4/1/2017 Inhalation NEGATIVE Exhalation:
|
|
|
- Hester Sutton
- 6 years ago
- Views:
Transcription


1 1



2 Inhalation Active process Diaphragm and intercostal muscles contract to increase thoracic volume vertically creating a NEGATIVE change in thoracic pressure. At end inhalation alveolar pressure equalizes with atmospheric pressure (approximately 0 cmh2o) Exhalation: Passive process Lungs recoil, thoracic volume decreases. At end exhalation alveolar & interstitial pressures return to atmospheric (approximately 0 cmh2o) 2
 Respiratory Rhythm Generator in VCC interacts with: Chemoreceptors")
 Located in thorax and ventilatory muscles Ultimate ventilatory")

3 2013 Gilstrap AJRCCM Spontaneous ventilatory pattern (Vt, Rate & I:E) is controlled by the brainstem Ventilatory Control Center (VCC) Respiratory Rhythm Generator in VCC interacts with: Chemoreceptors (PO2, PCO2 & ph receptors) Located in great vessels and 4 th ventricle of brain Mechanoreceptors (stretch and irritant receptors) Located in thorax and ventilatory muscles Ultimate ventilatory pattern generated by VCC: Adequate gas exchange Least amount of ventilatory muscle loading Least amount of air trapping Just what is it that is delivered by the ventilator to the patients lungs? Volume Flow Pressure 3
4 Physics of positive-pressure ventilation differs radically from those of spontaneous ventilation. During inhalation: Positive intra-thoracic pressures Flow distributed heterogeneously throughout the lung Effectively distributed through compliantlung Attenuated in low-compliant areas Inspiratory flow heterogenicity can result in: Over-distension of compliant healthy lung Under-distension of non-compliant injured lung 2013 Gilstrap AJRCCM Muscle loading inherent in mechanical ventilation can effect the VCC: Delayed or missed triggers Uncomfortable isometric load Increased inspiratory effort intensity Increased muscle loading during inhalation Spontaneous breathing pattern changes to reduce this increased load Rapid, shallow breathing Dyspnea Overdistension (mechanoreceptors) Shortening of neural Ti Activation of expiratory muscles 4
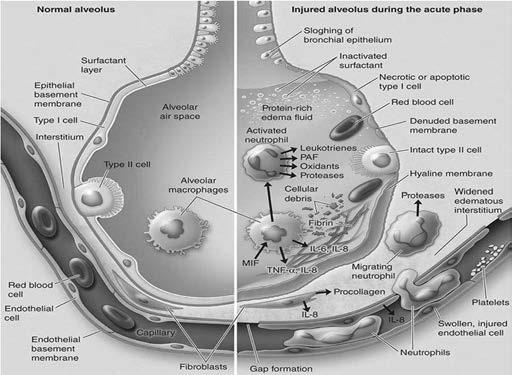
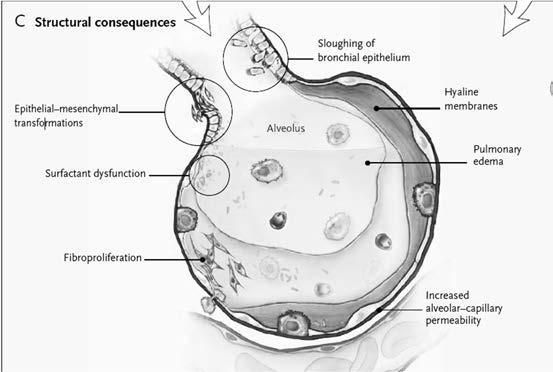
5 2013 Biehl Respiratory Care Results from injury to the blood-gas barrier in the lung Caused by mechanical ventilation Initial stretch of blood-gas barrier Disruption of pores in the endothelium Leakage of protein into the interstitial space Subsequent stretch of blood-gas barrier Membrane stress insult/failure Disruption of endothelium & alveolar epithelium Leakage of protein into alveolar space 1998 Dreyfuss AJRCCM 2013 Biehl Respiratory Care Duration of exposure <24 h in large mammals Intensity of exposure Vt Too high membrane strain/volutrauma FRC and the size of the available lung Baby lung PEEP Amount needed is influenced by prior recruitment and chest-wall compliance 5
6 1998 Dreyfuss AJRCCM 2013 Biehl Respiratory Care Heterogeneity of Flow Distribution: Atelectasis Consolidation Edema End-inspiratory lung volume (FRC) Too low promotes derecruitment Too high promotes overdistension Inspiratory flow and flow profile (strain rate) Too high = risk of VILI 1998 Dreyfuss AJRCCM 2013 Biehl Respiratory Care Breathing frequency Low RR = risk of VILI RR must be adequate to meet patient demand Most patients in ARF require bpm to meet metabolic needs Vascular pressures Higher transpulmonary pressures promotes higher hydrostatic pressures risk of pulmonary edema 6
7 1998 Dreyfuss AJRCCM 2013 Biehl Respiratory Care The First Hit suscep bility to second hit of VILI Endotoxin/sepsis Tissue injury Fluid/transfusion 1744 Fothergill: May be the earliest description of ventilator-induced lung injury Described the mouth-to-mouth resuscitation of a coal miner The lungs of one may bear, without injury, as great a force as those of another man can exert; which by the bellows cannot always be determined Lassen -Lancet: Copenhagen polio outbreak Several problems with positive-pressure ventilation identified: When bag ventilation is administered for weeks there is a risk of emphysema The weaning period from positive-pressure ventilation is not infrequently difficult 18 7


8 1967 Nash NEJM Postmortem of patients who had undergone mechanical ventilation revealed alveolar infiltrates and hyaline membranes The term Respirator Lung coined 1970 Mead J ApplPhysiol In mechanical ventilation, by applying high transpulmonary pressures to heterogeneously expanded lungs could contribute to the development of lung hemorhage and hyaline membranes Pontoppidian NEJM ARDS patients experienced discomfort when using small Vt s. Beginning of the practice of using Vt sin the ml/kg range 19 For decades Barotrauma was considered as the major cause of VILI It was accepted that as long as Peak Inspiratory Pressures were maintained in the safe range the lungs were protected from injury In the 1980 s and 1990 s further research identified the more subtle effects of VILI: Volutrauma Atelectrauma Oxygen Toxicity 8


 Alveolar pressures caused considerably less lung damage in the alveoli")
9 1974 -Webb & Tierney ARRD Two important concepts that were contrary to the barotrauma focus: Distending pressures & volumes above normal maximums but below that which was required for alveolar rupture still produced lung edema, surfactant abnormalities, tissue inflammation and hemorrhage. Preventing cyclical alveolar collapse & reopening could also significantly reduce the incidence of lung injury. Unfortunately, these concepts were not widely applied at the time Dreyfus ARRD Applied normal & excessive alveolar pressures to both volumelimited lungs (chests bound to prevent alveolar expansion) and volume-unlimited lungs (chests unbound with unchecked alveolar expansion) Alveolar pressures caused considerably less lung damage in the alveoli with limited expansion than in the alveoli in the unbound chest. Alveoli that do not overdistendwere unlikely to experience damage 9
10 Measured Lung Flooding factors in rodents ventilated with three different ventilatory styles: HiP/HiV High Pressure (45 cmh2o) High Volume LoP/HiV Low Pressure (neg.pres.ventilator) High Volume HiP/LoV High Pressure (45 cmh2o) Low Volume (chest strapped) Dreyfuss,DARRD 1988;137: Dreyfus ARRD High-volume mechanical ventilation leads to pulmonary edema of the permeability type 2000 Tschumperlin AJRCCM Limiting Vt reduces injury of alveolar epithelium Large cyclic increases in alveolar surface area are much more damaging than static increases in alveolar surface area Alveolar epithelial viability is not adversely affected by application of large static deformations (PEEP) Occasional deep inspirations to recruit collapsed alveoli should not have a serious negative impact on alveolar epithelial viability. 10
11 daviddarling.com 26 11

12 27 EXCESSIVE END-INSPIRATORY ALVEOLAR VOLUME IS THE MAJOR DETERMINANT OF VOLUTRAUMA. Diffuse alveolar damage at the pulmonary/capillary membrane. epithelial & microvascular permeability pulmonary edema May be indicated by excessive P PLAT May result from a combination of PEEP + Vt GOAL:Prevent excessive end-inspiratory volume Target 4-6cc/kg (may try 8cc/kg first) Slutsky, Chest,


13 CYCLICAL END-EXPIRATORY ALVEOLAR COLLAPSE/RE-EXPANSION IS THE PRIMARY DETERMINANT OF ATELECTRAUMA 2003 Bilek J ApplPhysiol Repeated cyclical recruitment/de-recruitment of small airways/lung units Abrasion of the epithelial airspace lining GOAL: Prevent end-expiratory alveolar de-recruitment Slutsky, Chest, Marini Critical Care Medicine Consensus that for the same plateau pressure minimizing the number of collapsed units at jeopardy is a key objective Lungs with extensive collapse need higher pressure to ventilate: Overstretch already open lung units Amplify tensions at the borders of open and closed lung units Promote tidal opening-closure cycles Amplified border tension & tidal opening/closure cycles: Deplete or inactivate surfactant Accentuate tissue tensions Tear delicate membranes Evoke inflammatory signaling in the endothelium & microvasculature 13
14 EXCESSIVE FIO2 IS THE PRIMARY DETERMINANT OF OXYGEN TOXICITY Excessive FiO2 Progressive alveolar damage/death secondary to generation of Reactive Oxygen Species (ROS) Formation of disruptive chemical bonds with surrounding lipids, proteins and carbohydrates Damage to cell membranes, collagen, connective tissue & DNA Alter enzymatic reactions within these tissues. Absorption atelectasis 1967 Nash NEJM Prolonged exposure to excessive FiO2 in mechanically ventilated pts: Worsens gas exchange Decreases ciliary efficacy Produces hyperoxic bronchitis and atelectasis 2012 Rachmale RespirCare Prolonged exposure to excessive FiO2 : Worse OI at 48 hrs. VLOS & ICU days May be associated with worsening lung function 14



15 EXCESSIVE TRANSPULMONARY PRESSURE ASSOCIATED WITH LUNG OVER-DISTENSION IS THE PRIMARY DETERMINANT OF BAROTRAUMA Gross tissue injury permits transfer of air into the interstitial tissues. Clinically presents as: Pneumothorax Pneumomediastinum Pneumopericardium Subcutaneous emphysema. Slutsky, Chest, 1999 BLOWING UP LUNGS BETTER 15





16 Ann Intern Med 1938, 12: The goal of Lung-Protective Ventilation is to limit VILI through the early application of strategies that: Limit alveolar over-expansion Prevent cyclical alveolar collapse/re-recruitment Prevent oxygen toxicity 16


17 LUNG PROTECTIVE VENTILATION RCT S Amato et al Brazil Stewart et al Canada Brochard et al Multinational Brower et al USA ARDSnetwork USA Villar et al Spain 29 pts: Vt < 6ml/kg, Pplat < 20cmH2O 38% Mortality 24 pts: Vt = 12ml/kg, PaCO mmhg 71% Mortality 60 pts: Vt <8ml/kg, Ppeak< 30cmH2O 50% Mortality at disch 60 pts: Vt 10-15ml/kg, Ppeak < 50cmH2O 47% Mortality at disch 58 pts: Vt 6-10ml/kg, Pplat <25-30 cmh2o 47% Mortality at 60 d 58 pts: Vt 10-15ml/kg, PaCO mmhg 38% Mortality at 60 d 26 pts: Vt 5-8ml/kg, Pplat <30 cmh2o 50% Mortality at disch 26 pts: Vt 10-12ml/kg, Pplat < cmh2o 46% Mortality at disch 432 pts: Vt 6ml/kg, Pplat <30 cmh2o 31% Mortality at disch/180 d 429 pts: Vt 12ml/kg, Pplat <50 cmh2o 40% Mortality at disch/180d 50 pts: Vt 5-8ml/kg, + 2cmH2O 32% Mortality in ICU 53 pts: Vt 9-11ml/kg, PEEP >5 cmh2o 53% Mortality in ICU What caused the different survival outcomes of the six previous RCT s? 2002 Eichacher et al AJRCCM (Meta-Analysis): Could the survival benefit of the two Low Vt RCT s be related to the larger-than-routine Vt s in the control arms? The control arms of the non-beneficial Low Vt RCT s actually had lower Pplat s than in the two beneficial arms Could the differences be related to Pplatrather than Vt? 17
18 2016 Guo Critical Care (Network Meta-Analysis) 17 RCT s with a total of 575 patients without ALI/ARDS Objective was to identify the optimal mechanical ventilation strategy : Strategy C (lower VT + higher PEEP) Highest PaO2/FiO2 ratio. Strategy B (higher VT + lower PEEP) Highest pulmonary compliance. Strategy A (lower VT + lower PEEP) Shortest length of ICU stay Strategy D (lower VT + ZEEP) Lowest P/F ratio Lowest pulmonary compliance Gattinoni Intensive Care Medicine Suggested P PLAT and Vt limits may not be safe for all ARDS patients 2008 Chiumello AJRCCM P PLAT and Vt may be inadequate in assessing lung stress and strain 2016 Borsellino Expert Review of Respiratory Medicine Potential benefit of LPV in neuro-critical patients is unclear LPV can increase intracranial pressure: Permissive hypercapnia High airway pressures during recruitment maneuvers 18


