CEEA 2015, Kosice Luciano Gattinoni, MD, FRCP Università di Milano Fondazione IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy
|
|
|
- Clifton Andrews
- 5 years ago
- Views:
Transcription


1 ARDS and VILI CEEA 2015, Kosice Luciano Gattinoni, MD, FRCP Università di Milano Fondazione IRCCS Ca Granda Ospedale Maggiore Policlinico Milan, Italy

2
3 VILI 3
4 VILI What is due to the ventilator/ventilation: Tidal Volume Pressure change Flow rate Respiratory rate Energy Power What is due to the lung: Lung inhomogeneity Stress risers

5 Chest wall elastance Stiff Soft Soft Stiff ELL Ew ELL Ew 25 5 cmh 2 O E tot E tot

6 Driving pressure Drive the lungs Drive the chest wall On the ventilator Transpulmonary pressure Pleural pressure Paw = P L + Ppl
7 How to measure the pleural pressure

8 Esophageal and gastric baloon

9 Anatomical section of a frozen cadaver between the thoracic vertebra 8 and 9 Bo WJ, Wolfman NT, Krueger WA, Meschan I Basic Atlas of Sectional Anatomy with Correlated Imaging. 2nd edition; WB Saunders Co. page 99
 Inspiratory Expiratory 6 dogs, oleic acid Pelosi et al.")
10 PES and Ppl Ppl 1 Ppl 2 Ppl 3 Non dependent middle dependent Ppl (cmh 2 O) PES (cmh 2 O) Inspiratory Expiratory 6 dogs, oleic acid Pelosi et al. Am J Respir Crit Care Med pp , 2001


11 Stress and Strain F b L 0 DL a S=a*b Stress Strain s=f/s e=dl/l 0 Transpulmonary pressure V T /EELV
12 Clinical equivalents Stress PL transpulmonary pressure Strain V T / FRC The linkage is the specific elastance PL E = lspec * V T FRC Barotrauma Volotrauma
13 DTranspulmonary Pressure (cm H 2 O) Specific lung elastance in ARDS is normal Control subjects (30) 26 ALI/ARDS patients (50) Lung Strain
14 DTranspulmonary plateau pressue (cmh 2 O) A Surgical control group Medical control group B ALI patients ARDS patients Airway plateau pressure (cmh 2 O) Airway plateau pressure (cmh 2 O) Chiumello et al, Am J Respir Crit Care Med. 2008
15 %Total Lung Capacity Percentage Resting Biotrauma Stress at rupture 3V ALI/ARDS 30 Healthy sbj 20 2V Specific Lung Elastance 12 (cmh 2 O) V Transpulmonary pressure (PL cmh 2 O)
16 Peripheral FRC 80% TLC
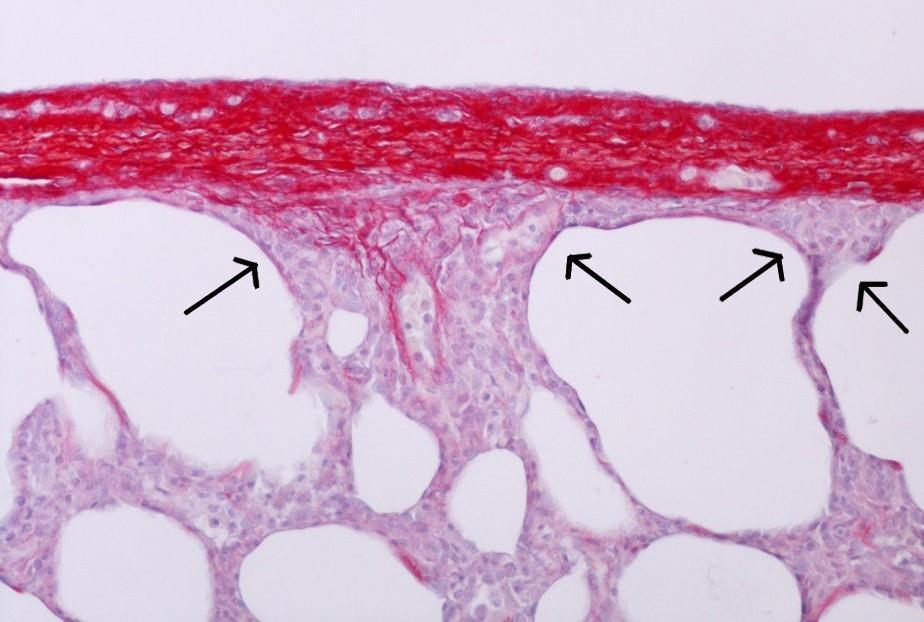
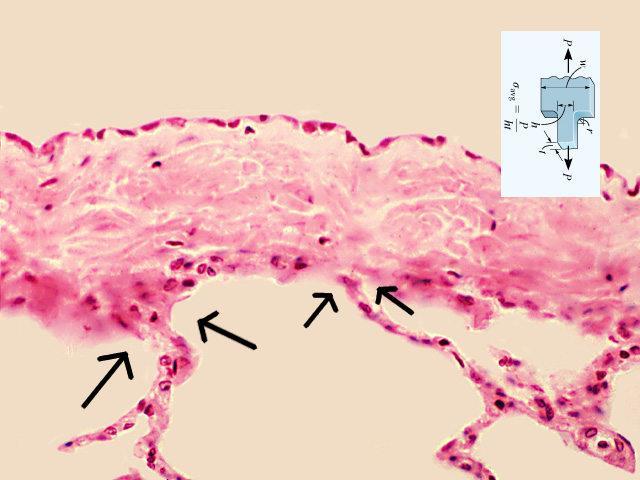
 Elastin fiber network in the respiratory bronchioli (RB) and in the alveolar duct (AD) (scale bar 200 μm) Toshima et al. Arch Histol Cytol.")
17 AS =alveolar sac P=pleura V=blood vessel Continuum of elastin fiber network (scale bar 200 μm) Elastin fiber network in the outer surface of the pleura (scale bar 10 μm) Elastin fiber network in the respiratory bronchioli (RB) and in the alveolar duct (AD) (scale bar 200 μm) Toshima et al. Arch Histol Cytol. 67(1):31-40 (2004)
 Toshima et al. Arch Histol Cytol.")
18 Collagen fiber network in rat lung Collapsed Inflated AE =alveolar entrances (scale bar 100 μm) Toshima et al. Arch Histol Cytol. 67(1):31-40 (2004)
19 Time course of ventilator induced lung injury DLung Weight (g) Strain (Vt/FRC) Hours of mechanical ventilation 0.5 Protti A. et al. Am J Respir Crit Care Med Feb 4.
20 Stress-strain curve of healthy pigs Stress (PL, cmh2o) Specific Lung Elastance 5.8 cmh 2 O Strain (dvgas/vgas0) Protti A. et al. Am J Respir Crit Care Med Feb 4.
21 Volumes and Pressures FRC [ml] TLC [ml] TLC/FRC Espec [cmh 2 O] PL to TLC [cmh 2 O] MICE ?? RATS PIGS MEN
22 Lung Volume TLC FRC VT 100% V PEEP 0% VT 75% V PEEP 25% VT 50% V PEEP 50% VT 25% V PEEP 75% Protti et al. Crit Care Med Feb 4.
23 Tidal Strain P*ΔV = Energy Input Dissipated Surface Tension Sliding EM Opening and Closing Undissipated Elastic System Continuous Strain PEEP *ΔV = Energy Input = 0
24 ZEEP 600 Total Inspiratory Volume Volume EXAPLES OF ENERGY COMPUTATIONS AT DIFFERENT PRESSURES 0 ZEEP Peak Pressure Pressure Total Inspiratory Volume LOW PEEP Total Inspiratory Volume HIGH PEEP PEEP Volume Volume 600 PEEP Volume Volume PEEP Peak Pressure 0 PEEP Peak Pressure Pressure Pressure
25 76 PIGS 10 Total Peak Power SURVIVED Total Peak Power DEAD Dynamic Peak Power SURVIVED Dynamic Peak Power DEAD 8 Power (Watt) SURVIVED DEAD SURVIVED DEAD SURVIVED DEAD LOW INTERMEDIATE HIGH
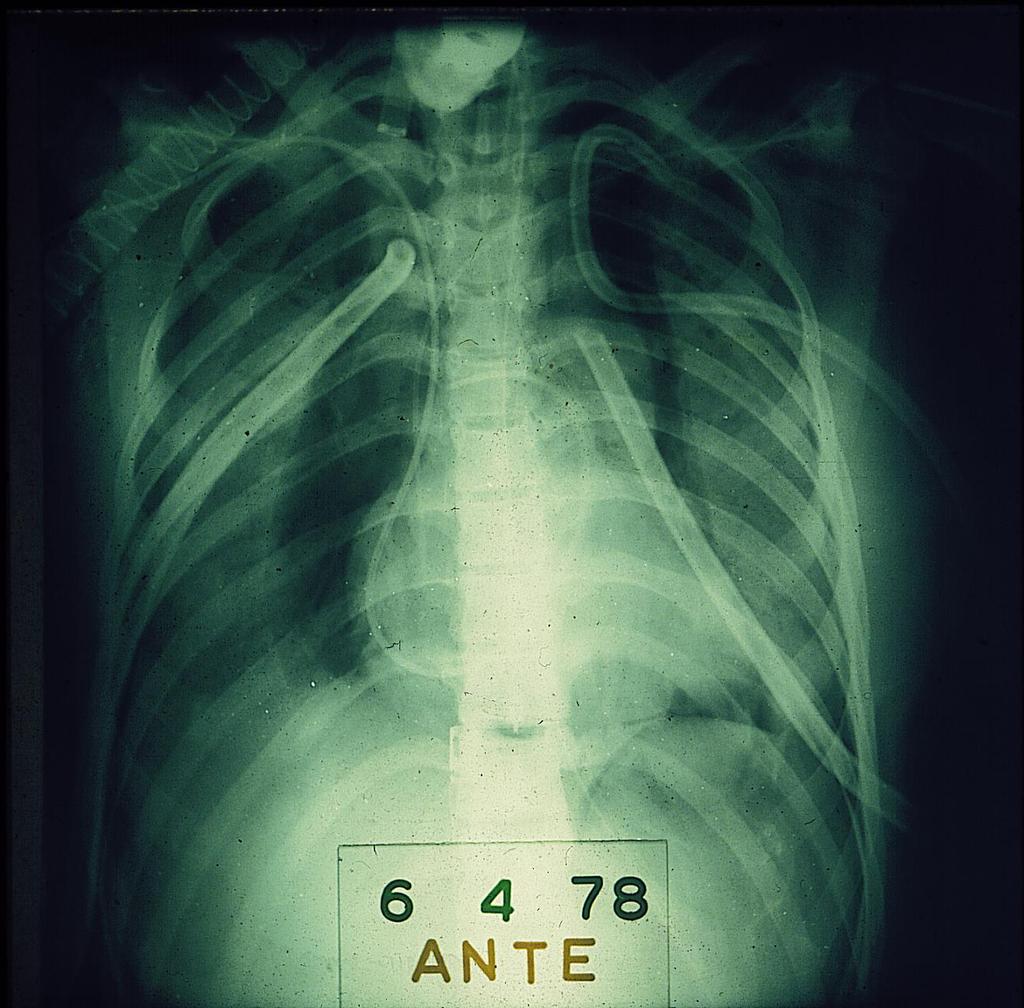
26 Tidal volume 38 ml/kg Plateau pressure 27 cmh 2 O Lethal in 54 hours 15 breaths/min but RESPIRATORY RATE - 3 breaths/min - 6 breaths/min - 9 breaths/min - 12 breaths/min - 15 breaths/min
27 Baseline
28 After 12 hours
29 After 45 hours
30 After 50 hours!




