capacity is the maximum volume of air that can be exhaled after a maximum inspiration. It is about 3.5 4.5 litres in the human body. It
Control of Respiration. Central Control of Ventilation
 Central Control of Goal: maintain sufficient ventilation with minimal energy Process steps: mechanics + aerodynamics Points of Regulation Breathing rate and depth, coughing, swallowing, breath holding
Central Control of Goal: maintain sufficient ventilation with minimal energy Process steps: mechanics + aerodynamics Points of Regulation Breathing rate and depth, coughing, swallowing, breath holding
Respiratory Pulmonary Ventilation
 Respiratory Pulmonary Ventilation Pulmonary Ventilation Pulmonary ventilation is the act of breathing and the first step in the respiratory process. Pulmonary ventilation brings in air with a new supply
Respiratory Pulmonary Ventilation Pulmonary Ventilation Pulmonary ventilation is the act of breathing and the first step in the respiratory process. Pulmonary ventilation brings in air with a new supply
Chapter 37: Pulmonary Ventilation. Chad & Angela
 Chapter 37: Pulmonary Ventilation Chad & Angela Respiratory Structures Basic Structures of Respiration Nasal/Oral Cavities Larynx Trachea Bronchi Secondary Bronchi Bronchioles Alveoli Mechanics of Ventilation
Chapter 37: Pulmonary Ventilation Chad & Angela Respiratory Structures Basic Structures of Respiration Nasal/Oral Cavities Larynx Trachea Bronchi Secondary Bronchi Bronchioles Alveoli Mechanics of Ventilation
Exam Key. NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: % of grade in class
 NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: 100 20% of grade in class 1) An arterial blood sample for a patient at sea level is obtained, and the following physiological values
NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: 100 20% of grade in class 1) An arterial blood sample for a patient at sea level is obtained, and the following physiological values
How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital. Synopsis
 How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital Synopsis Definition of an oscillator Historical perspective Differences between HFOV and CMV Determinants
How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital Synopsis Definition of an oscillator Historical perspective Differences between HFOV and CMV Determinants
Chapter 17 The Respiratory System: Gas Exchange and Regulation of Breathing
 Chapter 17 The Respiratory System: Gas Exchange and Regulation of Breathing Overview of Pulmonary Circulation o Diffusion of Gases o Exchange of Oxygen and Carbon Dioxide o Transport of Gases in the Blood
Chapter 17 The Respiratory System: Gas Exchange and Regulation of Breathing Overview of Pulmonary Circulation o Diffusion of Gases o Exchange of Oxygen and Carbon Dioxide o Transport of Gases in the Blood
Respiratory system & exercise. Dr. Rehab F Gwada
 Respiratory system & exercise Dr. Rehab F Gwada Objectives of lecture Outline the major anatomical components & important functions of the respiratory system. Describe the mechanics of ventilation. List
Respiratory system & exercise Dr. Rehab F Gwada Objectives of lecture Outline the major anatomical components & important functions of the respiratory system. Describe the mechanics of ventilation. List
CARBON DIOXIDE METABOLISM AND CAPNOGRAPHY
 CARBON DIOXIDE METABOLISM AND CAPNOGRAPHY CARBON DIOXIDE METABOLISM Production Transportation Elimination Carbon Dioxide production CO 2 is the metabolite produced by the utilization by cells of oxygen
CARBON DIOXIDE METABOLISM AND CAPNOGRAPHY CARBON DIOXIDE METABOLISM Production Transportation Elimination Carbon Dioxide production CO 2 is the metabolite produced by the utilization by cells of oxygen
RSPT 1060 OBJECTIVES OBJECTIVES OBJECTIVES EQUATION OF MOTION. MODULE C Applied Physics Lesson #1 - Mechanics. Ventilation vs.