19 48 Stable Vt in the presence of varying compliance Clinician control of Minute Ventilation and CO2 clearance Inspiratory flow is Back-End loaded More gradual filling of alveoli Pre-set inspiratory flow May be less comfortable for actively breathing patients Variable airway and transpulmonary pressures. 19

20 Stable PIP in the presence of variable compliances Inspiratory Flow is Front-End loaded More rapid filling of alveoli Variable inspiratory flow, based on distending pressure The high initial flow of Pressure-Limited ventilation may be injurious May overinflate with improving compliance Higher Mean Paw may improve ventilation/perfusion matching VOLUME/PRESSURE HYBRID MODES PRVC/AUTOFLOW/VC+/APV Variable inspiratory flowof pressure-limited ventilation with a pre-set target Vt Variable PIP Less variation in Vt with varying compliance Advantages: Positive attributes of pressure-limited ventilation More consistent Vt & Ve than conventional pressure-limited Automated weaning of PIP as compliance improves and/or patient effort increases Disadvantages: Require volume-limited test breath(s) at initiation and following alarms and changes Intermittent patient effort leads to variable Vt 20
21 2003 MacIntyre- New Approaches to Mechanical Ventilatory Support Currently no evidence of benefit for any one mode. The choice of volume-or pressure-limited mode depends on which feature is required for the clinical goal. Volume-limited is preferable if CO2 clearance is of primary concern and patient comfort and lung stretch are less of an issue, Pressure-limited is preferable if volutrauma risk is high and/or patient synchrony is more of an issue than CO2 clearance. Many clinicians have a bias in favor of Pressure-Limited ventilation in patients with ALI/ARDS but supporting evidence for this choice is weak Rittayamai - Chest Systematic review & meta-analysis to determine whether pressure-control ventilation has demonstrated advantages over volume-control ventilation Outcomes included: Compliance Gas exchange Hemodynamics Work of breathing The two modes have different working principles but clinical available data do not suggest any difference in outcomes 21

22 It is against this background that intermittent mandatory ventilation (IMV) was introduced in This allowed partial ventilatory support, in which some of the minute ventilation is provided by the ventilator and the remainder is provided by the patient s respiratory muscles. In their original report, Downs et al 4 promoted several advantages for IMV: re 54 Marini et al 8 reported that inspiratory work increased progressively for both spontaneous and mandatory breaths as ventilator support was withdrawn, suggesting little adaptation to the mandatory volume-control breaths during IMV. Imsand et al 9 reported that electrical activations of the sternocleidomastoid and diaphragm were similar in successive spontaneous and mandatory breaths during SIMV. They concluded that inspiratory motor output is not regulated breath by breath but rather is constant for a given level of ventilator support. Leung et al 10 reported that the addition of PS of 10 cm H 2 O with IMV resulted in respiratory muscle unloading for both the mandatory and spontaneous breaths. The results of these studies suggest that, unlike what has been commonly taught, SIMV does not allow partitioning the work of breathing between that done by the ventilator and that done by the patient. The most common use of IMVSIMV has been 2013 Gilstrap AJRCCM IMV modes do not allow the patients Ventilatory Control Center to accurately anticipate the loading pattern of the next breath Adapting to the applied pattern of support may be more difficult to achieve 55 22

23 2015 Luo J Thor Diseases Conclusions: In patients with moderate ARDS, SIMV + PS can safely and effectively improve oxygenation, but does not decrease mortality, incidence of delirium and patient-ventilator asynchrony, dosages of analgesics and sedatives, and duration of mechanical ventilation and hospital stay. 56 Respiratory Rate Accurately measured Tidal Volume Accurately measured FiO2 Accurately measured Plateau Pressure Measured but not accurately PEEP Measured but not accurately 23
24 Respiratory Rate Accurately measured Tidal Volume Accurately measured FiO2 Accurately measured Plateau Pressure Measured but not accurately PEEP Measured but not accurately GOAL: Vt = 4-6 ml/kg IBW IBW Males: [height (inches) -60] IBW Females: [height (inches) -60] An initial Vt of 8ml/kg may be beneficial followed by subsequent reductions in Vt by 1 ml/kg at intervals 2 hours until Vt = 6ml/kg IBW. Cell death can be reduced by limiting the amplitude of alveolar deformation, even at constant peak deformations. Strategies that limit changes in Vt may limit epithelial injury Tschumerlin, Am J Respir Crti Care Med, 2000 Rocco, Curr Op Anesth, 2012 SpiethP, AJRCCM

25 2000 The ARDSNetwork-NEJM In patients with acute lung injury and the acute respiratory distress syndrome, mechanical ventilation with a lower tidal volume than is traditionally used results in decreased mortality and increases the number of days without ventilator use Volume Controlled Continuous Mandatory Ventilation Control Group Vt set at 12ml/kg IBW Vt reduced to maintain Pplat<50cmH2O Test Group Vt set at 6ml/kg IBW Vt reduced to maintain Pplat<30 cmh2o Vt increased to 8ml/kg IBW in patients with severe dyspnea Trial was stopped after enrollment of 861 patients Mortality was lower in Test Group (31% vs39.8% P=.007) Lee Chest Surgical ICU patients randomized to receive Vt of 6cc/kg or 12cc/kg Lower Vt = VLOS Lower vt= ICU days 2004 Gajic Critical Care Medicine First observational study of VILI in patients without ARDS Patients ventilated with Vt s of >12cc/kg IBW Excessive Vt identified as a risk factor for development of ARDS Odds Ratio of 1.3 for each cc above 6cc/kg IBW 25
26 2015 Ghamioush Respiratory Care Determine the optimal V T setting for each patient rather than applying the same set V T to lungs that are mildly, moderately, or severely diseased. Set V T may be a fluid value that varies with the degree of aerated lung, not a single value from intubation to extubation. Verify that the chosen V T is achieving the desired physiologic effect and adjust it when necessary. Conditions wherelower Vt may be beneficial ARDS Lung Resection Single-lung Ventilation Chest Wall Deformaties ECMO Rationale Functional lung size is smaller Functional lung size is smaller Functional lung size is smaller Functional lung size is smaller Lung Rest 2016 Davies Respiratory Care 63 26
27 Conditions wherehigher Vt may be beneficial COPD and Asthma Metabolic Acidosis Neurological Injury Neuromuscular Patients Drug OD or Withdrawl Exercise(Rehabilitation) Rationale IncreasedVd, increased metabolic demands, increased WOB, acidosis, prolonged time constant Increased metabolic requirements, increased neural drive, increased WOB Increased neural drive unable to control with any mode Need to avoid atelectasis, preserve chest wall mobility, aid cough Increased neural drive, agitation, increased WOB, increased metabolic requirements Increased metabolic demand 2016 Davies Respiratory Care Davies Respiratory Care Two reasons to strongly consider the use of an initial Vt of 6 ml/kg PBW in all patients: Pulmonary damage can happen only a few hours after the initiation of mechanical ventilation with inappropriate settings. ARDS is frequently recognized after a delay in onset of the inflammatory process. Early use of 6 ml/kg PBW may be preventive as opposed to therapeutic. Especially protective in at-risk conditions, such as sepsis, trauma, transfusions, or high-risk surgeries
28 Low Vt s may cause ventilator/patient dys-synchrony and/or doubletriggering. Insufficient Inspiratory Time (Ti) Low Vt srequire shorter Ti s to be delivered Ventilator Ti may be shorter than the patients neural Ti Insufficient Inspiratory Flow (PIFR): Whether PIFR is set directly or as a function of Ti, it is integral to promoting synchrony. Low Vt srequire lower PIFR s to deliver set volume during Ti 2 large RCT s currently underway: PRe-VENT-NL (Netherlands) Critically ill patients without ARDS 4 6 ml/kg PBW vs 8 10 ml/kg PBW EPALI (Spain) Critically ill patients at risk of developing ARDS 6 ml/kg PBW vs 8 ml/kg PBW 68 28
29 2000 Rich J.Trauma, Injury, Infection and Crit Care PIFR = risk of VILI 2004 Maeda - Anesthesiology The PIFR in pressure-limited ventilation induced significantly more severe lung damage than the PIFR s in volume-control ventilation 2013 Gajic Respiratory Care Square wave flow profile of volume-control ventilation may be preferable than the more aggressive decelerating flow profile of pressure-control ventilation Square wave flow may be less well tolerated unless the patient is paralyzed 2012 Aboab J Critical Care Abrupt cessation of inspiratory flow enhances CO2 elimination. In ARDS patients an end-inspiratory pause: Reduces deadspace Reduces CO2 s No clinically significant increase in the intrinsic PEEP or negative hemodynamic effects 29
30 GOAL: RR = rate adequate to approximate the patients baseline spontaneous Ve(along with Vt) Adjust Vt and RR to achieve ph and plateau pressure goals Current consensus is that RR should not to exceed bpm Often needs to match the patients demand 2000 Blanch AJRCCM At the same pulmonary artery pressure, lower breathing frequencies lessened VILI 2012 Hartmann Critical Care For the same VT/strain, higher breathing frequencies intensify VILI Multiple strategies can be employed to improve patient/ventilator synchrony during lung-protective ventilation: Sedation, Analgesia, Paralysis Adjust RR Adjust Vt Adjust trigger sensitivity Minimize Auto-PEEP Adjust PIFR Adjust Ti Adjust inspiratory flow cycling Adjust rise time 30

31 2011 -de Graaff-Intensive Care Med Although most clinicians are aware of the adverse effects of hyperoxia, prevention of hypoxia often takes priority and liberal oxygenation targets tend to be preferred Gilbert-Kawai - Cochrane Database Systematic Review Goal of oxygen titration is to achieve: PaO mm Hg SpO2 approximately 90% Critically ill patients may tolerate lower PaO2 levels Permissive hypoxemia Don t automatically increase FiO2 in response to low PaO2 s Respiratory Rate Accurately measured Tidal Volume Accurately measured FiO2 Accurately measured PEEP Measured but not accurately Plateau Pressure Measured but not accurately 31

32 P PLAT Static pressure exerted by the volume of gas in the lungs at the end of an inhalation. Indicator of lung fullness 1993 Slutsky Chest - ACCP Consensus Conference Recommendation Maintain P PLAT <35cm H2O 2007 Jardin Intensive Care Medicine 352 ARDS patients P PLAT MORTALITY > 35 cmh2o 80% cmh2o 42% <27 cmh2o 30% 2003 Gattinoni Critical Care Medicine Avoidance of stretch by maintaining a low plateau pressureis one of the physiologic cornerstones of mechanical ventilation 2007 Malhotra NEJM The goal of low-vt ventilation is to maintain a P PLAT <30 cm H2O If P PLAT > 30 cmh2o then reduce Vt to 4cc/kg It is reasonable to allow P PLAT >30cmH2O in patients with stiff chest wall/increased abdominal pressures Pleural pressures are elevated but transpulmonary pressures are not 32
33 Check P PLAT (with a minimum 0.5 second inspiratorypause) at least q 4h andafter each change in PEEP or V T. If P PLAT >30 cmh2o: V T by 1ml/kg to minimum of 4 ml/kg. If P PLAT < 25 cmh2o andv T < 6 ml/kg: V T by 1 ml/kg until P PLAT > 25 cmh2o or V T = 6 ml/kg. If P PLAT < 30 but patient/ventilator dysynchronyis evident: V T by 1ml/kg to a V T of 7-8 ml/kg if P PLAT remains < 30 cm 2002 Eichacker AJRCCM Excessive reduction in plateau pressure might increase mortality in ARDS patients 2005 Hager AJRCCM Increased mortality in ARDS with day-1 P PLAT > cm H2O 2013 Terragni Anesthesiology A P PLAT <30 cmh2o does not identify all patients a risk of lung injury due to mechanical venton 78 33
34 PEEP -The pressure exerted by the volume of gas remaining in the lungs at end exhalation (FRC) necessary to prevent intra-tidal collapse Barach Annals of Internal Medicine First description of PEEP, used to treat pulmonary edema 1967 Ashbaugh Lancet Widespread use of PEEP in the treatment of ARDS begins Gattinoni NEJM PEEP reduces injurious alveolar shear stresses PEEP improves ventilation perfusion matching PEEP improves arterial oxygenation ARDSNet NEJM survival benefit with PEEP combined with Low Vt ventilation 2013 Ed-Khatib-CCMJournal Optimal PEEP is that which either results in: Best lung compliance Lowest intrapulmonary shunt Best conteract of compressive atelctasis Maximized alveolar recruitment 34
 Low PEEP Arm (475 pts) High PEEP arm (508 pts) Mean PEEP = 10.")
35 2001 Brower NEJM (the ALVEOLI Study) Low PEEP Arm (273 pts) High PEEP arm (276 pts) Mean PEEP = 8.9 cmh2o Mean PEEP = 14.7 cmh2o Mortality = 27.5% Mortality = 25% Mortality and VLOS not significantly different between both arms 2008 Meade JAMA (the LOVS Study) Low PEEP Arm (475 pts) High PEEP arm (508 pts) Mean PEEP = 10.1 cmh2o Mean PEEP = 15.6 cmh2o Mortality = 40% Mortality = 36% No significant difference in mortality or barotrauma with Open Lung protocol vs Low Vt protocol Open-Lung protocol did appear to improve hypoxemia 35
36 2008 Mercat JAMA (the EXPRESS Study) Low PEEP Arm (382 pts) High PEEP arm (385 pts) Mean PEEP = 7.1 cmh2o Mean PEEP = 14.6 cmh2o Mortality = 39% Mortality = 35% No significant difference in mortality. High PEEP arm: Improved lung function VLOS Duration of organ failure Briele JAMA Difference in hospital mortality between high and low PEEP arms was not statically significant (32.9% vs 35.2%) Statistically significant reduction of death in the ICU for patients in the High PEEP arm Clinicians needed to institute rescue therapies for profound hypoxemia less frequently in patients in the High PEEP group Rate of death following rescue therapy was also lower 36
37 2013 Santa Cruz Cochrane Databse of Systematic Reviews High levels of PEEP did not reduce hospital mortality compared to low levels of PEEP No significant difference in the risk of barotrauma with high levels of PEEP High levels of PEEP improved oxygenation to the first, third, and seventh days Chikhani British Journal of Anesthesia Not certain whether Low-PEEP vs High-PEEP strategies result in improvements in mortality and ventilator-free days. Select PEEP to improve Oxygenation 1975 Suter NEJM Select PEEP based upon best oxygenation and cardiac output Optimum PEEP is that which provides best respiratory compliance Select PEEP to Protect the Lung 1993 Bone JAMA Target of PEEP should not be oxygenation but prevention of intratidal collapse and decollapse. Open the lung and keep it open 37