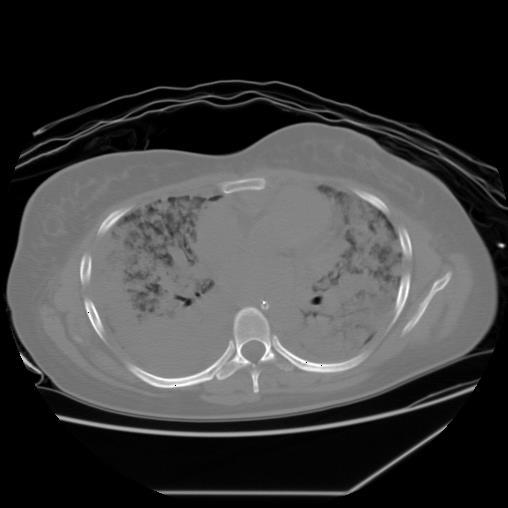
31 Whole lung edema One-field edema Isolated densities Baseline Delivered dynamic transpulmonary energy load (J/min)
32 Volume (ml) Volume (ml) RR3 RR6 RR9 RR12 RR15 Paw (cmh 2 O) Start End Paw (cmh 2 O)
33 Therefore VILI arises from mechanical power: PL TV RR
34 VILI What is due to the ventilator/ventilation: Tidal Volume Pressure change Flow rate Respiratory rate Energy Power What is due to the lung: Lung inhomogeneity Stress risers
35 f=f/3 VILI 28 HOMOGENEOUS SYSTEM F f=f/3 f=f/3 L 0 +DL HOMOGENEOUS f<f/3 F f>>f/3 f<f/3 L 0 +DL INCLUSION RUPTURE F f=f/2 f=0 f=f/2 L. Gattinoni, 2003 L 0 +DL RUPTURE
36 Stress distribution: homogeneous system VILI 29 F T min max Mead J et al. J. Appl. Physiol. 28(5):
37 Stress distribution: VILI 30 high stiffness zone min max Mead J et al. J. Appl. Physiol. 28(5):
38 Voxel Vgas Gas fraction = V gas0 /V voxel Weighted gas ratio = V gas1 /V gas0 * fraction of tissue Cressoni et al. Am J Respir Crit Care Med Jan 15;189(2):149-58





39 Average ratio in normal subjects : 1.37±0.15 Healthy subject Moderate ARDS Severe ARDS
40 Lung expansion from F a gas-free state F F V V V Homogeneous lung F F F V V STRESS RISER
41 Stress risers and shape
42 Lung dishomogeneity and ARDS Mild (N=82) Moderate (N=71) Severe (N=12) P Dishomogeneity 1.49 ± ± ± Dishomogeneity 2/ ± ± ± 0.55 Extent 0.3 ± ± ± Intensity 2.69 ± ± ± Intensity 2/ ± ± ± 0.55 Courtesy of Dr. Cressoni
43
44 Hypothesis Lesions should first occur where physiological stress risers are located

![[57-76]%](/docs-images/87/96975315/images/45-1.jpg "Peribronchial 19")
![[11-23]% Courtesy](/docs-images/87/96975315/images/45-2.jpg "of dr. Cressoni M.")
45 KIND OF DENSITIES Subpleural 61 [57-76]% Peribronchial 19 [11-23]% Courtesy of dr. Cressoni M. Parenchymal 19 [6-25]%

46 Before appearance first new densities END EXPIRATION END INSPIRATION TIME 1: 5.7±6.5 hours Courtesy of dr. Cressoni M.

47 First CT scan with new densities END EXPIRATION END INSPIRATION TIME 2: 8.4±6.3 hours Courtesy of dr. Cressoni M.
48 Last CT scan with distinguishable densities END EXPIRATION END INSPIRATION TIME 3: 15±12 hours Courtesy of dr. Cressoni M.

49 First CT scan with one-field edema END EXPIRATION END INSPIRATION TIME 4: 18±11 hours Courtesy of dr. Cressoni M.
50 First CT scan with all-field edema END EXPIRATION END INSPIRATION TIME 5: 20±11 hours Courtesy of dr. Cressoni M.
51 Severity trend VILI cumulative time course T4-5 + Gas Exchange T3 + Lung mechanics T2 CT scan only Hours Courtesy of dr. Cressoni M.