 RSPT 1060 MODULE C Applied Physics Lesson #1 - Mechanics OBJECTIVES At the end of this module, the student should be able to define the terms and abbreviations used in the module. draw & explain the equation
RSPT 1060 MODULE C Applied Physics Lesson #1 - Mechanics OBJECTIVES At the end of this module, the student should be able to define the terms and abbreviations used in the module. draw & explain the equation
Physiology (3) Pulmonary Function Test:
 Pulmonary Function Test:") Pulmonary Function Test: Today we will continue with the pulmonary function test, and the question is: why do we do pulmonary function tests for patients? Can pulmonary function tests tell us what type
Pulmonary Function Test: Today we will continue with the pulmonary function test, and the question is: why do we do pulmonary function tests for patients? Can pulmonary function tests tell us what type
DOWNLOAD OR READ : VENTILATION BLOOD FLOW AND DIFFUSION PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : VENTILATION BLOOD FLOW AND DIFFUSION PDF EBOOK EPUB MOBI Page 1 Page 2 ventilation blood flow and diffusion ventilation blood flow and pdf ventilation blood flow and diffusion Title:
DOWNLOAD OR READ : VENTILATION BLOOD FLOW AND DIFFUSION PDF EBOOK EPUB MOBI Page 1 Page 2 ventilation blood flow and diffusion ventilation blood flow and pdf ventilation blood flow and diffusion Title:
Chapter 13 The Respiratory System
 VI edit Pag 451-499 Chapter 13 The Respiratory System V edit. Pag 459-509 Tissue cell Alveoli of lungs Atmosphere 1 External respiration Ventilation or gas exchange between the atmosphere and air sacs
VI edit Pag 451-499 Chapter 13 The Respiratory System V edit. Pag 459-509 Tissue cell Alveoli of lungs Atmosphere 1 External respiration Ventilation or gas exchange between the atmosphere and air sacs
ALVEOLAR - BLOOD GAS EXCHANGE 1
 ALVEOLAR - BLOOD GAS EXCHANGE 1 Summary: These notes examine the general means by which ventilation is regulated in terrestrial mammals. It then moves on to a discussion of what happens when someone over
ALVEOLAR - BLOOD GAS EXCHANGE 1 Summary: These notes examine the general means by which ventilation is regulated in terrestrial mammals. It then moves on to a discussion of what happens when someone over
CHAPTER 3: The respiratory system
 CHAPTER 3: The respiratory system Practice questions - text book pages 56-58 1) When the inspiratory muscles contract, which one of the following statements is true? a. the size of the thoracic cavity
CHAPTER 3: The respiratory system Practice questions - text book pages 56-58 1) When the inspiratory muscles contract, which one of the following statements is true? a. the size of the thoracic cavity
PART ONE CHAPTER ONE PRIMARY CONSIDERATIONS RELATING TO THE PHYSIOLOGICAL AND PHYSICAL ASPECTS OF THE MECHANICAL VENTILATION OF THE LUNG
 PART ONE CHAPTER ONE PRIMARY CONSIDERATIONS RELATING TO THE PHYSIOLOGICAL AND PHYSICAL ASPECTS OF THE MECHANICAL VENTILATION OF THE LUNG POSSIBLE ORIGIN OF THE MECHANICAL VENTILATION OF THE LUNG- The first
PART ONE CHAPTER ONE PRIMARY CONSIDERATIONS RELATING TO THE PHYSIOLOGICAL AND PHYSICAL ASPECTS OF THE MECHANICAL VENTILATION OF THE LUNG POSSIBLE ORIGIN OF THE MECHANICAL VENTILATION OF THE LUNG- The first
GAS EXCHANGE & PHYSIOLOGY
 GAS EXCHANGE & PHYSIOLOGY Atmospheric Pressure Intra-Alveolar Pressure Inspiration 760 mm HG at Sea Level (= 1 atm) Pressure due to gases (N2, O2, CO2, Misc.) Pressure inside the alveolus (air sac) Phrenic
GAS EXCHANGE & PHYSIOLOGY Atmospheric Pressure Intra-Alveolar Pressure Inspiration 760 mm HG at Sea Level (= 1 atm) Pressure due to gases (N2, O2, CO2, Misc.) Pressure inside the alveolus (air sac) Phrenic
Oxygen and Carbon dioxide Transport. Dr. Laila Al-Dokhi
 Oxygen and Carbon dioxide Transport Dr. Laila Al-Dokhi Objectives 1. Understand the forms of oxygen transport in the blood, the importance of each. 2. Differentiate between O2 capacity, O2 content and
Oxygen and Carbon dioxide Transport Dr. Laila Al-Dokhi Objectives 1. Understand the forms of oxygen transport in the blood, the importance of each. 2. Differentiate between O2 capacity, O2 content and
Vienna, Austria May 2005 MONITORING GAS EXCHANGE: FROM THEORY TO CLINICAL APPLICATION
 EUROANESTHESIA 2005 Vienna, Austria 28-31 May 2005 MONITORING GAS EXCHANGE: FROM THEORY TO CLINICAL APPLICATION 5RC2 OLA STENQVIST Department of Anaesthesia and Intensive Care Sahlgrenska University Hospital
EUROANESTHESIA 2005 Vienna, Austria 28-31 May 2005 MONITORING GAS EXCHANGE: FROM THEORY TO CLINICAL APPLICATION 5RC2 OLA STENQVIST Department of Anaesthesia and Intensive Care Sahlgrenska University Hospital
Module Two. Objectives: Objectives cont. Objectives cont. Objectives cont.