38 Gas Exchange/ Oxygenation Maximal PEEP while avoiding overdistension Compliance Imaging ARDSNet PEEP Table Pressure/Volume Curve Stress Index Esophageal Pressures Lowest shunt (highest PaO2),lowest deadspace(lowest PaCO2), best oxygen delivery (CaO2 x C.O.) Use highest PEEP while maintaining Pplat < 30cmH20 Usethe highest PEEP that results in the highest respiratory-system compliance Computed tomography, electrical impedance tomography, ultrasound Table of FiO2and PEEP combinations to achieve PaO2 or SpO2 in target range Set PEEP slightly higher than the Lower Inflection Point Observe the pressure-timecurve during constant-flow inhalation for signs of tidal recruitment and overdistension Estimate the intra-pleuralpressure with an esophageal balloon measurement of esophageal pressure, then determine optimal PEEP 2004 ARDSNet NEJM ARDSNet suggested that the clinician consider the use of Incremental FiO2/PEEP tables to achieve goal of improved oxygenation. Low PEEP/High FiO2 Protocol FiO PEEP High PEEP/Low FiO2 Protocol FiO PEEP Couple of caveats: Assumes a Pleural Pressure of ZERO! Does not address PEEP Hunger Need for higher PEEP s with lower FiO2 s that some patients exhibit 38
39 The Pressure/Volume loop can be used for PEEP selection with the hypothesis that: A Lower Inflection Point (A) indicates the end of recruitment Set PEEP at the Lower Inflection Point pressure A Upper Inflection Point (B) indicates the beginning of hyperinflation 2001 Croti AJRCCM Collapsed units open-up at different pressures Recruitment is not limited to the LIP but occurs along the entire curve At pressures of 30 cmh2o up to 15-30% of the lung remains closed May require pressures up to 60 cmh2o to open 39



40 2004 Grasso Critical Care Medicine At a CONSTANT PIFR: Concave Paw waveform = Stress Index <1.0 = Inadequate PEEP Linear Paw waveform = Stress Index = 1.0 = Adequate PEEP Convex Paw waveform = Stress Index >1.0 = Excessive PEEP 2013 Terragni Anesthesiology Stress Index RS >1.05 may be indicative of developing VILI SI = 0.75 SI = 1.06 SI = Terragni AJRCCM 40
41 AIRWAYPRESSURE(PAW) Measured at the circuit wye or ventilator outlet Reflects both lung and pleural pressures Paw PLEURALPRESSURE(PPL) Pressure imposed upon the lungs by the Chest Wall and Abdomen Can be approximated by measuring pressures within the esophagus Pes Ptp TRANSPULMONARY PRESSURE(PTP) The true pressure within the lung PTP= PAW PES Ppl Airway pressures do not reflect pressures within the lung but pressures of the entire Respiratory System To know true Lung Pressure (Transpulmonary Pressure) you must account for the pressures outside of the lung (Pleural Pressures) Numerous studies have demonstrated reasonable correlation between Esophageal Pressures and Pleural Pressures Pleural pressures adjacent to the esophagus transmitted to esophagus. GOAL: Avoid alveolar collapse after recruitment by providing a PEEP that is greater than the compressive forces operating on the lung 41
42 2008 Talmor NEJM Could PEEP be managed better with P TP PEEP rather than the ARDSNet PEEP Tables? P TP PEEP Arm: P/F ra o respiratory-system compliance mortality 2010 Talmor Respiratory Care Estimate pleural pressures from PES Set PEEP to achieve a target P TP May allow higher PEEP in many patients without overdistending lung regions that are already recruited. P TP PEEP RESEARCH 2013 Yang Chinese Medical Journal In patients with ARDS and IAH PEEP titrated by transpulmonary pressure was higher than PEEP titrated by ARDSnetprotocol Oxygenation improved 2016 Kassis Intensive Care Medicine Compared to conventional PEEP titration using Pes for PEEP titration: Improved elastance Decreased driving pressures 42
43 2006 Borges AJRCCM Best recruitabilitywith stepwise PEEP increases PEEPs up to 45 cmh2o Driving Pressure fixed at 15 cmh2o DP = P PLAT -PEEP 2011 Silva Critical Care Medicine Compared to sustained inflation, stepwise increase in pressures: hemodynamic compromise microscopic and biochemical signs of lung injury 2010 Briele JAMA PEEP is beneficial in ARDS lungs with a high potential for recruitment PEEP can result in over-distension in ARDS lungs with a low potential for recruitment Malhotra NEJM Potential for lung recruitment can be inferred at the bedside: Recruitable Lung: If PEEP is and P PLAT then s in a lesser increment as the change in PEEP Non-Recruitable Lung: If PEEP is and P PLAT then sin an equal or greater increment as the change in PEEP 43


44 2015 Gattinoni Critical Care The best PEEP does not exist. To pretend and claim that we may find a PEEP level that avoids intratidalrecruitment-derecruitment, providing in the meantime the best compliance, best oxygenation and lowest deadspace, without causing hyperinflation and affecting hemodynamics, reflects a wishful dream that has nothing to do with the reality A reasonable approach may simply be tailoring PEEP according to the Berlin ARDS severity scale: Mild ARDS 5-10 cmh2o Moderate ARDS cmh2o Severe ARDS cmh2o 44
45 2012 Gattinoni Current Opinion in Anesthesiology Stress distribution of distending forces per unit area In the lung this distending force = transpulmonary pressure Strain deformation of the area in response to the stress 2016 Protti Critical Care Medicine Lung Strain Ratio between Vt and FRC Lung Strain Rate Ratio between Lung Strain and Ti Low Strain Rate I:E of 1:2 1:3 High Strain Rate I:E of 1: Amato NEJM Driving Pressure of the Respiratory System (DP RS ) may be a superior marker of VILI DP RS = P PLAT -PEEP DP RS correlated with mortality even in patients receiving lowvolume lung-protective ventilation However, did not account for effect of chest-wall 2016 Kassis IntCare Med Chest wall pressures may account for up to 33% of DP RS 45
46 2015 Loring NEJM Driving Pressure of the Lung (DP L ) takes into consideration the effect of the Pleural Pressure impinging upon the Lung by using transpulmonary pressures in the equation: DP L = P TP PLAT -P TP PEEP DP L, instead of DP RS, may be the more appropriate measure of lung injury due to the varying chest wall compliance and pleural pressures between patients Cressoni J.AmSociety of Anesth Vt and P PLAT represent static work of a single breath. Does the dynamicwork applied to the lung also contribute to VILI? Mechanical Power considers both static and dynamic energy applied over the lung over time. Mechanical Power (W) = P TP x Vt Lethally ventilated piglets (Vt=38cc/kg, P TP PLAT =27cmH2O) with varying RR s While RR only varied 5 fold (3-15bpm), powerincreased 11 fold as PIFR is augmented at higher RR. Determined that a power of 12 Joules/minute was threshold for VILI Does PIP still play a role in VILI? 46
47 47
48 1987 Downs Critical Care First description of Airway Pressure Release Ventilation 2001 Frawley AACN Clinical Issues Relatively high CPAP with regular, brief, intermittent releases in airway pressure Unlike CPAP, APRV facilitates both oxygenation and CO2 clearance Release phase permits alveolar ventilation & removal of CO2 Time-triggered, pressure-limited, time-cycled mode of mechanical ventilation Allows unrestricted spontaneous breathing 2011 MODRYKAMIEN Cleveland Clinic Journal of Medicine 48
 - Fixed APRV (F-APRV): Relatively short Thigh (<90% total cycle time) Fixed Tlow")

49 2016 Jain Intensive Care Medicine Experimental Care must be exercised when reviewing APRV research as there are two eras in the application of APRV: Early Methodology (Downs/Stock) - Fixed APRV (F-APRV): Relatively short Thigh (<90% total cycle time) Fixed Tlow not adjusted based on changing lung mechanics Recent Methodology (Habashi) Personalized (P-APRV) Phighset at previous P PLAT Thigh > 90% of total cycle time Tlow adjusted based on changes in lung mechanics Analysis of expiratory flow curve Plow set at 0 cmh2o Fixed Personalized 49
 Minimizes airway pressure (animal studies) Seems to decrease or prevent lung injury Allows unrestricted spontaneous")

50 2011 Mondrykamien Cleveland Clinic Journal of Medicine Mireles-Cabodevila & Kacmarek Respiratory Care PRO Mireles-Cabodevila Serves the goals of safety and comfort. Promotes alveolar stability and recruitment (animal studies) Minimizes airway pressure (animal studies) Seems to decrease or prevent lung injury Allows unrestricted spontaneous breathing CON Kacmarek No humanstudies have demonstrated a reduction in WOB No human studies have demonstrated a reductionin the need for sedation and narcotics No human studies have demonstrated a minimized likelihood of VILI No human studies have demonstrated a reduction in VLOS or ICU stay No human studies have demonstrated a effect on mortality. 50

51 Mireles-Cabodevila Spontaneous breathing seemslike a positive but research on spontaneous breathing during APRV is scant. Modes of ventilation are just like medications; you need the correct one, at the correct dose, and for the right time for a given condition. APRV, like many other modes, is still looking for definition of the dose, the timing, and optimization of its delivery. Kacmarek: APRV has a greater potential for adversely affecting patient outcome than improving it Unless definitive data are forthcoming demonstrating outcome benefits from the use of APRV in ARDS or any other patient group, there is no reason to consider this approach to ventilatory support. 51
52 High Frequency ventilators are described by their delivery method and classified by their exhalation mechanism (active or passive). High-Frequency Oscillatory Ventilation (HFOV) Active Exhalation High-Frequency Percussive Ventilation (HFPV) Passive Exhalation 2011 Ali Crit Care Clin Constant mean airway pressure Pressure waves in the ventilatory circuit (generated by a diaphragm) at frequencies between 3 and 15 Hz ( bpm) Active exhalation as diaphragm creates both inspiratory and expiratory pressure waves May be beneficial in preventing hyperinflation and controlling CO2 elimination 1972 Lunkenheimer Br J Anaesth First published findings of adequate CO2 clearance with HFOV Numerous RCT s of HFOV in neonatal respiratory distress have been conducted but there is a smaller body of work in adult HFOV
53 2000 FDA approval of Adult HFOV Initially a rescue therapy for patients failing conventional ventilation Expanding into treatment of patients with severe ARDS 2002 Derdak AJRCCM (MOAT Trial) First RCP comparing HFOV with conventional ventilation HFOV group: Significant in P/F ra o Did not persist past 24 hrs No significant difference in hemodynamic variables Trend towards mortality Derdak-AJRCCM Early but non-sustained in the P/F ra o Similar complication rates Non-significant trend towards reduced 30-day mortality 2003 Sedeek Anesthesiology histological damage & lung inflamma on with HFOV vs CMV 2013 Mashael SeminRespirCrit Care Med Mean airway pressures during HFOV often exceed the cm H2O lung-protective threshold employed during CMV. Could tolerance of higher mean s during HFOV be 2 to better maintained alveolar structure with a slowlyapplied constant pressure as opposed to cyclical brief tidal pressures? 53
54 2010 Sud BMJ 8 RCT s with a total of 419 patients were included Almost all patients had ARDS HFOV may mortality in ARDS pa ents HFOV P/F ra o No significant difference in VLOS Ventilator-free days No significant differences in the risk of: Barotrauma Hypotension Endotracheal tube obstruction 2013 Ferguson NEJM (The OSCILLATE Study) mortality with HFOV compared to CMV with high PEEP s need for pressor medications High mean-airway pressures led to hemodynamic compromise 2013 Young NEJM (The OSCAR Study) No major difference in outcome between HFOV and CMV 2013 Malhotra NEJM (Editorial Response) OSCILLATE & OSCAR underscore the notion that HFOV should be: Reserved for patients failing conventional lung protective strategies Provided by clinicians with expertise in the technology. 54