52 CT SCAN INFLATION LUNG IMAGING INHOMOGENEITY PET FDG UPTAKE

53 Ki/lung inhomogeneity interaction and gas/tissue composition MILD MODERATE SEVERE
54 Prevention of VILI Decrease mechanical power Tidal Volume Pressure variation Respiratory rate Flow Increasing Homogeneity PEEP Prone Position
55 Lung protective strategy Less energy + More homogeneous lung
56 Lung protective strategy recipe: the ingredients Assess severity Select Tidal Volume Select PEEP Select RR-IE Watch hemodynamics
57 Lung and gasless tissue weight in acute respiratory failure n=39 n=34 n=34 n=34 lung tissue weight [gr] total lung tissue non-aerated lung tissue * * * * * * Healthy lungs Unilateral pneumonia ALI/ARDS: lower-potential for lung recruitment ALI/ARDS: higher-potential for lung recruitment Submitted for publication * P<0.01 vs. patients with healthy lungs, P<0.01 vs. other groups.
58 Severity Edema Baby Lung Gas Exchange Lung Mechanics
59 Severity trend VILI cumulative time course T4-5 + Gas Exchange T3 + Lung mechanics T2 CT scan only Hours Courtesy of dr. Cressoni M.
60 PaO2/FiO2 at 5 cmh 2 O PEEP ARDS patients b[0] 235 b[1] r P < Lung weight at 5 cmh 2 O PEEP (grams)
61 Assess severity The simplest P/F at 5 cmh 2 O PEEP (300, 200, 100) Berlin definition
62 Lung protective strategy recipe: the ingredients Assess severity Select Tidal Volume Select PEEP Select RR-IE Watch hemodynamics
63 Lung gas volume and body weight Total gas volume at 5 cmh 2 O PEEP 5000 Mild Moderate 4000 Severe P=0.025 R 2 = Ideal body weight (kg)
64 The ARDS lung is small and not stiff Normal V T FRC = 500 ml 2500 ml = 0.2 ARDS V T FRC = 500 ml 500 ml = 1
65 Select tidal volume The simplest Tidal volume 6 ml/kg IBW (check plateau pressure)
66 Lung protective strategy recipe: the ingredients Assess severity Select Tidal Volume Select PEEP Select RR-IE Watch hemodynamics
67 Frequency [no. of patients] Figure 1 Potential for lung recruitment ± 4% (59 ± 51 grams) lower 21 ± 10% (374 ± 236 grams) higher ALI patients ARDS patients potential for lung recruitment [% total lung weight] Gattinoni L, Caironi P, Cressoni M, Chiumello D, Ranieri VM, Quintel M, Russo S, Cornejo R, Bugedo G, NEJM 2006, 354(17):
68 PEEP selection methods comparison CT scan derived PEEP Esophageal Pressure The Stress Index method The ExPress study The LOVs study
69 PEEP (cmh 2 O) Mild (n=7) ARDS Moderate (n=33) Severe (n=11) LOV ExPress 8±2 $ 11±3 $ 15±3 14±2 * 14±3 * 16±3 Stress Index Esophageal pressure 11±2 14±3 * 14±3 13±3 * 12±4 13±4 $ p<0.05 vs severe ARDS * p<0.05 vs LOV selection method p (method) <0.001 p (classification according to Berlin definition) 0.02 p (interaction) 0.01 Crit Care Med Feb;42(2):252-64
70 Superimposed pressure Superimposed pressure The same transpulmonary pressure is required to keep the lung open!!!
71 Select PEEP The simplest Mild ARDS: below 10 cmh O 2 Moderate: cmh O 2 Severe: >15 cmh O 2
72 ARDS Mild Moderate Severe Paw plat/pl plat 30 cmh 2 O/ 20 cmh 2 O Tidal Volume/strain 6 ml/kg IBW/ PEEP 10 cmh 2 O > 15 cmh 2 O ECMO ALTERNATIVE TREATMENTS ECCO 2 -R Neuromusc.Blockade Prone Position HFO
73 Thank you for your attention Grazie
Mechanical power and opening pressure. Fellowship training program Intensive Care Radboudumc, Nijmegen
 Mechanical power and opening pressure Fellowship training program Intensive Care Radboudumc, Nijmegen Mechanical power Energy applied to the lung: Ptp * V (Joule) Power = Energy per minute (J/min) Power
Mechanical power and opening pressure Fellowship training program Intensive Care Radboudumc, Nijmegen Mechanical power Energy applied to the lung: Ptp * V (Joule) Power = Energy per minute (J/min) Power
Pressure -Volume curves in ARDS. G. Servillo
 Pressure -Volume curves in ARDS G. Servillo Dipartimento di Scienze Chirurgiche, Anestesiologiche- Rianimatorie e dell Emergenza Facoltà di Medicina e Chirurgia Università degli Studi di Napoli Federico
Pressure -Volume curves in ARDS G. Servillo Dipartimento di Scienze Chirurgiche, Anestesiologiche- Rianimatorie e dell Emergenza Facoltà di Medicina e Chirurgia Università degli Studi di Napoli Federico
Mechanical Ventilation Guided by Esophageal Pressure in Acute Lung Injury *
 A teaching hospital of Harvard Medical School Mechanical Ventilation Guided by Esophageal Pressure in Acute Lung Injury * Ray Ritz BA RRT FAARC Beth Israel Deaconess Medical Center Boston MA * n engl j
A teaching hospital of Harvard Medical School Mechanical Ventilation Guided by Esophageal Pressure in Acute Lung Injury * Ray Ritz BA RRT FAARC Beth Israel Deaconess Medical Center Boston MA * n engl j
VENTILATOR-INDUCED lung injury (VILI) has. Mechanical Power and Development of Ventilator-induced Lung Injury CRITICAL CARE MEDICINE ABSTRACT
 has. Mechanical Power and Development of Ventilator-induced Lung Injury CRITICAL CARE MEDICINE ABSTRACT") Mechanical Power and Development of Ventilator-induced Lung Injury ABSTRACT Background: The ventilator works mechanically on the lung parenchyma. The authors set out to obtain the proof of concept that
Mechanical Power and Development of Ventilator-induced Lung Injury ABSTRACT Background: The ventilator works mechanically on the lung parenchyma. The authors set out to obtain the proof of concept that
Driving Pressure. What is it, and why should you care?
 Driving Pressure What is it, and why should you care? Jonathan Pak MD March 2, 2017 Lancet 1967; 290: 319-323 Traditional Ventilation in ARDS Tidal Volume (V T ) = 10-15 ml/kg PBW PEEP = 5-12 cm H 2 O
Driving Pressure What is it, and why should you care? Jonathan Pak MD March 2, 2017 Lancet 1967; 290: 319-323 Traditional Ventilation in ARDS Tidal Volume (V T ) = 10-15 ml/kg PBW PEEP = 5-12 cm H 2 O
What is Lung Protective Ventilation? NBART 2016
 What is Lung Protective Ventilation? NBART 2016 Disclosure Full time employee of Draeger Outline 1. Why talk about Lung Protective Ventilation? 2. What is Lung Protective Ventilation? 3. How to apply Lung
What is Lung Protective Ventilation? NBART 2016 Disclosure Full time employee of Draeger Outline 1. Why talk about Lung Protective Ventilation? 2. What is Lung Protective Ventilation? 3. How to apply Lung
Lung recruitment maneuvers
 White Paper Lung recruitment maneuvers Assessment of lung recruitability and performance of recruitment maneuvers using the P/V Tool Pro Munir A Karjaghli RRT, Clinical Application Specialist, Hamilton
White Paper Lung recruitment maneuvers Assessment of lung recruitability and performance of recruitment maneuvers using the P/V Tool Pro Munir A Karjaghli RRT, Clinical Application Specialist, Hamilton
Chapter 37: Pulmonary Ventilation. Chad & Angela
 Chapter 37: Pulmonary Ventilation Chad & Angela Respiratory Structures Basic Structures of Respiration Nasal/Oral Cavities Larynx Trachea Bronchi Secondary Bronchi Bronchioles Alveoli Mechanics of Ventilation
Chapter 37: Pulmonary Ventilation Chad & Angela Respiratory Structures Basic Structures of Respiration Nasal/Oral Cavities Larynx Trachea Bronchi Secondary Bronchi Bronchioles Alveoli Mechanics of Ventilation
Invasive Ventilation: State of the Art
 ARDSnet NEJM 2000;342:1301 9-30-17 Cox Invasive Ventilation: State of the Art Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts A V T of 6 ml/kg PBW results
ARDSnet NEJM 2000;342:1301 9-30-17 Cox Invasive Ventilation: State of the Art Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts A V T of 6 ml/kg PBW results
What is an Optimal Paw Strategy?
 What is an Optimal Paw Strategy? A Physiological Rationale Anastasia Pellicano Neonatologist Royal Children s Hospital, Melbourne Acute injury sequence Barotrauma Volutrauma Atelectotrauma Biotrauma Oxidative
What is an Optimal Paw Strategy? A Physiological Rationale Anastasia Pellicano Neonatologist Royal Children s Hospital, Melbourne Acute injury sequence Barotrauma Volutrauma Atelectotrauma Biotrauma Oxidative
RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Pulmonary Function and
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Pulmonary Function and
VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL
 VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National
VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National
High Frequency Ventilation. Neil MacIntyre MD Duke University Medical Center Durham NC USA
 High Frequency Ventilation Neil MacIntyre MD Duke University Medical Center Durham NC USA High frequency ventilation Concept of ventilator induced lung injury and lung protective ventilatory strategies
High Frequency Ventilation Neil MacIntyre MD Duke University Medical Center Durham NC USA High frequency ventilation Concept of ventilator induced lung injury and lung protective ventilatory strategies
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES
 INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES") INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
Sumit Ray Senior Consultant & Vice-Chair Critical Care & Emergency Medicine Sir Ganga Ram Hospital
 Sumit Ray Senior Consultant & Vice-Chair Critical Care & Emergency Medicine Sir Ganga Ram Hospital ARDS pathophysiology B Taylor Thompson et al. NEJM 2017;377:562-72. Outcome Australian Epidemiologic
Sumit Ray Senior Consultant & Vice-Chair Critical Care & Emergency Medicine Sir Ganga Ram Hospital ARDS pathophysiology B Taylor Thompson et al. NEJM 2017;377:562-72. Outcome Australian Epidemiologic
ONLINE DATA SUPPLEMENT. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg
 APPENDIX 1 Appendix 1. Complete respiratory protocol. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg predicted body weight (PBW)) (NEJM 2000; 342
APPENDIX 1 Appendix 1. Complete respiratory protocol. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg predicted body weight (PBW)) (NEJM 2000; 342
RESPIRATORY PHYSIOLOGY RELEVANT TO HFOV
 RESPIRATORY PHYSIOLOGY RELEVANT TO Physiology of CMV 1 What is? Ventilation using a relatively high continuous distending pressure at the airway opening, around which an oscillatory wave is generated to
RESPIRATORY PHYSIOLOGY RELEVANT TO Physiology of CMV 1 What is? Ventilation using a relatively high continuous distending pressure at the airway opening, around which an oscillatory wave is generated to
Prof. Javier García Fernández MD, Ph.D, MBA.
 Prof. Javier García Fernández MD, Ph.D, MBA. Chairman of Anesthesia & Perioperative Medicine Department Puerta de Hierro Universitary Hospital Prof. of Anaesthesia and Perioperative Medicine. Autonoma
Prof. Javier García Fernández MD, Ph.D, MBA. Chairman of Anesthesia & Perioperative Medicine Department Puerta de Hierro Universitary Hospital Prof. of Anaesthesia and Perioperative Medicine. Autonoma
Positive end-expiratory pressure Luciano Gattinoni a,b, Eleonora Carlesso b, Luca Brazzi a,b and Pietro Caironi a,b
 Positive end-expiratory pressure Luciano Gattinoni a,b, Eleonora Carlesso b, Luca Brazzi a,b and Pietro Caironi a,b a Dipartimento di Anestesia, Rianimazione (Intensiva e Subintensiva) e Terapia del Dolore,
Positive end-expiratory pressure Luciano Gattinoni a,b, Eleonora Carlesso b, Luca Brazzi a,b and Pietro Caironi a,b a Dipartimento di Anestesia, Rianimazione (Intensiva e Subintensiva) e Terapia del Dolore,
RSPT 1060 OBJECTIVES OBJECTIVES OBJECTIVES EQUATION OF MOTION. MODULE C Applied Physics Lesson #1 - Mechanics. Ventilation vs.
 RSPT 1060 MODULE C Applied Physics Lesson #1 - Mechanics OBJECTIVES At the end of this module, the student should be able to define the terms and abbreviations used in the module. draw & explain the equation
RSPT 1060 MODULE C Applied Physics Lesson #1 - Mechanics OBJECTIVES At the end of this module, the student should be able to define the terms and abbreviations used in the module. draw & explain the equation
Ventilating the Sick Lung Mike Dougherty RRT-NPS
 Ventilating the Sick Lung 2018 Mike Dougherty RRT-NPS Goals and Objectives Discuss some Core Principles of Ventilation relevant to mechanical ventilation moving forward. Compare and Contrast High MAP strategies
Ventilating the Sick Lung 2018 Mike Dougherty RRT-NPS Goals and Objectives Discuss some Core Principles of Ventilation relevant to mechanical ventilation moving forward. Compare and Contrast High MAP strategies
Presentation Overview. Monitoring Strategies for the Mechanically Ventilated Patient. Early Monitoring Strategies. Early Attempts To Monitor WOB
 Monitoring Strategies for the Mechanically entilated Patient Presentation Overview A look back into the future What works and what may work What s all the hype about the WOB? Are ventilator graphics really
Monitoring Strategies for the Mechanically entilated Patient Presentation Overview A look back into the future What works and what may work What s all the hype about the WOB? Are ventilator graphics really
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Talmor D, Sarge T, Malhotra A, et al. Mechanical ventilation
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Talmor D, Sarge T, Malhotra A, et al. Mechanical ventilation
APRV: Moving beyond ARDSnet
 APRV: Moving beyond ARDSnet Matthew Lissauer, MD Associate Professor of Surgery Medical Director, Surgical Critical Care Rutgers, The State University of New Jersey What is APRV? APRV is different from
APRV: Moving beyond ARDSnet Matthew Lissauer, MD Associate Professor of Surgery Medical Director, Surgical Critical Care Rutgers, The State University of New Jersey What is APRV? APRV is different from
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo
 Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
excellence in care Procedure Management of patients with difficult oxygenation. For Review Aug 2015
 Difficult Oxygenation HELI.CLI.12 Purpose This procedure describes the processes and procedures for a lung protective strategy in the mechanical ventilation of patients that are difficult to oxygenate
Difficult Oxygenation HELI.CLI.12 Purpose This procedure describes the processes and procedures for a lung protective strategy in the mechanical ventilation of patients that are difficult to oxygenate
Accumulation of EEV Barotrauma Affect hemodynamic Hypoxemia Hypercapnia Increase WOB Unable to trigger MV
 Complicated cases during mechanical ventilation Pongdhep Theerawit M.D. Pulmonary and Critical Care Division Ramathibodi Hospital Case I Presentation Male COPD 50 YO, respiratory failure, on mechanical
Complicated cases during mechanical ventilation Pongdhep Theerawit M.D. Pulmonary and Critical Care Division Ramathibodi Hospital Case I Presentation Male COPD 50 YO, respiratory failure, on mechanical
Why we should care (I)
") What the $*!# is Lung Protective Ventilation and Why Should I be Using it in the OR? Disclosures KATHERINE PALMIERI, MD, MBA 64 TH ANNUAL POSTGRADUATE SYMPOSIUM UNIVERSITY OF KANSAS MEDICAL CENTER DEPARTMENT
What the $*!# is Lung Protective Ventilation and Why Should I be Using it in the OR? Disclosures KATHERINE PALMIERI, MD, MBA 64 TH ANNUAL POSTGRADUATE SYMPOSIUM UNIVERSITY OF KANSAS MEDICAL CENTER DEPARTMENT
Advanced Ventilator Modes. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine
 Advanced Ventilator Modes Shekhar T. Venkataraman M.D. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Advanced modes Pressure-Regulated
Advanced Ventilator Modes Shekhar T. Venkataraman M.D. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Advanced modes Pressure-Regulated
Physiological Basis of Mechanical Ventilation
 Physiological Basis of Mechanical Ventilation Wally Carlo, M.D. University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu Fine Tuning Mechanical Ventilation