 Transition to the New National EMS Education Standards: EMT-B B to EMT Module Two Objectives: Upon completion, each participant will do the following to a degree of accuracy that meets the Ntl EMS Education
Transition to the New National EMS Education Standards: EMT-B B to EMT Module Two Objectives: Upon completion, each participant will do the following to a degree of accuracy that meets the Ntl EMS Education
Accumulation of EEV Barotrauma Affect hemodynamic Hypoxemia Hypercapnia Increase WOB Unable to trigger MV
 Complicated cases during mechanical ventilation Pongdhep Theerawit M.D. Pulmonary and Critical Care Division Ramathibodi Hospital Case I Presentation Male COPD 50 YO, respiratory failure, on mechanical
Complicated cases during mechanical ventilation Pongdhep Theerawit M.D. Pulmonary and Critical Care Division Ramathibodi Hospital Case I Presentation Male COPD 50 YO, respiratory failure, on mechanical
Fysiologie van de ademhaling - gasuitwisseling
 What you will learn in this lecture... Lessenreeks co s 014-015 Fysiologie van de ademhaling - gasuitwisseling Professor Dr. Steffen Rex Department of Anesthesiology University Hospitals Leuven Department
What you will learn in this lecture... Lessenreeks co s 014-015 Fysiologie van de ademhaling - gasuitwisseling Professor Dr. Steffen Rex Department of Anesthesiology University Hospitals Leuven Department
The Safe Use and Prescription of Medical Oxygen. Luke Howard
 The Safe Use and Prescription of Medical Oxygen Luke Howard Consultant Respiratory Physician Imperial College Healthcare NHS Trust & Co-Chair, British Thoracic Society Emergency Oxygen Guideline Group
The Safe Use and Prescription of Medical Oxygen Luke Howard Consultant Respiratory Physician Imperial College Healthcare NHS Trust & Co-Chair, British Thoracic Society Emergency Oxygen Guideline Group
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo
 Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: % of grade in class
 NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: 100 20% of grade in class 1) An arterial blood sample for a patient at sea level is obtained, and the following physiological values
NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: 100 20% of grade in class 1) An arterial blood sample for a patient at sea level is obtained, and the following physiological values
Respiratory System Study Guide, Chapter 16
 Part I. Clinical Applications Name: Respiratory System Study Guide, Chapter 16 Lab Day/Time: 1. A person with ketoacidosis may hyperventilate. Explain why this occurs, and explain why this hyperventilation
Part I. Clinical Applications Name: Respiratory System Study Guide, Chapter 16 Lab Day/Time: 1. A person with ketoacidosis may hyperventilate. Explain why this occurs, and explain why this hyperventilation
Respiratory Physiology Gaseous Exchange
 Respiratory Physiology Gaseous Exchange Session Objectives. What you will cover Basic anatomy of the lung including airways Breathing movements Lung volumes and capacities Compliance and Resistance in
Respiratory Physiology Gaseous Exchange Session Objectives. What you will cover Basic anatomy of the lung including airways Breathing movements Lung volumes and capacities Compliance and Resistance in
1.2 The structure and functions of the cardio-respiratory system Learning objectives
 1.2 The structure and functions of the cardio-respiratory system Learning objectives To understand the functions of the circulatory system. To be able to identify the differences between veins, arteries
1.2 The structure and functions of the cardio-respiratory system Learning objectives To understand the functions of the circulatory system. To be able to identify the differences between veins, arteries
Ch 16: Respiratory System
 Ch 16: Respiratory System SLOs: Explain how intrapulmonary pressures change during breathing Explain surface tension and the role of surfactant in respiratory physiology. Compare and contrast compliance
Ch 16: Respiratory System SLOs: Explain how intrapulmonary pressures change during breathing Explain surface tension and the role of surfactant in respiratory physiology. Compare and contrast compliance
CHAPTER 3: The cardio-respiratory system
 : The cardio-respiratory system Exam style questions - text book pages 44-45 1) Describe the structures involved in gaseous exchange in the lungs and explain how gaseous exchange occurs within this tissue.
: The cardio-respiratory system Exam style questions - text book pages 44-45 1) Describe the structures involved in gaseous exchange in the lungs and explain how gaseous exchange occurs within this tissue.