55 2010 Allan J Burn Care Res Small high-frequency pulses of gas Pulses accumulate/stack to form a low -frequency Vt Emulates a typical pressurelimited, time-cycled waveform Salim Critical Care Medicine HFPV provides favorable gas exchange in several well-defined patient populations oxygena on and PIP s vs conven onal ven la on 2006 Eastman American Journal of Surgery HFPV may oxygenation in patients with ARDS without a concomitant increase in mpaw 2010 Allan J Burn Care Res Lack of literature regarding the practical application of HFPV theory toward improving gas exchange. No discussion has been held regarding the possible risk of HFPVassociated VILI

56 1957 Saxon J ApplPhysiol First published report of closed-loop ventilation Described a servo mechanism to automatically adjust the negative pressure of an iron lung ventilator in response to EtCO Wysocki Critical Care Clinics Early closed-loop systems designed to maintain ABG s at normal levels Current closed-loop systems designed to: Improve lung-protection Disease is a dynamic process so closed-loop system may be able to automatically adjust in response Reduce clinician errors Cover resource limitations 56
 to maintain the pre-set PSV pressure (input).")
57 2002 Branson Respiratory Care Simple -control of oneoutputbased on the measurement of one input. The constant modification of inspiratory flow (output) to maintain the pre-set PSV pressure (input). Complex -measurement of multiple inputs (eg, compliance, oxygen saturation, respiratory rate) to control multiple outputs (eg, ventilator frequency, airway pressure, tidal volume). 57
58 1977 Hewlett Anesthesia First description of Mandatory Minute Ventilation (MMV) ASV is based upon MMV with adaptive pressure control 1994 Laubscher -IEEE Trans Biomed Eng First description of clinical application of ASV Measured respiratory mechanics applied to algorithms of pressure control to maintain a target Ve 2007 ASV commercially available in the US 2014 Chopra Journal of Association of Chest Physicians Assist-control, pressure-targeted, time-cycled mode RR/Vt pattern automatically set according to minimize ventilator work. Selects the appropriate RR and Vt for mandatory breaths Selects the appropriate Vt or spontaneous breaths This minimal ventilator work maytranslate into minimal stretching forces on the lungs
59 2008 Chen -J lnternmed Taiwan Small studies have demonstrated that ASV can be used as a safe weaning mode for specific postoperative and chronically ventilated patient groups May save manpower and management, May reduce VILI There is concern regarding patient/ventilator asynchrony if there is no awareness of the underlying mechanism for respiratory distress in the patients Could worsen the patient's condition or prolong weaning process 2015 Kirakli Chest RCT comparing ASV vs pressure A/C in Medical ICU patients Previous RCT s focused on post-op cardiac patients ASV arm outcomes: VLOS number of manual ventilator setting changes pa ents extubated successfully on the first a empt Weaning success and mortality at day 28 were comparable between the two arms 59

60 2016 Greico Chest Aspects of the Kirakli RCT require further discussion Reasons of weaning failure were not presented. PSV was contemplatedin the PC-CMV arm only afterfailure of the third SBT Delay in applying PSV hampers the understanding of to what extent the benefit described in patients receiving ASV No mention of sedation in either arms Patients in the PC-CMV arm may have required more sedation to achieve adequate patient/ventilator interaction. No data on fluid balance and cardiac function even though cardiac decompensation and fluid overload are recognized as the most common causes of SBT failure 60
61 1992 Younes ARRD First description of Proportional Assist Ventilation (PAV_ 2007 Wysocki Critical Care Clinics Pressure-regulated mode of ventilation Inspiratory airway pressure is titrated within each breath in proportion to the patients inspiratory airflow Surrogate of the patient s respiratory muscle effort The proportionality between flow and airway pressure is determined by the clinician determining the proportions of the total WOB to be performed by both ventilator and patient. PAV+measures resistance (R rs ) and compliance (C rs ) of the respiratory system and the percentage of assistance adjusted accordingly Chopra Journal of Association of Chest Physicians All PAV breaths are spontaneous. Patient controls the timing and size of the breath. No present pressures, flow, or volume goals Safety limits on the volume and pressure delivered can be set. Patient effort is boosted according to a pre-set proportion of the measured WOB. pa ent effort = delivered flow PAV is contraindicated in: Respiratory depression (bradypnea) Large air leaks (e.g. bronchopleural fistulas) 61
62 2008 Gruber Anesthesiology WOB vs PSV 2006 Kondili Anesthesiology Hemodynamic profile similar to that of PSV Vt sare variable but are usually within the lung-protective range 2008 Xirouchaki Intensive Care Medicine patient/ventilator dys-synchrony vs PSV probability of spontaneous breathing without assistance vs PSV No trial has reported effect of PAV on mortality 2015 Teixiera Respiratory Care RCT compared weaning with PAV+, PSV, or T-tube When subjects were ready to perform the SBT: PAV+ group -ventilated in PAV mode up to 40% support PSV group -ventilated with 7 cmh2o T-tube group - connected to T-piece with supplemental oxygen. No significant differences in the groups was observed regarding: Rate of extubation failure VLOS Duration of ICU and hospital stay 62

63 2016 Gautam IJRCCM Crossover study comparing PAV+ to PSV Ventilator Ti was significantly longer than patient Ti in PSV vs PAV+ pa ent/ven lator dys-synchronies were in PAV+ vs PSV while patients were awake Variable end inspiratory hold observed in PAV+. Non-significant in compliance and P/F ratio in PAV+ PSV and PAV+ modes perform similarly for patient-ventilator interactions in awake and sedated states. Changeover between modes resulted in swings in hemodynamics and respiratory mechanics Patient tunes to ventilator deliveries over time. 63
64 1999 Sinderby Nature Medicine First published report of NAVA technology 2014 Chopra Journal of Association of Chest Physicians Diaphragmatic EMG signal (EAdi) triggers and cycles ventilator breath. EMG sensor positioned in esophagus at crurallevel of the diaphragm. Triggering -virtually simultaneous with phrenic nerve excitation of inspiratory muscles. Termination -linked to the cessation of inspiratory muscle contraction Patthum- JBI Database of Systematic Rev & ImplemenReports Ventilatory assist proportional to EAdi Chopra Journal of Association of Chest Physicians Small clinical studies have demonstrated improved trigger and cycle synchrony with NAVA Data lacking showing improved outcomes (e.g. VLOS, sedation needs). Concern with NAVA is the expense associated with the EMG sensor Diniz-Silva ATS 2016 variability of Vt and Paw with NAVA vs PSV 2016 Carteaux Critical Care Medicine Can be excessively sensitive to EAdi in terms of triggering 2016 Demoule Critical Care Medicine Associated with less frequent application of post-extubation noninvasive mechanical ventilation
 PaCO2 averaged 60 mmhg Effects of Respiratory Acidosis:")
65 Volutrauma & atelectrauma are more detrimental to patient outcomes than respiratory acidosis Hickling Intensive Care Medicine First description of Permissive Hypercapnia 50 ARDS patients with 16% mortality (predicted to be 40%) PaCO2 averaged 60 mmhg Effects of Respiratory Acidosis: Cellular: In the absence of hypoxemia, intracellular acidemia appears to be well tolerated. Cardiovascular: Increased HR, BP & stroke volume. CNS: Variable, some agitation may occur. 65
66 I:E of 1:1 or inverse (I>E) Possible alternative to PEEP Usually reserved for patients with plateau pressures >35 cm H20 Ti may improve shunt in severe ventilatory failure Understanding of ventilator graphics very important 1998 Tharrat Chest Inverse ratio ventilation improves arterial oxygenation mean alveolar pressure with PIP 2013 Lee Anesthesia I:E ratio of 1:1 vs I:E ratio of 1:2 in one-lung ventilation: Modest in oxygenation 66
67 2015 Naik Respiratory Care Biological systems are characterized by a continuously variable response to changing intrinsic or extrinsic input (noise) Bad Noise = irregular, random input Good Noise = frequency and amplitude of input controlled Signal outputcan be improved with good noise This paradoxical effect of noise is termed stochastic resonance Lefevre AJRCCM First description of Variable Ventilation Variable ventilation arm: RR range of breaths/min with over 360 RR changes Vt varied 75% -135% of mean Vt Variable ventilation arm: Significant in arterial oxygenation Significant respiratory compliance postmortem wet/dry lung weight 67
68 Currently no commercially available ventilators capable of performing variable ventilation Pelosi AJRCCM The application of intermittent sigh breaths offers the opportunity to introduce some limited variability Steimback Intensive Care Medicine Sigh breath frequency should be limited to 2 3 breaths/min Facilitates maximum recruitment without inducing volumerelated lung injury Terragni AJRCCM Low-Vt ventilation does not definitively protect the lung from overdistention during a tidal breath. End-inspiratory over-distention occurs in 30% of ARDS patients receiving lung-protective ventilation May be 2 extensive consolidated dorsal lung regions not recruited during the tidal breath. Maneuvers to recruit alveoli might counteract those adverse effects of low VT and improve oxygenation 68

69 2007 Kacmarek Respiratory Care Intentional, transient increase in transpulmonary pressure Reopen non-aerated/poorly aerated alveoli. Immediate expected benefits are improvements in oxygenation and respiratory system compliance 2015 Suzumura Intensive Care Medicine RMs have a clear role as rescue therapy for patients with severe hypoxemia, refractory to protective ventilation strategies and prone position. 69


70 2015 Suzumura Intensive Care Medicine 2008 Badet Respiratory Care Sighs superimposed on lung-protective ventilation significantly improve oxygenation and Cstat in patients with ALI/ARDS Sigh/decremental PEEP Procedure: 1. Sustained inflation of 40 cmh2o for 30 seconds 2. Adjust PEEP to 24 cmh2o for 10 minutes Adjusted Vt to maintain P PLAT < 32 cmh2o 3. Stepwise decrement of PEEP of 4 cmh2o every 10 min Measure ABG & C STAT after each decrement 4. Re-set PEEP to optimal PEEP The PEEP below which PaO2/FIO2 fell by at least 20%. 70


71 2015 Suzumura Intensive Care Medicine 2016 Pirrone- Critical Care Medicine Determining optimal PEEP in morbidly obese patients: Method #1 - Decremental PEEP Protocol 1. PEEP in a stepwise manner un l P TP PEEP = cmh2o 2. PEEP then set 4 cmh2o higher than the P TP PEEP PEEP level. 3. After 2 minutes P PLAT & PEEP were measured and Driving Pressure (Pplat PEEP) was calculated 4. PEEP by 2 cmh2o, step 3 repeated for at least 5 increments 5. Best decremental PEEP = PEEP with lowest Driving Pressure 6. PEEP set at best decremental PEEP plus 2 cmh2o Method #2 -Stepwise Recruitment Maneuver 1. Initial PEEP = 15 cmh2o 2. PEEP by 5 cmh2o every 30 seconds 3. Total duration of the RM was 2 minutes 71
72 PEEP selected by the ICU team prior to the trial averaged 9 cmh2o lower than PEEP determined by titration methods RM followed by PEEP titration significantly improves EELV RM performed with lowest PEEP with a positive P TP PEEP : EELV by 3 ml/kg P TP INSP by 1.5 cm H2O Suggests a more favorable distribution of volume among alveolar units. RM followed by PEEP titration significantly improves lung elastance and oxygenation PEEP without a RM did not significantly improve lung elastance 2004 Chu Critical Care Medicine Atelectatic lung is relatively inert with scant cytokine production Cytokine production may be markedly increased by inadequate recruitment or repeated derecruitment Rzezinski Respir Physiol Neurobiol Progressive RM significantly reduced lung inflammation, alveolar epithelial cell apoptosis, and alveolar-capillary membrane injury Epithelial damage more pronounced if high distending pressures are applied abruptly as compared to progressive approaches 72
73 Koutsoukou Health Science Journal High distending pressure may impair hemodynamics Correcting patients volume status prior to RM may attenuate potent circulatory depression 2010 Silva Critical Care Fluid management, used to minimize hemodynamic instability associated with RM s, may have an impact on lung and distal organ injury In hypervolemic animals RM s: Improved oxygenation Increased lung injury Increased inflammatory and fibrogenic responses. 73
74 May promote recruitment of dependent, atelectatic lung regions by relieving external compressive forces Abdominal contents push upward on the diaphragm and collapse lower lobes of the lung. Over 40% of left lung and 15% of right lung are located underthe heart and may be compressed 2006 Mancebo AJRCCM Trend towards survival when prone positioning: Administered early For a much as 20h /day 2009 Taccone JAMA No significant survival benefit in ARDS patients or in patients with moderate and severe hypoxemia Sud BMJ (meta-analysis) mortality (by about 10%) in the most hypoxic patients (P/F < 100) 2013 Guerin NEJM The PROSEVA Trial RCT involving 566 patients Test arm patients were pronedat least 16 h/day Early application of prolonged prone-positioning sessions significantly 28-& 90-day mortality. 74