Physiological Basis of Mechanical Ventilation Wally Carlo, M.D. University of Alabama at Birmingham Department of Pediatrics Division of Neonatology wcarlo@peds.uab.edu Fine Tuning Mechanical Ventilation
The ARDSnet and Lung Protective Ventilation: Where Are We Today
 The ARDSnet and Lung Protective Ventilation: Where Are We Today 4-16-12 RCSW Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Disclosure
The ARDSnet and Lung Protective Ventilation: Where Are We Today 4-16-12 RCSW Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital Boston, Massachusetts Conflict of Interest Disclosure
Mechanical Ventilation of the Patient with ARDS
 1 Mechanical Ventilation of the Patient with ARDS Dean Hess, PhD, RRT, FAARC Assistant Professor of Anesthesia Harvard Medical School Assistant Director of Respiratory Care Massachusetts General Hospital
1 Mechanical Ventilation of the Patient with ARDS Dean Hess, PhD, RRT, FAARC Assistant Professor of Anesthesia Harvard Medical School Assistant Director of Respiratory Care Massachusetts General Hospital
Basics of Mechanical Ventilation. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of Mechanical Ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Overview of topics 1. Goals 2. Settings 3. Modes 4. Advantages and disadvantages
Basics of Mechanical Ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Overview of topics 1. Goals 2. Settings 3. Modes 4. Advantages and disadvantages
Model Based Approach to Estimate dfrc in the ICU Using Measured Lung Dynamics
 Model Based Approach to Estimate dfrc in the ICU Using Measured Lung Dynamics A.N. Mishra*, Y.S. Chiew*, J.G. Chase*, G.M. Shaw** *University of Canterbury, Christchurch, 8041, New Zealand (e-mail: ankit.mishra@pg.canterbury.ac.nz,
Model Based Approach to Estimate dfrc in the ICU Using Measured Lung Dynamics A.N. Mishra*, Y.S. Chiew*, J.G. Chase*, G.M. Shaw** *University of Canterbury, Christchurch, 8041, New Zealand (e-mail: ankit.mishra@pg.canterbury.ac.nz,
Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X
 HELICOPTER OPERATING PROCEDURE HOP No: C/12 Issued: May 2011 Page: 1 of 5 Revision No: Original Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X TRIM No: 09/300 Document No: D10/9973 X
HELICOPTER OPERATING PROCEDURE HOP No: C/12 Issued: May 2011 Page: 1 of 5 Revision No: Original Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X TRIM No: 09/300 Document No: D10/9973 X
Principles of mechanical ventilation. Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands
 Principles of mechanical ventilation Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands Disclosure Research grant Chiesi Pharmaceuticals Research grant CareFusion GA: 27 weeks,
Principles of mechanical ventilation Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands Disclosure Research grant Chiesi Pharmaceuticals Research grant CareFusion GA: 27 weeks,
Transpulmonary pressure: importance and limits
 Review Article Page 1 of 10 Transpulmonary pressure: importance and limits Domenico Luca Grieco 1,2,3, Lu Chen 1,2, Laurent Brochard 1,2 1 Interdepartmental Division of Critical Care Medicine, University
Review Article Page 1 of 10 Transpulmonary pressure: importance and limits Domenico Luca Grieco 1,2,3, Lu Chen 1,2, Laurent Brochard 1,2 1 Interdepartmental Division of Critical Care Medicine, University
Introduction. Respiration. Chapter 10. Objectives. Objectives. The Respiratory System
 Introduction Respiration Chapter 10 The Respiratory System Provides a means of gas exchange between the environment and the body Plays a role in the regulation of acidbase balance during exercise Objectives
Introduction Respiration Chapter 10 The Respiratory System Provides a means of gas exchange between the environment and the body Plays a role in the regulation of acidbase balance during exercise Objectives
Respiratory system. Role. Ventilation consists of 4 (5) steps : oxygen delivery and carbon dioxide elimination ph balance sound and voice formation
 steps : oxygen delivery and carbon dioxide elimination ph balance sound and voice formation") Respiratory system Role oxygen delivery and carbon dioxide elimination ph balance sound and voice formation Ventilation consists of 4 (5) steps : 1. pulmonary ventilation gas exchange between lungs and
Respiratory system Role oxygen delivery and carbon dioxide elimination ph balance sound and voice formation Ventilation consists of 4 (5) steps : 1. pulmonary ventilation gas exchange between lungs and
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate
 Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate
 Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia, Critical Care and Pain Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM Non-anaesthesiated healthy
Underlying Principles of Mechanical Ventilation: An Evidence-Based Approach
 Underlying Principles of Mechanical Ventilation: An Evidence-Based Approach Ira M. Cheifetz, MD, FCCM, FAARC Professor of Pediatrics and Anesthesiology Chief Medical Officer, Children s Services Associate
Underlying Principles of Mechanical Ventilation: An Evidence-Based Approach Ira M. Cheifetz, MD, FCCM, FAARC Professor of Pediatrics and Anesthesiology Chief Medical Officer, Children s Services Associate
PROBLEM SET 8. SOLUTIONS April 15, 2004
 Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Lung Opening and Closing during Ventilation of Acute Respiratory Distress Syndrome
 Lung Opening and Closing during Ventilation of Acute Respiratory Distress Syndrome Pietro Caironi 1,2, Massimo Cressoni 1, Davide Chiumello 2, Marco Ranieri 3, Michael Quintel 4, Sebastiano G. Russo 4,
Lung Opening and Closing during Ventilation of Acute Respiratory Distress Syndrome Pietro Caironi 1,2, Massimo Cressoni 1, Davide Chiumello 2, Marco Ranieri 3, Michael Quintel 4, Sebastiano G. Russo 4,
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia and Critical Care Service Puerta de Hierro University Hospital Associate Professor.
 Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia and Critical Care Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM CV and Conflict of interest Chairman
Javier García Fernández. MD. Ph.D. MBA. Chairman of Anaesthesia and Critical Care Service Puerta de Hierro University Hospital Associate Professor. Medical School. UAM CV and Conflict of interest Chairman
Collin County Community College. Lung Physiology
 Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 9 Respiratory System 1 Lung Physiology Factors affecting Ventillation 1. Airway resistance Flow = Δ P / R Most resistance is encountered
Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 9 Respiratory System 1 Lung Physiology Factors affecting Ventillation 1. Airway resistance Flow = Δ P / R Most resistance is encountered
Initiation and Management of Airway Pressure Release Ventilation (APRV)
") Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
SAFE MECHANICAL VENTILATION: WHAT YOU NEED TO KNOW AND DO.
 SAFE MECHANICAL VENTILATION: WHAT YOU NEED TO KNOW AND DO. Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine holets.steven@mayo.edu OBJECTIVES: Describe the physiology
SAFE MECHANICAL VENTILATION: WHAT YOU NEED TO KNOW AND DO. Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine holets.steven@mayo.edu OBJECTIVES: Describe the physiology
SUPPLEMENTARY APPENDIX. Ary Serpa Neto MD MSc, Fabienne D Simonis MD, Carmen SV Barbas MD PhD, Michelle Biehl MD, Rogier M Determann MD PhD, Jonathan
 1 LUNG PROTECTIVE VENTILATION WITH LOW TIDAL VOLUMES AND THE OCCURRENCE OF PULMONARY COMPLICATIONS IN PATIENTS WITHOUT ARDS: a systematic review and individual patient data metaanalysis SUPPLEMENTARY APPENDIX
1 LUNG PROTECTIVE VENTILATION WITH LOW TIDAL VOLUMES AND THE OCCURRENCE OF PULMONARY COMPLICATIONS IN PATIENTS WITHOUT ARDS: a systematic review and individual patient data metaanalysis SUPPLEMENTARY APPENDIX