82 Respiratory Tract NOTES
 82 Respiratory Tract NOTES RESPIRATORY TRACT The respiratory tract conducts air to the lungs where gaseous exchange occurs. It is separated into air-conducting and respiratory (where gas exchange occurs)
82 Respiratory Tract NOTES RESPIRATORY TRACT The respiratory tract conducts air to the lungs where gaseous exchange occurs. It is separated into air-conducting and respiratory (where gas exchange occurs)
Let s talk about Capnography
 Let s talk about Capnography This is one of a series of articles by Keith Simpson BVSc MRCVS MIET (Electronics) discussing the practical aspects of some common monitoring techniques. Capnometry is the
Let s talk about Capnography This is one of a series of articles by Keith Simpson BVSc MRCVS MIET (Electronics) discussing the practical aspects of some common monitoring techniques. Capnometry is the
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES
 INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES") INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
Regulation of Ventilation, Ventilation/ Perfusion Ratio, and Transport of Gases
 M07_LIMM3516_01_SE_C07.indd Page 37 1/28/11 4:38 PM user-s146 Standard Pathophysiology TOPIC Competency Applies fundamental knowledge of the pathophysiology of respiration and perfusion to patient assessment
M07_LIMM3516_01_SE_C07.indd Page 37 1/28/11 4:38 PM user-s146 Standard Pathophysiology TOPIC Competency Applies fundamental knowledge of the pathophysiology of respiration and perfusion to patient assessment
Initiation and Management of Airway Pressure Release Ventilation (APRV)
") Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Office. Hypoxia. Or this. Or even this. Hypoxia E-1. COL Brian W. Smalley DO, MSPH, CPE
 Hypoxia Office COL Brian W. Smalley DO, MSPH, CPE Or this Or even this Hypoxia State of oxygen deficiency in the blood cells and tissues sufficient to cause impairment of function 4 Types Hypoxic Hypemic
Hypoxia Office COL Brian W. Smalley DO, MSPH, CPE Or this Or even this Hypoxia State of oxygen deficiency in the blood cells and tissues sufficient to cause impairment of function 4 Types Hypoxic Hypemic
Chapter 23. Gas Exchange and Transportation
 Chapter 23 Gas Exchange and Transportation What is air? Mixture of gasses 78.6 % nitrogen 20.9% oxygen 0.04% carbon dioxide 0 4% water vapor depending on temperature and humidity and minor gases argon,
Chapter 23 Gas Exchange and Transportation What is air? Mixture of gasses 78.6 % nitrogen 20.9% oxygen 0.04% carbon dioxide 0 4% water vapor depending on temperature and humidity and minor gases argon,
Respiratory Physiology
 chapter 4 Respiratory Physiology I. LUNG VOLUMES AND CAPACITIES A. Lung volumes (Figure 4-1) 1. Tidal volume (TV) is the volume inspired or expired with each normal breath. 2. Inspiratory reserve volume
chapter 4 Respiratory Physiology I. LUNG VOLUMES AND CAPACITIES A. Lung volumes (Figure 4-1) 1. Tidal volume (TV) is the volume inspired or expired with each normal breath. 2. Inspiratory reserve volume
Anatomy and Physiology Part 11: Of Blood and Breath by: Les Sellnow
 Anatomy and Physiology Part 11: Of Blood and Breath by: Les Sellnow There are few similarities between horses and automobiles, but in a manner of speaking, the horse's circulatory and respiratory systems
Anatomy and Physiology Part 11: Of Blood and Breath by: Les Sellnow There are few similarities between horses and automobiles, but in a manner of speaking, the horse's circulatory and respiratory systems
GENETIC INFLUENCE ON FACTORS OF OXYGEN TRANSPORT
 GENETIC INFLUENCE ON FACTORS OF OXYGEN TRANSPORT Claudio Marconi IBFM-Sect. of Muscle Physiology and Proteome National Research Council Milano, Italy 100 90 80 % s.l. VO 2 max. 70 60 50 40 30 20 10 0 2
GENETIC INFLUENCE ON FACTORS OF OXYGEN TRANSPORT Claudio Marconi IBFM-Sect. of Muscle Physiology and Proteome National Research Council Milano, Italy 100 90 80 % s.l. VO 2 max. 70 60 50 40 30 20 10 0 2
Chapter 23. Gas Exchange and Transportation
 Chapter 23 Gas Exchange and Transportation What is air? Mixture of gasses 78.6 % nitrogen 20.9% oxygen 0.04% carbon dioxide 0 4% water vapor depending on temperature and humidity other minor gases argon,
Chapter 23 Gas Exchange and Transportation What is air? Mixture of gasses 78.6 % nitrogen 20.9% oxygen 0.04% carbon dioxide 0 4% water vapor depending on temperature and humidity other minor gases argon,
birth: a transition better guidelines better outcomes the birth experience a challenging transition the fountains of life: 2/8/2018
 better guidelines better outcomes neonatal resuscitation Anne G. Wlodaver, MD neonatology OU medical center the birth experience a challenging transition birth requires major and sudden transitions some
better guidelines better outcomes neonatal resuscitation Anne G. Wlodaver, MD neonatology OU medical center the birth experience a challenging transition birth requires major and sudden transitions some
ONLINE DATA SUPPLEMENT. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg
 APPENDIX 1 Appendix 1. Complete respiratory protocol. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg predicted body weight (PBW)) (NEJM 2000; 342
APPENDIX 1 Appendix 1. Complete respiratory protocol. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg predicted body weight (PBW)) (NEJM 2000; 342