75 2009 Taccone JAMA need for increased seda on/muscle relaxants Airway obstruction Transient desaturation Vomiting Hypotension, arrhythmias, increased vasopressors Loss of venous access Displacement of endotracheal tube Displacement of thoracotomy tube 75
76 2014 Chopra Journal of Association of Chest Physicians Endotracheal tubes provide a significant resistance to flow during both inspiration and expiration. May result in significant initial flow dys-synchrony in patients with vigorous inspiratory efforts Frutos-Vivar Intensive Care Medicine Designed to overcome the imposed WOB due to artificial airways by providing dynamic ventilatory support of each spontaneous breath Delivers the exact amount of pressure necessary to overcome the resistive load of the endotracheal tube for the flow measured at that time Frutos-Vivar Intensive Care Medicine Mode evaluated as a method for the first trial of withdrawal from mechanical ventilation in a few studies Favorable results in the rate of successful first weanings Rate of extubation failure was similar to that reported using other weaning modes 1998 Strauss AJRCCM A 2-hour trial of spontaneous breathing through an ETT mimicked the WOB performed after extubation. The WOB dissipated against the ETT represented around 10% of the overall work performed by the patient. This increased work load was not different from what was related to upper airways obstruction immediately following extubation The use of such a compensatory mode may falsify spontaneous 170 breathing trial relevance. 76
77 2009 Aggarwal Respiratory Care 41 patients requiring mechanical ventilation due to acute respiratory failure secondary to poisoning from snakebites. Compared weaning time of PS with ETRC vs PSV alone PSV with ETRC median weaning time was 8h PSV alone median weaning time was 12h 2012 Oto Respiratory Care ETRC does not necessarily compensate for an ETT-imposed respiratory work load. ETT configuration changes and tracheal secretions can increase ETT resistance and decrease the ability of ETRC to compensate for the increased respiratory work load Frutos-Vivar Intensive Care Medicine Designed to overcome the imposed work of breathing due to artificial airways. Provides dynamic ventilatory support of each spontaneous breath Delivers the exact amount of pressure necessary to overcome the resistive load of the endotracheal tube for the flow measured at that time This mode has been evaluated as a method for the first trial of withdrawal from mechanical ventilation in a few studies Favorable results in the rate of successful first weanings Rate of extubation failure was similar to that reported using other weaning modes
78 2013 El-Gendy TherDeliv Almost all of the currently used exogenous surfactants have a high efficacy in treating neonatal respiratory distress syndrome, yet almost none of them are as successful in treating surfactant dysfunction in adults Willson Chest Administration of calfactant was not associated with improved oxygenation or longer-term benefits relative to placebo in this randomized, controlled, and masked trial. At present, exogenous surfactant cannot be recommended for routine clinical use in ARDS. 78

79 2012 Meng J Cardiothoracic and Vasc Anesthesia (Meta-Analysis) Nine trials involving 2,575 patients Surfactant replacement therapy: Does not significantly decrease mortality. Increases P/F ratio in the first 24 hours Lost by 120 hours. Causes a non-significant trend towards lower VLOS Slightly higher risk of adverse effects. 79
80 2005 Griffiths JAMA ino induces vasodilatation in ventilated lung areas 2015 Bhatraju Nitric Oxide ino diffuses across the alveolar membrane and binds with Hb Allows for ino to positively modulate the pulmonary circulation. ino selectively works on area of lung that maintains ventilation Lung units that maintain ventilation Vasculature will dilate and preferentially receive more of the systemic blood flow. Improves V/Q Lung units with impaired ventilation Lower ratio of perfusion Provide a lower amount of the body's total arterial oxygenation 2000 Payen Clin ChesMed When dissolved in alveolar fluid ino may react with Reactive Oxygen Species to form reactive Nitrogen species which may be cytotoxic to epithelial calls Adhikari-BMJ Trend towards increased mortality rates in groups using ino Significantly increased risk for renal dysfunction 2014 Adhikari Critical Care Medicine Nitric oxide does not reduce mortality in adults or children with ARDS, regardless of the degree of hypoxemia. 80

81 2016 Gebistorf Cochrane Reviews Evidence is insufficient to support INO in any category of critically ill patients with acute hypoxemic respiratory failure Inhaled NO results in a transient improvement in oxygenation Inhaled NO does not reduce mortality Inhaled NO seems to increase renal impairment. 81


82 It is remarkable how little The most is known meaningful about cost reduction alveolar deformation during breathing. of clinical care and elimination of strategies will involve standardization variation in patient procedures. Rolf Hubmayr Am J RespirCrit Care Med, 2002 May 9,

83 Positive-pressure ventilation is a proven, effective modality but is the cause of immense physiological derangements: Redistribution of alveolar ventilation Altered capillary perfusion Functional changes in surfactant Transcapillary fluid shifts Impaired lymphatic drainage Impeded venous return These derangements all contribute to wet, harder-to-ventilate lungs which necessitate even more aggressive positive-pressure ventilation. To minimize these derangements clinical evidence supports: Small Vt(4-6 ml/kg IBW) Optimal PEEP therapy Plateau Pressure maintained below 30cmH2O 83