Principles of Mechanical Ventilation: A Graphics-Based Approach
 Principles of Mechanical Ventilation: A Graphics-Based Approach Steven M. Donn, MD, FAAP Professor of Pediatrics Neonatal-Perinatal Medicine C.S. Mott Children s Hospital University of Michigan Health
Principles of Mechanical Ventilation: A Graphics-Based Approach Steven M. Donn, MD, FAAP Professor of Pediatrics Neonatal-Perinatal Medicine C.S. Mott Children s Hospital University of Michigan Health
OPEN LUNG APPROACH CONCEPT OF MECHANICAL VENTILATION
 OPEN LUNG APPROACH CONCEPT OF MECHANICAL VENTILATION L. Rudo Mathivha Intensive Care Unit Chris Hani Baragwanath Aacademic Hospital & the University of the Witwatersrand OUTLINE Introduction Goals & Indications
OPEN LUNG APPROACH CONCEPT OF MECHANICAL VENTILATION L. Rudo Mathivha Intensive Care Unit Chris Hani Baragwanath Aacademic Hospital & the University of the Witwatersrand OUTLINE Introduction Goals & Indications
Mechanical power and the development of Ventilator-Induced Lung
 Supplemental Digital Content 1 Mechanical power and the development of Ventilator-Induced Lung Injury Massimo Cressoni, Miriam Gotti, Chiara Chiurazzi, Dario Massari, Ilaria Algieri, Martina Amini, Antonio
Supplemental Digital Content 1 Mechanical power and the development of Ventilator-Induced Lung Injury Massimo Cressoni, Miriam Gotti, Chiara Chiurazzi, Dario Massari, Ilaria Algieri, Martina Amini, Antonio
EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES
 GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
Stratégie ventilatoire pendant la RCP Pr Jean-Christophe M Richard
 Stratégie ventilatoire pendant la RCP Pr Jean-Christophe M Richard Pôle SAMU 74 Urgence et Réanimation Centre Hospitalier Annecy Genevois CONFLICTS OF INTEREST - Air Liquide Medical Systems (part time)
Stratégie ventilatoire pendant la RCP Pr Jean-Christophe M Richard Pôle SAMU 74 Urgence et Réanimation Centre Hospitalier Annecy Genevois CONFLICTS OF INTEREST - Air Liquide Medical Systems (part time)
Respiratory Physiology Gaseous Exchange
 Respiratory Physiology Gaseous Exchange Session Objectives. What you will cover Basic anatomy of the lung including airways Breathing movements Lung volumes and capacities Compliance and Resistance in
Respiratory Physiology Gaseous Exchange Session Objectives. What you will cover Basic anatomy of the lung including airways Breathing movements Lung volumes and capacities Compliance and Resistance in
How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital. Synopsis
 How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital Synopsis Definition of an oscillator Historical perspective Differences between HFOV and CMV Determinants
How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital Synopsis Definition of an oscillator Historical perspective Differences between HFOV and CMV Determinants
 C CONFERENCIAS MAGISTRALES Vol. 34. Supl. 1 Abril-Junio 211 pp S293-S31 Perioperative ventilator management: Why it makes a difference Daniel R. Brown, PhD, MD, FCCM Chair, Division of Critical Care Medicine.
C CONFERENCIAS MAGISTRALES Vol. 34. Supl. 1 Abril-Junio 211 pp S293-S31 Perioperative ventilator management: Why it makes a difference Daniel R. Brown, PhD, MD, FCCM Chair, Division of Critical Care Medicine.
Using Common Ventilator Graphics to Provide Optimal Ventilation
 Using Common Ventilator Graphics to Provide Optimal Ventilation David Vines, MHS, RRT, FAARC Associate Professor Chair / Program Director Department of Respiratory Care RUSH UNIVERSITY MEDICAL CENTER Disclosure
Using Common Ventilator Graphics to Provide Optimal Ventilation David Vines, MHS, RRT, FAARC Associate Professor Chair / Program Director Department of Respiratory Care RUSH UNIVERSITY MEDICAL CENTER Disclosure
mechanical ventilation Arjun Srinivasan
 Respiratory mechanics in mechanical ventilation Arjun Srinivasan Introduction Mechanics during ventilation PV curves Application in health & disease Difficulties & pitfalls The future. Monitoring Mechanics
Respiratory mechanics in mechanical ventilation Arjun Srinivasan Introduction Mechanics during ventilation PV curves Application in health & disease Difficulties & pitfalls The future. Monitoring Mechanics
Neonatal Assisted Ventilation. Haresh Modi, M.D. Aspirus Wausau Hospital, Wausau, WI.
 Neonatal Assisted Ventilation Haresh Modi, M.D. Aspirus Wausau Hospital, Wausau, WI. History of Assisted Ventilation Negative pressure : Spirophore developed in 1876 with manual device to create negative
Neonatal Assisted Ventilation Haresh Modi, M.D. Aspirus Wausau Hospital, Wausau, WI. History of Assisted Ventilation Negative pressure : Spirophore developed in 1876 with manual device to create negative
The comparison of Work Of Breathing methodologies on a patient model
 The comparison of Work Of Breathing methodologies on a patient model E. Koumoundouros 1, J. Santamaria 2 and J. Patterson 3. 1 Department of Electrical and Electronic Engineering, The University of Melbourne,
The comparison of Work Of Breathing methodologies on a patient model E. Koumoundouros 1, J. Santamaria 2 and J. Patterson 3. 1 Department of Electrical and Electronic Engineering, The University of Melbourne,
Limits of normality of quantitative thoracic CT analysis
 RESEARCH Open Access Limits of normality of quantitative thoracic CT analysis Massimo Cressoni 1*, Elisabetta Gallazzi 1, Chiara Chiurazzi 1, Antonella Marino 1, Matteo Brioni 1, Federica Menga 1, Irene
RESEARCH Open Access Limits of normality of quantitative thoracic CT analysis Massimo Cressoni 1*, Elisabetta Gallazzi 1, Chiara Chiurazzi 1, Antonella Marino 1, Matteo Brioni 1, Federica Menga 1, Irene
Nitrogen washout/washin, helium dilution and computed tomography in the assessment of End Expiratory Lung Volume
 Critical Care This Provisional PDF corresponds to the article as it appeared upon acceptance. Copyedited and fully formatted PDF and full text (HTML) versions will be made available soon. Nitrogen washout/washin,
Critical Care This Provisional PDF corresponds to the article as it appeared upon acceptance. Copyedited and fully formatted PDF and full text (HTML) versions will be made available soon. Nitrogen washout/washin,
Neonatal tidal volume targeted ventilation
 Neonatal tidal volume targeted ventilation Colin Morley Retired Professor of Neonatal Medicine, Royal Women s Hospital, Melbourne, Australia. Honorary Visiting Fellow, Dept Obstetrics and Gynaecology,
Neonatal tidal volume targeted ventilation Colin Morley Retired Professor of Neonatal Medicine, Royal Women s Hospital, Melbourne, Australia. Honorary Visiting Fellow, Dept Obstetrics and Gynaecology,
Lung Volumes and Ventilation
 Respiratory System ssrisuma@rics.bwh.harvard.edu Lung Volumes and Ventilation Minute ventilation Volume of an inspired or expired air per minute = tidal volume (V T ) x respiratory rate Dead space ventilation
Respiratory System ssrisuma@rics.bwh.harvard.edu Lung Volumes and Ventilation Minute ventilation Volume of an inspired or expired air per minute = tidal volume (V T ) x respiratory rate Dead space ventilation
Mechanical Ventilation and Optimisation through Analytical Lung Model
 Mechanical Ventilation and Optimisation through Analytical Lung Model Ankit Mishra A thesis presented for the degree of Masters of Engineering in Mechanical Engineering at the University of Canterbury,
Mechanical Ventilation and Optimisation through Analytical Lung Model Ankit Mishra A thesis presented for the degree of Masters of Engineering in Mechanical Engineering at the University of Canterbury,
Mechanical Ventilation. Which of the following is true regarding ventilation? Basics of Ventilation