84 Acute Lung Injury: Prevention May Be the Best Medicine, LitellJ, Resp Care 2011 Dynamic Alveolar Mechanics and Ventilator-Induced Lung Injury, Carney, Crit Care Med 2005 Acute Respiratory Distress Syndrome and Acute Lung Injury, Dushianthan, Postgrad Med Journal, 2011 Ventilator-Induced Lung Injury in Healthy and Diseased Lungs, Pelosi, Anesthesiology 2011 Acute Lung Injury and Acute Respiratory Distress Syndrome, Mackay, Cont Ed in Anaesthesia, Crit Care and Pain, 2009 New Insights Into the Pathogenesis of the Acute Respiratory Distress Syndrome, Slutsky, Medscape Crit Care
4/1/2017 Inhalation NEGATIVE Exhalation:
 1 2 3 Inhalation Active process Diaphragm and intercostal muscles contract to increase thoracic volume vertically creating a NEGATIVE change in thoracic pressure. At end inhalation alveolar pressure equalizes
1 2 3 Inhalation Active process Diaphragm and intercostal muscles contract to increase thoracic volume vertically creating a NEGATIVE change in thoracic pressure. At end inhalation alveolar pressure equalizes
4/1/2017. Volume. Flow. Pressure
 1 Inhalation Active process Diaphragm and intercostal muscles contract to increase thoracic volume vertically creating a NEGATIVE change in thoracic pressure. At end inhalation alveolar pressure equalizes
1 Inhalation Active process Diaphragm and intercostal muscles contract to increase thoracic volume vertically creating a NEGATIVE change in thoracic pressure. At end inhalation alveolar pressure equalizes
Mechanical Ventilation. Mechanical Ventilation is a Drug!!! is a drug. MV: Indications for use. MV as a Drug: Outline. MV: Indications for use
 Mechanical Ventilation is a Drug!!! Mechanical Ventilation is a drug I am an employee of Philips Healthcare Hospital Respiratory Care Group and they help me pay for my kids education Jim Laging, RRT, RCP
Mechanical Ventilation is a Drug!!! Mechanical Ventilation is a drug I am an employee of Philips Healthcare Hospital Respiratory Care Group and they help me pay for my kids education Jim Laging, RRT, RCP
Mechanical Ventilation of the Patient with ARDS
 1 Mechanical Ventilation of the Patient with ARDS Dean Hess, PhD, RRT, FAARC Assistant Professor of Anesthesia Harvard Medical School Assistant Director of Respiratory Care Massachusetts General Hospital
1 Mechanical Ventilation of the Patient with ARDS Dean Hess, PhD, RRT, FAARC Assistant Professor of Anesthesia Harvard Medical School Assistant Director of Respiratory Care Massachusetts General Hospital
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES
 INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES") INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
Basics of Mechanical Ventilation. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of Mechanical Ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Overview of topics 1. Goals 2. Settings 3. Modes 4. Advantages and disadvantages
Basics of Mechanical Ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Overview of topics 1. Goals 2. Settings 3. Modes 4. Advantages and disadvantages
Selecting the Ventilator and the Mode. Chapter 6
 Selecting the Ventilator and the Mode Chapter 6 Criteria for Ventilator Selection Why does the patient need ventilatory support? Does the ventilation problem require a special mode? What therapeutic goals
Selecting the Ventilator and the Mode Chapter 6 Criteria for Ventilator Selection Why does the patient need ventilatory support? Does the ventilation problem require a special mode? What therapeutic goals
OPEN LUNG APPROACH CONCEPT OF MECHANICAL VENTILATION
 OPEN LUNG APPROACH CONCEPT OF MECHANICAL VENTILATION L. Rudo Mathivha Intensive Care Unit Chris Hani Baragwanath Aacademic Hospital & the University of the Witwatersrand OUTLINE Introduction Goals & Indications
OPEN LUNG APPROACH CONCEPT OF MECHANICAL VENTILATION L. Rudo Mathivha Intensive Care Unit Chris Hani Baragwanath Aacademic Hospital & the University of the Witwatersrand OUTLINE Introduction Goals & Indications
Initiation and Management of Airway Pressure Release Ventilation (APRV)
") Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Indications for Mechanical Ventilation. Mechanical Ventilation. Indications for Mechanical Ventilation. Modes. Modes: Volume cycled
 Mechanical Ventilation Eric A. Libré, MD VCU School of Medicine Inova Fairfax Hospital and VHC Indications for Mechanical Ventilation Inadequate ventilatory effort Rising pco2 with resp acidosis (7.25)
Mechanical Ventilation Eric A. Libré, MD VCU School of Medicine Inova Fairfax Hospital and VHC Indications for Mechanical Ventilation Inadequate ventilatory effort Rising pco2 with resp acidosis (7.25)
High Frequency Ventilation. Neil MacIntyre MD Duke University Medical Center Durham NC USA
 High Frequency Ventilation Neil MacIntyre MD Duke University Medical Center Durham NC USA High frequency ventilation Concept of ventilator induced lung injury and lung protective ventilatory strategies
High Frequency Ventilation Neil MacIntyre MD Duke University Medical Center Durham NC USA High frequency ventilation Concept of ventilator induced lung injury and lung protective ventilatory strategies
Why we should care (I)
") What the $*!# is Lung Protective Ventilation and Why Should I be Using it in the OR? Disclosures KATHERINE PALMIERI, MD, MBA 64 TH ANNUAL POSTGRADUATE SYMPOSIUM UNIVERSITY OF KANSAS MEDICAL CENTER DEPARTMENT
What the $*!# is Lung Protective Ventilation and Why Should I be Using it in the OR? Disclosures KATHERINE PALMIERI, MD, MBA 64 TH ANNUAL POSTGRADUATE SYMPOSIUM UNIVERSITY OF KANSAS MEDICAL CENTER DEPARTMENT
Lung recruitment maneuvers
 White Paper Lung recruitment maneuvers Assessment of lung recruitability and performance of recruitment maneuvers using the P/V Tool Pro Munir A Karjaghli RRT, Clinical Application Specialist, Hamilton
White Paper Lung recruitment maneuvers Assessment of lung recruitability and performance of recruitment maneuvers using the P/V Tool Pro Munir A Karjaghli RRT, Clinical Application Specialist, Hamilton
What is Lung Protective Ventilation? NBART 2016
 What is Lung Protective Ventilation? NBART 2016 Disclosure Full time employee of Draeger Outline 1. Why talk about Lung Protective Ventilation? 2. What is Lung Protective Ventilation? 3. How to apply Lung
What is Lung Protective Ventilation? NBART 2016 Disclosure Full time employee of Draeger Outline 1. Why talk about Lung Protective Ventilation? 2. What is Lung Protective Ventilation? 3. How to apply Lung
The ARDSnet and Lung Protective Ventilation: Where Are We Today
 The ARDSnet and Lung Protective Ventilation: Where Are We Today 4-16-12 RCSW Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Disclosure
The ARDSnet and Lung Protective Ventilation: Where Are We Today 4-16-12 RCSW Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Disclosure
APRV: Moving beyond ARDSnet
 APRV: Moving beyond ARDSnet Matthew Lissauer, MD Associate Professor of Surgery Medical Director, Surgical Critical Care Rutgers, The State University of New Jersey What is APRV? APRV is different from
APRV: Moving beyond ARDSnet Matthew Lissauer, MD Associate Professor of Surgery Medical Director, Surgical Critical Care Rutgers, The State University of New Jersey What is APRV? APRV is different from
Mechanical Ventilation
 Mechanical Ventilation Chapter 4 Mechanical Ventilation Equipment When providing mechanical ventilation for pediatric casualties, it is important to select the appropriately sized bag-valve mask or endotracheal
Mechanical Ventilation Chapter 4 Mechanical Ventilation Equipment When providing mechanical ventilation for pediatric casualties, it is important to select the appropriately sized bag-valve mask or endotracheal
Mechanical Ventilation Guided by Esophageal Pressure in Acute Lung Injury *
 A teaching hospital of Harvard Medical School Mechanical Ventilation Guided by Esophageal Pressure in Acute Lung Injury * Ray Ritz BA RRT FAARC Beth Israel Deaconess Medical Center Boston MA * n engl j
A teaching hospital of Harvard Medical School Mechanical Ventilation Guided by Esophageal Pressure in Acute Lung Injury * Ray Ritz BA RRT FAARC Beth Israel Deaconess Medical Center Boston MA * n engl j
Mechanical Ventilation. Which of the following is true regarding ventilation? Basics of Ventilation
 Mechanical Ventilation Jeffrey L. Wilt, MD, FACP, FCCP Associate Professor of Medicine Michigan State University Associate Program Director MSU-Grand Rapids Internal Medicine Residency Which of the following
Mechanical Ventilation Jeffrey L. Wilt, MD, FACP, FCCP Associate Professor of Medicine Michigan State University Associate Program Director MSU-Grand Rapids Internal Medicine Residency Which of the following
VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL
 VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National
VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National
ONLINE DATA SUPPLEMENT. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg
 APPENDIX 1 Appendix 1. Complete respiratory protocol. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg predicted body weight (PBW)) (NEJM 2000; 342
APPENDIX 1 Appendix 1. Complete respiratory protocol. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg predicted body weight (PBW)) (NEJM 2000; 342
Neonatal tidal volume targeted ventilation
 Neonatal tidal volume targeted ventilation Colin Morley Retired Professor of Neonatal Medicine, Royal Women s Hospital, Melbourne, Australia. Honorary Visiting Fellow, Dept Obstetrics and Gynaecology,
Neonatal tidal volume targeted ventilation Colin Morley Retired Professor of Neonatal Medicine, Royal Women s Hospital, Melbourne, Australia. Honorary Visiting Fellow, Dept Obstetrics and Gynaecology,
Mechanical Ventilation
 Mechanical Ventilation Understanding Modes Rob Chatburn, RRT-NPS, FAARC Research Manager Respiratory Therapy Cleveland Clinic Associate Professor Case Western Reserve University 1 Overview Characteristics
Mechanical Ventilation Understanding Modes Rob Chatburn, RRT-NPS, FAARC Research Manager Respiratory Therapy Cleveland Clinic Associate Professor Case Western Reserve University 1 Overview Characteristics
The Basics of Ventilator Management. Overview. How we breath 3/23/2019
 The Basics of Ventilator Management What are we really trying to do here Peter Lutz, MD Pulmonary and Critical Care Medicine Pulmonary Associates, Mobile, Al Overview Approach to the physiology of the
The Basics of Ventilator Management What are we really trying to do here Peter Lutz, MD Pulmonary and Critical Care Medicine Pulmonary Associates, Mobile, Al Overview Approach to the physiology of the
Sumit Ray Senior Consultant & Vice-Chair Critical Care & Emergency Medicine Sir Ganga Ram Hospital
 Sumit Ray Senior Consultant & Vice-Chair Critical Care & Emergency Medicine Sir Ganga Ram Hospital ARDS pathophysiology B Taylor Thompson et al. NEJM 2017;377:562-72. Outcome Australian Epidemiologic
Sumit Ray Senior Consultant & Vice-Chair Critical Care & Emergency Medicine Sir Ganga Ram Hospital ARDS pathophysiology B Taylor Thompson et al. NEJM 2017;377:562-72. Outcome Australian Epidemiologic
Invasive Ventilation: State of the Art
 ARDSnet NEJM 2000;342:1301 9-30-17 Cox Invasive Ventilation: State of the Art Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts A V T of 6 ml/kg PBW results
ARDSnet NEJM 2000;342:1301 9-30-17 Cox Invasive Ventilation: State of the Art Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts A V T of 6 ml/kg PBW results
Presentation Overview. Monitoring Strategies for the Mechanically Ventilated Patient. Early Monitoring Strategies. Early Attempts To Monitor WOB
 Monitoring Strategies for the Mechanically entilated Patient Presentation Overview A look back into the future What works and what may work What s all the hype about the WOB? Are ventilator graphics really
Monitoring Strategies for the Mechanically entilated Patient Presentation Overview A look back into the future What works and what may work What s all the hype about the WOB? Are ventilator graphics really
excellence in care Procedure Management of patients with difficult oxygenation. For Review Aug 2015
 Difficult Oxygenation HELI.CLI.12 Purpose This procedure describes the processes and procedures for a lung protective strategy in the mechanical ventilation of patients that are difficult to oxygenate
Difficult Oxygenation HELI.CLI.12 Purpose This procedure describes the processes and procedures for a lung protective strategy in the mechanical ventilation of patients that are difficult to oxygenate
Objectives. Respiratory Failure : Challenging Cases in Mechanical Ventilation. EM Knows Respiratory Failure!
 Respiratory Failure : Challenging Cases in Mechanical Ventilation Peter DeBlieux, MD, FAAEM, FACEP LSUHSC University Hospital Pulmonary and Critical Care Medicine Emergency Medicine pdebli@lsuhsc.edu Objectives
Respiratory Failure : Challenging Cases in Mechanical Ventilation Peter DeBlieux, MD, FAAEM, FACEP LSUHSC University Hospital Pulmonary and Critical Care Medicine Emergency Medicine pdebli@lsuhsc.edu Objectives
Guide to Understand Mechanical Ventilation Waveforms
 Do No Harm Ventilate Gently Guide to Understand Mechanical Ventilation Waveforms Middle East Critical Care Assembly 1/30/2015 Mazen Kherallah, MD, FCCP http://www.mecriticalcare.net Email: info@mecriticalcare.net
Do No Harm Ventilate Gently Guide to Understand Mechanical Ventilation Waveforms Middle East Critical Care Assembly 1/30/2015 Mazen Kherallah, MD, FCCP http://www.mecriticalcare.net Email: info@mecriticalcare.net
Accumulation of EEV Barotrauma Affect hemodynamic Hypoxemia Hypercapnia Increase WOB Unable to trigger MV
 Complicated cases during mechanical ventilation Pongdhep Theerawit M.D. Pulmonary and Critical Care Division Ramathibodi Hospital Case I Presentation Male COPD 50 YO, respiratory failure, on mechanical
Complicated cases during mechanical ventilation Pongdhep Theerawit M.D. Pulmonary and Critical Care Division Ramathibodi Hospital Case I Presentation Male COPD 50 YO, respiratory failure, on mechanical
 http://www.priory.com/cmol/hfov.htm INTRODUCTION The vast majority of patients who are admitted to an Intensive Care Unit (ICU) will need artificial ventilation (Jones et al 1998). The usual means through
http://www.priory.com/cmol/hfov.htm INTRODUCTION The vast majority of patients who are admitted to an Intensive Care Unit (ICU) will need artificial ventilation (Jones et al 1998). The usual means through
RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Pulmonary Function and
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Pulmonary Function and
Respiratory Failure & Mechanical Ventilation. Denver Health Medical Center Department of Surgery and the University Of Colorado Denver
 Respiratory Failure & Mechanical Ventilation Denver Health Medical Center Department of Surgery and the University Of Colorado Denver + + Failure of the Respiratory Pump 1. Lack of patent airway 2. Bronchospasm
Respiratory Failure & Mechanical Ventilation Denver Health Medical Center Department of Surgery and the University Of Colorado Denver + + Failure of the Respiratory Pump 1. Lack of patent airway 2. Bronchospasm
Physiological Basis of Mechanical Ventilation
 Physiological Basis of Mechanical Ventilation Wally Carlo, M.D. University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu Fine Tuning Mechanical Ventilation
Physiological Basis of Mechanical Ventilation Wally Carlo, M.D. University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu Fine Tuning Mechanical Ventilation
Conflict of Interest Disclosure Robert M Kacmarek
 The Impact of Asynchrony on Patient Outcomes Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 6-1-15 CSRT Conflict of Interest Disclosure Robert M Kacmarek
The Impact of Asynchrony on Patient Outcomes Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts 6-1-15 CSRT Conflict of Interest Disclosure Robert M Kacmarek
3100A Competency Exam
 NAME DATE (Circle the appropriate answer) 3100A Competency Exam 1. Of the following, which best describes the mechanics of ventilation used by the 3100A? a. Active inspiration with passive exhalation b.
NAME DATE (Circle the appropriate answer) 3100A Competency Exam 1. Of the following, which best describes the mechanics of ventilation used by the 3100A? a. Active inspiration with passive exhalation b.
What is an Optimal Paw Strategy?
 What is an Optimal Paw Strategy? A Physiological Rationale Anastasia Pellicano Neonatologist Royal Children s Hospital, Melbourne Acute injury sequence Barotrauma Volutrauma Atelectotrauma Biotrauma Oxidative
What is an Optimal Paw Strategy? A Physiological Rationale Anastasia Pellicano Neonatologist Royal Children s Hospital, Melbourne Acute injury sequence Barotrauma Volutrauma Atelectotrauma Biotrauma Oxidative
Principles of mechanical ventilation. Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands
 Principles of mechanical ventilation Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands Disclosure Research grant Chiesi Pharmaceuticals Research grant CareFusion GA: 27 weeks,
Principles of mechanical ventilation Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands Disclosure Research grant Chiesi Pharmaceuticals Research grant CareFusion GA: 27 weeks,
Advanced Ventilator Modes. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine
 Advanced Ventilator Modes Shekhar T. Venkataraman M.D. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Advanced modes Pressure-Regulated
Advanced Ventilator Modes Shekhar T. Venkataraman M.D. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Advanced modes Pressure-Regulated
Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X
 HELICOPTER OPERATING PROCEDURE HOP No: C/12 Issued: May 2011 Page: 1 of 5 Revision No: Original Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X TRIM No: 09/300 Document No: D10/9973 X
HELICOPTER OPERATING PROCEDURE HOP No: C/12 Issued: May 2011 Page: 1 of 5 Revision No: Original Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X TRIM No: 09/300 Document No: D10/9973 X
Potential Conflicts of Interest Received research grants from Hamilton, Covidien, Drager, General lel Electric, Newport, and Cardinal Medical Received
 How Does a Mechanical Ventilator t 6-22-10 Spain Work? Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts Potential Conflicts of Interest Received research
How Does a Mechanical Ventilator t 6-22-10 Spain Work? Bob Kacmarek PhD, RRT Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts Potential Conflicts of Interest Received research
Mechanical Ventilation 2016
 Conflict of Interest Disclosure Robert M Kacmarek Lung Protective Ventilation: New Information RT s Neec to Know 5-6-17 FOCUS Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital
Conflict of Interest Disclosure Robert M Kacmarek Lung Protective Ventilation: New Information RT s Neec to Know 5-6-17 FOCUS Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital
Prof. Javier García Fernández MD, Ph.D, MBA.
 Prof. Javier García Fernández MD, Ph.D, MBA. Chairman of Anesthesia & Perioperative Medicine Department Puerta de Hierro Universitary Hospital Prof. of Anaesthesia and Perioperative Medicine. Autonoma
Prof. Javier García Fernández MD, Ph.D, MBA. Chairman of Anesthesia & Perioperative Medicine Department Puerta de Hierro Universitary Hospital Prof. of Anaesthesia and Perioperative Medicine. Autonoma
UNDERSTANDING NEONATAL WAVEFORM GRAPHICS. Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services
 UNDERSTANDING NEONATAL WAVEFORM GRAPHICS Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services Disclosures Purpose: To enhance bedside staff s knowledge of ventilation and oxygenation
UNDERSTANDING NEONATAL WAVEFORM GRAPHICS Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services Disclosures Purpose: To enhance bedside staff s knowledge of ventilation and oxygenation
Underlying Principles of Mechanical Ventilation: An Evidence-Based Approach
 Underlying Principles of Mechanical Ventilation: An Evidence-Based Approach Ira M. Cheifetz, MD, FCCM, FAARC Professor of Pediatrics and Anesthesiology Chief Medical Officer, Children s Services Associate
Underlying Principles of Mechanical Ventilation: An Evidence-Based Approach Ira M. Cheifetz, MD, FCCM, FAARC Professor of Pediatrics and Anesthesiology Chief Medical Officer, Children s Services Associate
Driving Pressure. What is it, and why should you care?
 Driving Pressure What is it, and why should you care? Jonathan Pak MD March 2, 2017 Lancet 1967; 290: 319-323 Traditional Ventilation in ARDS Tidal Volume (V T ) = 10-15 ml/kg PBW PEEP = 5-12 cm H 2 O
Driving Pressure What is it, and why should you care? Jonathan Pak MD March 2, 2017 Lancet 1967; 290: 319-323 Traditional Ventilation in ARDS Tidal Volume (V T ) = 10-15 ml/kg PBW PEEP = 5-12 cm H 2 O
NOTE: If not used, provider must document reason(s) for deferring mechanical ventilation in a patient with an advanced airway
 for deferring mechanical ventilation in a patient with an advanced airway") APPENDIX: TITLE: Mechanical Ventilator Use REVISED: November 1, 2017 I. Introduction: Mechanical Ventilation is the use of an automated device to deliver positive pressure ventilation to a patient. Proper
APPENDIX: TITLE: Mechanical Ventilator Use REVISED: November 1, 2017 I. Introduction: Mechanical Ventilation is the use of an automated device to deliver positive pressure ventilation to a patient. Proper
Ventilating the Sick Lung Mike Dougherty RRT-NPS
 Ventilating the Sick Lung 2018 Mike Dougherty RRT-NPS Goals and Objectives Discuss some Core Principles of Ventilation relevant to mechanical ventilation moving forward. Compare and Contrast High MAP strategies
Ventilating the Sick Lung 2018 Mike Dougherty RRT-NPS Goals and Objectives Discuss some Core Principles of Ventilation relevant to mechanical ventilation moving forward. Compare and Contrast High MAP strategies
mechanical ventilation Arjun Srinivasan
 Respiratory mechanics in mechanical ventilation Arjun Srinivasan Introduction Mechanics during ventilation PV curves Application in health & disease Difficulties & pitfalls The future. Monitoring Mechanics
Respiratory mechanics in mechanical ventilation Arjun Srinivasan Introduction Mechanics during ventilation PV curves Application in health & disease Difficulties & pitfalls The future. Monitoring Mechanics
Disclosures. The Pediatric Challenge. Topics for Discussion. Traditional Anesthesia Machine. Tidal Volume = mls/kg 2/13/14
 2/13/14 Disclosures Optimal Ventilation of the Pediatric Patient in the OR Consulting Draeger Medical Jeffrey M. Feldman, MD, MSE Division Chief, General Anesthesia Dept. of Anesthesiology and Critical
2/13/14 Disclosures Optimal Ventilation of the Pediatric Patient in the OR Consulting Draeger Medical Jeffrey M. Feldman, MD, MSE Division Chief, General Anesthesia Dept. of Anesthesiology and Critical
Managing Patient-Ventilator Interaction in Pediatrics
 Managing Patient-Ventilator Interaction in Pediatrics Robert L. Chatburn, MHHS, RRT-NPS, FAARC Clinical Research Manager - Section of Respiratory Therapy Professor of Medicine Case Western Reserve University
Managing Patient-Ventilator Interaction in Pediatrics Robert L. Chatburn, MHHS, RRT-NPS, FAARC Clinical Research Manager - Section of Respiratory Therapy Professor of Medicine Case Western Reserve University
Mechanical Ventilation. Flow-Triggering. Flow-Triggering. Advanced Concepts. Advanced Concepts in Mechanical Ventilation
 Mechanical Ventilation Advanced Concepts in Mechanical Ventilation Flow-Triggering Trigger = the variable that causes the vent to begin the inspiratory phase Common triggers 1-2- 3- Effort required to
Mechanical Ventilation Advanced Concepts in Mechanical Ventilation Flow-Triggering Trigger = the variable that causes the vent to begin the inspiratory phase Common triggers 1-2- 3- Effort required to
EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES
 GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
RSPT 1060 OBJECTIVES OBJECTIVES OBJECTIVES EQUATION OF MOTION. MODULE C Applied Physics Lesson #1 - Mechanics. Ventilation vs.
 RSPT 1060 MODULE C Applied Physics Lesson #1 - Mechanics OBJECTIVES At the end of this module, the student should be able to define the terms and abbreviations used in the module. draw & explain the equation
RSPT 1060 MODULE C Applied Physics Lesson #1 - Mechanics OBJECTIVES At the end of this module, the student should be able to define the terms and abbreviations used in the module. draw & explain the equation
How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital. Synopsis
 How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital Synopsis Definition of an oscillator Historical perspective Differences between HFOV and CMV Determinants
How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital Synopsis Definition of an oscillator Historical perspective Differences between HFOV and CMV Determinants
Pressure Controlled Modes of Mechanical Ventilation
 Pressure Controlled Modes of Mechanical Ventilation Christopher Junker Department of Anesthesiology & Critical Care Medicine George Washington University Saturday, August 20, 2011 Assist Control Hypoxemic
Pressure Controlled Modes of Mechanical Ventilation Christopher Junker Department of Anesthesiology & Critical Care Medicine George Washington University Saturday, August 20, 2011 Assist Control Hypoxemic
PART EIGHT HIGH FREQUENCY PERCUSSIVE OSCILLATION (HFPOV )
") PART EIGHT HIGH FREQUENCY PERCUSSIVE OSCILLATION (HFPOV ) Note: For maximal comparative understanding, FIRST read PART SEVEN which defines the concept of High Frequency Oscillatory Ventilation (HFOV).
PART EIGHT HIGH FREQUENCY PERCUSSIVE OSCILLATION (HFPOV ) Note: For maximal comparative understanding, FIRST read PART SEVEN which defines the concept of High Frequency Oscillatory Ventilation (HFOV).
Flight Medical presents the F60
 Flight Medical presents the F60 Reliable Ventilation Across the Spectrum of Care Adult & Pediatric Pressure/Volume Control Basic/Advanced Modes Invasive/NIV High Pressure/Low Flow O2 Up to 12 hours batteries
Flight Medical presents the F60 Reliable Ventilation Across the Spectrum of Care Adult & Pediatric Pressure/Volume Control Basic/Advanced Modes Invasive/NIV High Pressure/Low Flow O2 Up to 12 hours batteries
VENTILATORS PURPOSE OBJECTIVES
 VENTILATORS PURPOSE To familiarize and acquaint the transfer Paramedic with the skills and knowledge necessary to adequately maintain a ventilator in the interfacility transfer environment. COGNITIVE OBJECTIVES
VENTILATORS PURPOSE To familiarize and acquaint the transfer Paramedic with the skills and knowledge necessary to adequately maintain a ventilator in the interfacility transfer environment. COGNITIVE OBJECTIVES
Bunnell LifePulse HFV Quick Reference Guide # Bunnell Incorporated
 Bunnell Incorporated n www.bunl.com n 800-800-4358 (HFJV) n info@bunl.com 436 Lawndale Drive n Salt Lake City, Utah 84115 n intl 801-467-0800 n f 801-467-0867 Bunnell LifePulse HFV Quick Reference Guide
Bunnell Incorporated n www.bunl.com n 800-800-4358 (HFJV) n info@bunl.com 436 Lawndale Drive n Salt Lake City, Utah 84115 n intl 801-467-0800 n f 801-467-0867 Bunnell LifePulse HFV Quick Reference Guide
INTELLiVENT -ASV. The world s first Ventilation Autopilot
 INTELLiVENT -ASV The world s first Ventilation Autopilot Intelligent Ventilation since 1983 We live for ventilation technology We live for ventilation technology that helps caregivers improve the lives
INTELLiVENT -ASV The world s first Ventilation Autopilot Intelligent Ventilation since 1983 We live for ventilation technology We live for ventilation technology that helps caregivers improve the lives
Invasive mechanical ventilation:
 Invasive mechanical ventilation definition mechanical ventilation: using an apparatus to facilitate transport of oxygen and CO2 between the atmosphere and the alveoli for the purpose of enhancing pulmonary
Invasive mechanical ventilation definition mechanical ventilation: using an apparatus to facilitate transport of oxygen and CO2 between the atmosphere and the alveoli for the purpose of enhancing pulmonary
6 th Accredited Advanced Mechanical Ventilation Course for Anesthesiologists. Course Test Results for the accreditation of the acquired knowledge
 6 th Accredited Advanced Mechanical Ventilation Course for Anesthesiologists Course Test Results for the accreditation of the acquired knowledge Q. Concerning the mechanics of the newborn s respiratory
6 th Accredited Advanced Mechanical Ventilation Course for Anesthesiologists Course Test Results for the accreditation of the acquired knowledge Q. Concerning the mechanics of the newborn s respiratory
Introduction to Conventional Ventilation
 Introduction to Conventional Ventilation Dr Julian Eason Consultant Neonatologist Derriford Hospital Mechanics Inspiration diaphragm lowers and thorax expands Negative intrathoracic/intrapleural pressure
Introduction to Conventional Ventilation Dr Julian Eason Consultant Neonatologist Derriford Hospital Mechanics Inspiration diaphragm lowers and thorax expands Negative intrathoracic/intrapleural pressure
MEDICAL EQUIPMENT IV MECHANICAL VENTILATORS. Prof. Yasser Mostafa Kadah
 MEDICAL EQUIPMENT IV - 2013 MECHANICAL VENTILATORS Prof. Yasser Mostafa Kadah Mechanical Ventilator A ventilator is a machine, a system of related elements designed to alter, transmit, and direct energy