 Mechanical Ventilation Jeffrey L. Wilt, MD, FACP, FCCP Associate Professor of Medicine Michigan State University Associate Program Director MSU-Grand Rapids Internal Medicine Residency Which of the following
Mechanical Ventilation Jeffrey L. Wilt, MD, FACP, FCCP Associate Professor of Medicine Michigan State University Associate Program Director MSU-Grand Rapids Internal Medicine Residency Which of the following
Mechanical Ventilation. Mechanical Ventilation is a Drug!!! is a drug. MV: Indications for use. MV as a Drug: Outline. MV: Indications for use
 Mechanical Ventilation is a Drug!!! Mechanical Ventilation is a drug I am an employee of Philips Healthcare Hospital Respiratory Care Group and they help me pay for my kids education Jim Laging, RRT, RCP
Mechanical Ventilation is a Drug!!! Mechanical Ventilation is a drug I am an employee of Philips Healthcare Hospital Respiratory Care Group and they help me pay for my kids education Jim Laging, RRT, RCP
Simplicity and Safety Prevention Efficiency and Biocompatibility
 Simplicity and Safety Prevention Efficiency and Biocompatibility Bibliography 1. Gattinoni L, Kolobow T, Damia G, Agostani A, Pesenti A: Extracorporeal carbon dioxide removal (ECCO2R): a new form of respiratory
Simplicity and Safety Prevention Efficiency and Biocompatibility Bibliography 1. Gattinoni L, Kolobow T, Damia G, Agostani A, Pesenti A: Extracorporeal carbon dioxide removal (ECCO2R): a new form of respiratory
Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams)
") Name Lab Partners Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams) Part 1. Lung Volumes and Capacities Objectives 1. Obtain graphical representation of lung capacities
Name Lab Partners Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams) Part 1. Lung Volumes and Capacities Objectives 1. Obtain graphical representation of lung capacities
Physiological based management of hypoxaemic respiratory failure
 Physiological based management of hypoxaemic respiratory failure David Tingay 1. Neonatal Research, Murdoch Children s Research Institute, Melbourne 2. Neonatology, Royal Children s Hospital 3. Dept of
Physiological based management of hypoxaemic respiratory failure David Tingay 1. Neonatal Research, Murdoch Children s Research Institute, Melbourne 2. Neonatology, Royal Children s Hospital 3. Dept of
Chapter 3: Invasive mechanical ventilation Stephen Lo
 Chapter 3: Invasive mechanical ventilation Stephen Lo Introduction Conventional mechanical ventilation is the delivery of positive pressure to the airway to allow removal of CO2 and delivery of O2. In
Chapter 3: Invasive mechanical ventilation Stephen Lo Introduction Conventional mechanical ventilation is the delivery of positive pressure to the airway to allow removal of CO2 and delivery of O2. In
WHAT IS SAFE VENTILATION? Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine
 WHAT IS SAFE VENTILATION? Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine holets.steven@mayo.edu DISCLOSURES Past and present Advisory Boards: Resmed Philips/Respironics
WHAT IS SAFE VENTILATION? Steven Holets RRT Assistant Professor of Anesthesiology Mayo Clinic College of Medicine holets.steven@mayo.edu DISCLOSURES Past and present Advisory Boards: Resmed Philips/Respironics
Flight Medical presents the F60
 Flight Medical presents the F60 Reliable Ventilation Across the Spectrum of Care Adult & Pediatric Pressure/Volume Control Basic/Advanced Modes Invasive/NIV High Pressure/Low Flow O2 Up to 12 hours batteries
Flight Medical presents the F60 Reliable Ventilation Across the Spectrum of Care Adult & Pediatric Pressure/Volume Control Basic/Advanced Modes Invasive/NIV High Pressure/Low Flow O2 Up to 12 hours batteries
 http://www.priory.com/cmol/hfov.htm INTRODUCTION The vast majority of patients who are admitted to an Intensive Care Unit (ICU) will need artificial ventilation (Jones et al 1998). The usual means through
http://www.priory.com/cmol/hfov.htm INTRODUCTION The vast majority of patients who are admitted to an Intensive Care Unit (ICU) will need artificial ventilation (Jones et al 1998). The usual means through
Acute Respiratory Distress Syndrome. Marty Black MD Concord Pulmonary Medicine 5/4/2018
 Acute Respiratory Distress Syndrome Marty Black MD Concord Pulmonary Medicine 5/4/2018 Financial: none Disclosures Objectives: Identify clinical features of ARDS Identify physiology and therapeutic benefit
Acute Respiratory Distress Syndrome Marty Black MD Concord Pulmonary Medicine 5/4/2018 Financial: none Disclosures Objectives: Identify clinical features of ARDS Identify physiology and therapeutic benefit
What can we learn from high-frequency ventilation?
 What can we learn from high-frequency ventilation? Dipartimento di Medicina Perioperatoria, Terapia Intensiva ed Emergenza Azienda Sanitaria Universitaria Integrata di Trieste Università degli Studi di
What can we learn from high-frequency ventilation? Dipartimento di Medicina Perioperatoria, Terapia Intensiva ed Emergenza Azienda Sanitaria Universitaria Integrata di Trieste Università degli Studi di
For more information about how to cite these materials visit
 Author(s): Louis D Alecy, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Louis D Alecy, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Online Data Supplement
 REVERSIBILITY OF LUNG COLLAPSE AND HYPOXEMIA IN EARLY ACUTE RESPIRATORY DISTRESS SYNDROME AUTHORS: BORGES, JOÃO B. MD OKAMOTO, VALDELIS N. MD MATOS, GUSTAVO F. J. MD CARAMEZ, MARIA P. R. MD ARANTES, PAULA
REVERSIBILITY OF LUNG COLLAPSE AND HYPOXEMIA IN EARLY ACUTE RESPIRATORY DISTRESS SYNDROME AUTHORS: BORGES, JOÃO B. MD OKAMOTO, VALDELIS N. MD MATOS, GUSTAVO F. J. MD CARAMEZ, MARIA P. R. MD ARANTES, PAULA
HFOV in the PICU and NICU setting
 in the PICU and NICU setting Courtesy from G. Niemann Peter C. Rimensberger, MD Associate Professor Pediatric and Neonatal Intensive Care University Hospital of Geneva Allowable V t depends on pathology
in the PICU and NICU setting Courtesy from G. Niemann Peter C. Rimensberger, MD Associate Professor Pediatric and Neonatal Intensive Care University Hospital of Geneva Allowable V t depends on pathology
Respiratory system & exercise. Dr. Rehab F Gwada
 Respiratory system & exercise Dr. Rehab F Gwada Objectives of lecture Outline the major anatomical components & important functions of the respiratory system. Describe the mechanics of ventilation. List
Respiratory system & exercise Dr. Rehab F Gwada Objectives of lecture Outline the major anatomical components & important functions of the respiratory system. Describe the mechanics of ventilation. List
April KHALED MOUSA BACHA. Physiology #2. Dr. Nayef AL-Gharaibeh. Pulmonary volumes & capacities
 25 th April Physiology #2 Pulmonary volumes & capacities Dr. Nayef AL-Gharaibeh KHALED MOUSA BACHA We will start this lecture by explaining an important concept from the previous one: Intrapleural pressure
25 th April Physiology #2 Pulmonary volumes & capacities Dr. Nayef AL-Gharaibeh KHALED MOUSA BACHA We will start this lecture by explaining an important concept from the previous one: Intrapleural pressure
4/18/12 MECHANISM OF RESPIRATION. Every Breath You Take. Fun Facts
 Objectives MECHANISM OF RESPIRATION Dr Badri Paudel Explain how the intrapulmonary and intrapleural pressures vary during ventilation and relate these pressure changes to Boyle s law. Define the terms
Objectives MECHANISM OF RESPIRATION Dr Badri Paudel Explain how the intrapulmonary and intrapleural pressures vary during ventilation and relate these pressure changes to Boyle s law. Define the terms
Mechanical Ventilation 2016
 Conflict of Interest Disclosure Robert M Kacmarek Lung Protective Ventilation: New Information RT s Neec to Know 5-6-17 FOCUS Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital
Conflict of Interest Disclosure Robert M Kacmarek Lung Protective Ventilation: New Information RT s Neec to Know 5-6-17 FOCUS Bob Kacmarek PhD, RRT Harvard Medical School Massachusetts General Hospital
Image-Based Measurement of Alveoli Volume Expansion in an Animal Model of a Diseased Lung
 Image-Based Measurement of Alveoli Volume Expansion in an Animal Model of a Diseased Lung C. E. Hann 1, D. Hewett 1, J. G. Chase 1, T. Rabczuk 1, A. Sundaresan 1, X. Chen 1, W. Wang 1 and G. M. Shaw 2
Image-Based Measurement of Alveoli Volume Expansion in an Animal Model of a Diseased Lung C. E. Hann 1, D. Hewett 1, J. G. Chase 1, T. Rabczuk 1, A. Sundaresan 1, X. Chen 1, W. Wang 1 and G. M. Shaw 2
3100A Competency Exam
 NAME DATE (Circle the appropriate answer) 3100A Competency Exam 1. Of the following, which best describes the mechanics of ventilation used by the 3100A? a. Active inspiration with passive exhalation b.
NAME DATE (Circle the appropriate answer) 3100A Competency Exam 1. Of the following, which best describes the mechanics of ventilation used by the 3100A? a. Active inspiration with passive exhalation b.
LUNG CLEARANCE INDEX. COR-MAN IN Issue A, Rev INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark
 LUNG CLEARANCE INDEX METHOD COR-MAN-0000-008-IN Issue A, Rev. 3 2013-07-01 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
LUNG CLEARANCE INDEX METHOD COR-MAN-0000-008-IN Issue A, Rev. 3 2013-07-01 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
Alveolar Recruiment for ARDS Trial
 Alveolar Recruiment for ARDS Trial Alexandre Biasi Cavalcanti HCor Research Institute For the ART Investigators Trial Organization Coordination: HCor Research Institute (Sao Paulo, Brazil). Support: Brazilian
Alveolar Recruiment for ARDS Trial Alexandre Biasi Cavalcanti HCor Research Institute For the ART Investigators Trial Organization Coordination: HCor Research Institute (Sao Paulo, Brazil). Support: Brazilian
Activity 2: Examining the Effect of Changing Airway Resistance on Respiratory Volumes
 1 BGYC34 PhysioEx Lab 7 Respiratory Systems Mechanics Marking Scheme Part 1 Complete PhysioEx lab #7. Hand-in all of the pages associated with the lab. Note that there are 5 activities to be completed.
1 BGYC34 PhysioEx Lab 7 Respiratory Systems Mechanics Marking Scheme Part 1 Complete PhysioEx lab #7. Hand-in all of the pages associated with the lab. Note that there are 5 activities to be completed.
RESPIRATORY REGULATION DURING EXERCISE
 RESPIRATORY REGULATION DURING EXERCISE Respiration Respiration delivery of oxygen to and removal of carbon dioxide from the tissue External respiration ventilation and exchange of gases in the lung Internal
RESPIRATORY REGULATION DURING EXERCISE Respiration Respiration delivery of oxygen to and removal of carbon dioxide from the tissue External respiration ventilation and exchange of gases in the lung Internal
MEDICAL EQUIPMENT IV MECHANICAL VENTILATORS. Prof. Yasser Mostafa Kadah
 MEDICAL EQUIPMENT IV - 2013 MECHANICAL VENTILATORS Prof. Yasser Mostafa Kadah Mechanical Ventilator A ventilator is a machine, a system of related elements designed to alter, transmit, and direct energy
MEDICAL EQUIPMENT IV - 2013 MECHANICAL VENTILATORS Prof. Yasser Mostafa Kadah Mechanical Ventilator A ventilator is a machine, a system of related elements designed to alter, transmit, and direct energy
RESPIRATORY PHYSIOLOGY. Anaesthesiology Block 18 (GNK 586) Prof Pierre Fourie
 Prof Pierre Fourie") RESPIRATORY PHYSIOLOGY Anaesthesiology Block 18 (GNK 586) Prof Pierre Fourie Outline Ventilation Diffusion Perfusion Ventilation-Perfusion relationship Work of breathing Control of Ventilation 2 This image
RESPIRATORY PHYSIOLOGY Anaesthesiology Block 18 (GNK 586) Prof Pierre Fourie Outline Ventilation Diffusion Perfusion Ventilation-Perfusion relationship Work of breathing Control of Ventilation 2 This image
The Respiratory System Part I. Dr. Adelina Vlad
 The Respiratory System Part I Dr. Adelina Vlad The Respiratory Process Breathing automatic, rhythmic and centrally-regulated mechanical process by which the atmospheric gas moves into and out of the lungs
The Respiratory System Part I Dr. Adelina Vlad The Respiratory Process Breathing automatic, rhythmic and centrally-regulated mechanical process by which the atmospheric gas moves into and out of the lungs
ONLINE SUPPLEMENT 6. EIT definitions and nomenclature
 Chest electrical tomography examination, data analysis, terminology, clinical use and recommendations: consensus statement of the TRanslational EIT development study group Inéz Frerichs, Marcelo B. P.
Chest electrical tomography examination, data analysis, terminology, clinical use and recommendations: consensus statement of the TRanslational EIT development study group Inéz Frerichs, Marcelo B. P.
CHAPTER 3: The cardio-respiratory system
 : The cardio-respiratory system Exam style questions - text book pages 44-45 1) Describe the structures involved in gaseous exchange in the lungs and explain how gaseous exchange occurs within this tissue.
: The cardio-respiratory system Exam style questions - text book pages 44-45 1) Describe the structures involved in gaseous exchange in the lungs and explain how gaseous exchange occurs within this tissue.
Recruitment and Derecruitment during Acute Respiratory Failure A Clinical Study
 Recruitment and Derecruitment during Acute Respiratory Failure A Clinical Study STEFANIA CROTTI, DANIELE MASCHERONI, PIETRO CAIRONI, PAOLO PELOSI, GIULIO RONZONI, MICHELE MONDINO, JOHN J. MARINI, and LUCIANO
Recruitment and Derecruitment during Acute Respiratory Failure A Clinical Study STEFANIA CROTTI, DANIELE MASCHERONI, PIETRO CAIRONI, PAOLO PELOSI, GIULIO RONZONI, MICHELE MONDINO, JOHN J. MARINI, and LUCIANO
Ventilators. Dr Simon Walton Consultant Anaesthetist Eastbourne DGH KSS Basic Science Course
 Ventilators Dr Simon Walton Consultant Anaesthetist Eastbourne DGH KSS Basic Science Course Objectives Discuss Classification/ terminology Look at Modes of ventilation How some specific ventilators work
Ventilators Dr Simon Walton Consultant Anaesthetist Eastbourne DGH KSS Basic Science Course Objectives Discuss Classification/ terminology Look at Modes of ventilation How some specific ventilators work
Respiratory System. Prepared by: Dorota Marczuk-Krynicka, MD, PhD
 Respiratory System Prepared by: Dorota Marczuk-Krynicka, MD, PhD Lungs: Ventilation Perfusion Gas Exchange - Diffusion 1. Airways and Airway Resistance (AWR) 2. Mechanics of Breathing and Lung (Elastic)
Respiratory System Prepared by: Dorota Marczuk-Krynicka, MD, PhD Lungs: Ventilation Perfusion Gas Exchange - Diffusion 1. Airways and Airway Resistance (AWR) 2. Mechanics of Breathing and Lung (Elastic)
Volume Diffusion Respiration (VDR)
") Volume Diffusion Respiration (VDR) A therapy with many uses Jeffrey Pietz, MD April 15, 2016 VDR ventilation has been used to treat patients with: ARDS Meconium Aspiration Burn and Inhalation Injury RDS
Volume Diffusion Respiration (VDR) A therapy with many uses Jeffrey Pietz, MD April 15, 2016 VDR ventilation has been used to treat patients with: ARDS Meconium Aspiration Burn and Inhalation Injury RDS
Chapter 4: Ventilation Test Bank MULTIPLE CHOICE
 Instant download and all chapters Test Bank Respiratory Care Anatomy and Physiology Foundations for Clinical Practice 3rd Edition Will Beachey https://testbanklab.com/download/test-bank-respiratory-care-anatomy-physiologyfoundations-clinical-practice-3rd-edition-will-beachey/
Instant download and all chapters Test Bank Respiratory Care Anatomy and Physiology Foundations for Clinical Practice 3rd Edition Will Beachey https://testbanklab.com/download/test-bank-respiratory-care-anatomy-physiologyfoundations-clinical-practice-3rd-edition-will-beachey/