MEDICAL EQUIPMENT IV - 2013 MECHANICAL VENTILATORS Prof. Yasser Mostafa Kadah Mechanical Ventilator A ventilator is a machine, a system of related elements designed to alter, transmit, and direct energy
SAFE MECHANICAL VENTILATION: WHAT YOU NEED TO KNOW AND DO.
 SAFE MECHANICAL VENTILATION: WHAT YOU NEED TO KNOW AND DO. Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine holets.steven@mayo.edu OBJECTIVES: Describe the physiology
SAFE MECHANICAL VENTILATION: WHAT YOU NEED TO KNOW AND DO. Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine holets.steven@mayo.edu OBJECTIVES: Describe the physiology
Ventilators. Dr Simon Walton Consultant Anaesthetist Eastbourne DGH KSS Basic Science Course
 Ventilators Dr Simon Walton Consultant Anaesthetist Eastbourne DGH KSS Basic Science Course Objectives Discuss Classification/ terminology Look at Modes of ventilation How some specific ventilators work
Ventilators Dr Simon Walton Consultant Anaesthetist Eastbourne DGH KSS Basic Science Course Objectives Discuss Classification/ terminology Look at Modes of ventilation How some specific ventilators work
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo
 Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
SUPPLEMENTARY APPENDIX. Ary Serpa Neto MD MSc, Fabienne D Simonis MD, Carmen SV Barbas MD PhD, Michelle Biehl MD, Rogier M Determann MD PhD, Jonathan
 1 LUNG PROTECTIVE VENTILATION WITH LOW TIDAL VOLUMES AND THE OCCURRENCE OF PULMONARY COMPLICATIONS IN PATIENTS WITHOUT ARDS: a systematic review and individual patient data metaanalysis SUPPLEMENTARY APPENDIX
1 LUNG PROTECTIVE VENTILATION WITH LOW TIDAL VOLUMES AND THE OCCURRENCE OF PULMONARY COMPLICATIONS IN PATIENTS WITHOUT ARDS: a systematic review and individual patient data metaanalysis SUPPLEMENTARY APPENDIX
Physiology Unit 4 RESPIRATORY PHYSIOLOGY
 Physiology Unit 4 RESPIRATORY PHYSIOLOGY In Physiology Today Respiration External respiration ventilation gas exchange Internal respiration cellular respiration gas exchange Respiratory Cycle Inspiration
Physiology Unit 4 RESPIRATORY PHYSIOLOGY In Physiology Today Respiration External respiration ventilation gas exchange Internal respiration cellular respiration gas exchange Respiratory Cycle Inspiration
TESTCHEST RESPIRATORY FLIGHT SIMULATOR SIMULATION CENTER MAINZ
 TESTCHEST RESPIRATORY FLIGHT SIMULATOR SIMULATION CENTER MAINZ RESPIRATORY FLIGHT SIMULATOR TestChest the innovation of lung simulation provides a breakthrough in respiratory training. 2 Organis is the
TESTCHEST RESPIRATORY FLIGHT SIMULATOR SIMULATION CENTER MAINZ RESPIRATORY FLIGHT SIMULATOR TestChest the innovation of lung simulation provides a breakthrough in respiratory training. 2 Organis is the
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate
 Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate
 Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Talmor D, Sarge T, Malhotra A, et al. Mechanical ventilation
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Talmor D, Sarge T, Malhotra A, et al. Mechanical ventilation
Capnography in the Veterinary Technician Toolbox. Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA
 Capnography in the Veterinary Technician Toolbox Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA What are Respiration and Ventilation? Respiration includes all those chemical and physical
Capnography in the Veterinary Technician Toolbox Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA What are Respiration and Ventilation? Respiration includes all those chemical and physical
Using Common Ventilator Graphics to Provide Optimal Ventilation
 Using Common Ventilator Graphics to Provide Optimal Ventilation David Vines, MHS, RRT, FAARC Associate Professor Chair / Program Director Department of Respiratory Care RUSH UNIVERSITY MEDICAL CENTER Disclosure
Using Common Ventilator Graphics to Provide Optimal Ventilation David Vines, MHS, RRT, FAARC Associate Professor Chair / Program Director Department of Respiratory Care RUSH UNIVERSITY MEDICAL CENTER Disclosure
Mechanical ven3la3on. Neonatal Mechanical Ven3la3on. Mechanical ven3la3on. Mechanical ven3la3on. Mechanical ven3la3on 8/25/11. What we need to do"
 8/25/11 Mechanical ven3la3on Neonatal Mechanical Ven3la3on Support oxygen delivery, CO2 elimination" Prevent added injury, decrease ongoing injury" Enhance normal development" Mark C Mammel, MD University
8/25/11 Mechanical ven3la3on Neonatal Mechanical Ven3la3on Support oxygen delivery, CO2 elimination" Prevent added injury, decrease ongoing injury" Enhance normal development" Mark C Mammel, MD University
 C CONFERENCIAS MAGISTRALES Vol. 34. Supl. 1 Abril-Junio 211 pp S293-S31 Perioperative ventilator management: Why it makes a difference Daniel R. Brown, PhD, MD, FCCM Chair, Division of Critical Care Medicine.
C CONFERENCIAS MAGISTRALES Vol. 34. Supl. 1 Abril-Junio 211 pp S293-S31 Perioperative ventilator management: Why it makes a difference Daniel R. Brown, PhD, MD, FCCM Chair, Division of Critical Care Medicine.
New Frontiers in Anesthesia Ventilation. Brent Dunworth, MSN, CRNA. Anesthesia Ventilation. New Frontiers in. The amount of gas delivered can be
 New Frontiers in Anesthesia Ventilation Senior Director, Nurse Anesthesia Department of Anesthesiology University of Pittsburgh Medical Center Content Outline 1 2 Anesthesia Evolution Anesthesia Evolution
New Frontiers in Anesthesia Ventilation Senior Director, Nurse Anesthesia Department of Anesthesiology University of Pittsburgh Medical Center Content Outline 1 2 Anesthesia Evolution Anesthesia Evolution
Neonatal Assisted Ventilation. Haresh Modi, M.D. Aspirus Wausau Hospital, Wausau, WI.
 Neonatal Assisted Ventilation Haresh Modi, M.D. Aspirus Wausau Hospital, Wausau, WI. History of Assisted Ventilation Negative pressure : Spirophore developed in 1876 with manual device to create negative
Neonatal Assisted Ventilation Haresh Modi, M.D. Aspirus Wausau Hospital, Wausau, WI. History of Assisted Ventilation Negative pressure : Spirophore developed in 1876 with manual device to create negative
Chapter 3: Invasive mechanical ventilation Stephen Lo
 Chapter 3: Invasive mechanical ventilation Stephen Lo Introduction Conventional mechanical ventilation is the delivery of positive pressure to the airway to allow removal of CO2 and delivery of O2. In
Chapter 3: Invasive mechanical ventilation Stephen Lo Introduction Conventional mechanical ventilation is the delivery of positive pressure to the airway to allow removal of CO2 and delivery of O2. In
Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo
 Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo Link full download: http://testbankcollection.com/download/pilbeams-mechanicalventilation-physiological-and-clinical-applications-5th-edition-test-bank-cairo
Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo Link full download: http://testbankcollection.com/download/pilbeams-mechanicalventilation-physiological-and-clinical-applications-5th-edition-test-bank-cairo
RESPIRATORY PHYSIOLOGY RELEVANT TO HFOV
 RESPIRATORY PHYSIOLOGY RELEVANT TO Physiology of CMV 1 What is? Ventilation using a relatively high continuous distending pressure at the airway opening, around which an oscillatory wave is generated to
RESPIRATORY PHYSIOLOGY RELEVANT TO Physiology of CMV 1 What is? Ventilation using a relatively high continuous distending pressure at the airway opening, around which an oscillatory wave is generated to
VENTILATION AND PERFUSION IN HEALTH AND DISEASE. Dr.HARIPRASAD VS
 VENTILATION AND PERFUSION IN HEALTH AND DISEASE Dr.HARIPRASAD VS Ventilation Total ventilation - total rate of air flow in and out of the lung during normal tidal breathing. Alveolar ventilation -represents
VENTILATION AND PERFUSION IN HEALTH AND DISEASE Dr.HARIPRASAD VS Ventilation Total ventilation - total rate of air flow in and out of the lung during normal tidal breathing. Alveolar ventilation -represents
New Modes of Ventilation. Dr. Zia Hashim
 New Modes of Ventilation Dr. Zia Hashim Mode Describes the specific combination of: control phase conditional variables Defined for spontaneous mandatory breaths Variable Control variable : Constant throughout
New Modes of Ventilation Dr. Zia Hashim Mode Describes the specific combination of: control phase conditional variables Defined for spontaneous mandatory breaths Variable Control variable : Constant throughout
What s new and exciting for Pediatric Mechanical ventilation?
 PMVF-ASMIC 2017 What s new and exciting for Pediatric Mechanical ventilation? Rujipat Samransamruajkit MD Professor of Pediatrics Chief of PICU KCMH, Faculty of Medicine Chulalongkorn U BKK, Thailand Introduction
PMVF-ASMIC 2017 What s new and exciting for Pediatric Mechanical ventilation? Rujipat Samransamruajkit MD Professor of Pediatrics Chief of PICU KCMH, Faculty of Medicine Chulalongkorn U BKK, Thailand Introduction
The physiological functions of respiration and circulation. Mechanics. exercise 7. Respiratory Volumes. Objectives
 exercise 7 Respiratory System Mechanics Objectives 1. To explain how the respiratory and circulatory systems work together to enable gas exchange among the lungs, blood, and body tissues 2. To define respiration,
exercise 7 Respiratory System Mechanics Objectives 1. To explain how the respiratory and circulatory systems work together to enable gas exchange among the lungs, blood, and body tissues 2. To define respiration,
Physiological based management of hypoxaemic respiratory failure
 Physiological based management of hypoxaemic respiratory failure David Tingay 1. Neonatal Research, Murdoch Children s Research Institute, Melbourne 2. Neonatology, Royal Children s Hospital 3. Dept of
Physiological based management of hypoxaemic respiratory failure David Tingay 1. Neonatal Research, Murdoch Children s Research Institute, Melbourne 2. Neonatology, Royal Children s Hospital 3. Dept of
PART SEVEN THE HISTORY AND APPLICATION OF HIGH FREQUENCY OSCILLATORY VENTILATION (HFOV)
") PART SEVEN THE HISTORY AND APPLICATION OF HIGH FREQUENCY OSCILLATORY VENTILATION (HFOV) Reciprocating pistons with an eccentric travel speed, moving to and fro within a cylinder (with a common inlet/outlet),
PART SEVEN THE HISTORY AND APPLICATION OF HIGH FREQUENCY OSCILLATORY VENTILATION (HFOV) Reciprocating pistons with an eccentric travel speed, moving to and fro within a cylinder (with a common inlet/outlet),
Respiratory Physiology. Adeyomoye O.I
 Respiratory Physiology By Adeyomoye O.I Outline Introduction Hypoxia Dyspnea Control of breathing Ventilation/perfusion ratios Respiratory/barometric changes in exercise Intra-pulmonary & intra-pleural
Respiratory Physiology By Adeyomoye O.I Outline Introduction Hypoxia Dyspnea Control of breathing Ventilation/perfusion ratios Respiratory/barometric changes in exercise Intra-pulmonary & intra-pleural
Respiration (revised 2006) Pulmonary Mechanics
 Pulmonary Mechanics") Respiration (revised 2006) Pulmonary Mechanics PUL 1. Diagram how pleural pressure, alveolar pressure, airflow, and lung volume change during a normal quiet breathing cycle. Identify on the figure the
Respiration (revised 2006) Pulmonary Mechanics PUL 1. Diagram how pleural pressure, alveolar pressure, airflow, and lung volume change during a normal quiet breathing cycle. Identify on the figure the
Introduction. Respiration. Chapter 10. Objectives. Objectives. The Respiratory System
 Introduction Respiration Chapter 10 The Respiratory System Provides a means of gas exchange between the environment and the body Plays a role in the regulation of acidbase balance during exercise Objectives
Introduction Respiration Chapter 10 The Respiratory System Provides a means of gas exchange between the environment and the body Plays a role in the regulation of acidbase balance during exercise Objectives
WHAT IS SAFE VENTILATION? Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine
 WHAT IS SAFE VENTILATION? Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine holets.steven@mayo.edu DISCLOSURES Past and present Advisory Boards: Resmed Philips/Respironics
WHAT IS SAFE VENTILATION? Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine holets.steven@mayo.edu DISCLOSURES Past and present Advisory Boards: Resmed Philips/Respironics
PART ONE CHAPTER ONE PRIMARY CONSIDERATIONS RELATING TO THE PHYSIOLOGICAL AND PHYSICAL ASPECTS OF THE MECHANICAL VENTILATION OF THE LUNG
 PART ONE CHAPTER ONE PRIMARY CONSIDERATIONS RELATING TO THE PHYSIOLOGICAL AND PHYSICAL ASPECTS OF THE MECHANICAL VENTILATION OF THE LUNG POSSIBLE ORIGIN OF THE MECHANICAL VENTILATION OF THE LUNG- The first
PART ONE CHAPTER ONE PRIMARY CONSIDERATIONS RELATING TO THE PHYSIOLOGICAL AND PHYSICAL ASPECTS OF THE MECHANICAL VENTILATION OF THE LUNG POSSIBLE ORIGIN OF THE MECHANICAL VENTILATION OF THE LUNG- The first
Respiratory System. Part 2
 Respiratory System Part 2 Respiration Exchange of gases between air and body cells Three steps 1. Ventilation 2. External respiration 3. Internal respiration Ventilation Pulmonary ventilation consists
Respiratory System Part 2 Respiration Exchange of gases between air and body cells Three steps 1. Ventilation 2. External respiration 3. Internal respiration Ventilation Pulmonary ventilation consists
carefusion.com CareFusion Yorba Linda, CA CareFusion
 CareFusion 22745 Savi Ranch Parkway Yorba Linda, CA 92887 800.231.2466 toll-free 714.283.2228 tel 714.283.8493 fax CareFusion Germany 234 GmbH Leibnizstrasse 7 97204 Hoechberg Germany +49 931 4972-0 tel
CareFusion 22745 Savi Ranch Parkway Yorba Linda, CA 92887 800.231.2466 toll-free 714.283.2228 tel 714.283.8493 fax CareFusion Germany 234 GmbH Leibnizstrasse 7 97204 Hoechberg Germany +49 931 4972-0 tel
Mechanical power and opening pressure. Fellowship training program Intensive Care Radboudumc, Nijmegen
 Mechanical power and opening pressure Fellowship training program Intensive Care Radboudumc, Nijmegen Mechanical power Energy applied to the lung: Ptp * V (Joule) Power = Energy per minute (J/min) Power
Mechanical power and opening pressure Fellowship training program Intensive Care Radboudumc, Nijmegen Mechanical power Energy applied to the lung: Ptp * V (Joule) Power = Energy per minute (J/min) Power
Volume Diffusion Respiration (VDR)
") Volume Diffusion Respiration (VDR) A therapy with many uses Jeffrey Pietz, MD April 15, 2016 VDR ventilation has been used to treat patients with: ARDS Meconium Aspiration Burn and Inhalation Injury RDS
Volume Diffusion Respiration (VDR) A therapy with many uses Jeffrey Pietz, MD April 15, 2016 VDR ventilation has been used to treat patients with: ARDS Meconium Aspiration Burn and Inhalation Injury RDS
Author: Thomas Sisson, MD, 2009
 Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author: Thomas Sisson, MD, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/