11/30/2015. Tactical Combat Casualty Care and SOF Tactical Trauma Protocols PFN: SOMTCL03. Terminal Learning Objective. Reason. Hours: 2.
|
|
|
- Daniela Todd
- 5 years ago
- Views:
Transcription
 and SOF Tactical Trauma Protocols (TTPs) Condition: Given a lecture in a")
1 Tactical Combat Casualty Care and SOF Tactical Trauma Protocols PFN: SOMTCL03 Hours: 2.5 Instructor: Slide 1 Terminal Learning Objective Action: Communicate knowledge of Tactical Combat Casualty Care (TCCC) and SOF Tactical Trauma Protocols (TTPs) Condition: Given a lecture in a classroom environment Standard: Received a minimum score of 75% on the written exam and a GO on the practical exam IAW course standards Slide 2 Reason Slide 3 1

2 Agenda Outline the origins, history, and objectives of TCCC and SOF TTPs Identify the three phases of TCCC and SOF TTPs Identify the Care Under Fire treatment priorities Identify the treatment priorities Slide 4 Agenda Identify the SOF TTPs extended Tactical Field Care considerations Identify the Tactical Evacuation Care treatment priorities Slide 5 Origins, History, and Objectives of TCCC and SOF TTPs Slide 6 2
 Slide 7 USSOCOM Directive All SOF deploying personnel Trained on current TCCC guidelines")
3 Origins, History, and Objectives of TCCC and SOF TTPs Navy initiated TCCC project in 1993 Original guidelines published in 1996 (Journal of Military Medicine) First TCCC course taught in 1996 TCCC incorporated in PHTLS manual 1999 ACSCOT and NAEMT endorsement CoTCCC established in 2001 (meets quarterly) Slide 7 USSOCOM Directive All SOF deploying personnel Trained on current TCCC guidelines ml _curriculum Training completed within 6 months prior to deployment in support of combat operations Slide 8 Origins, History, and Objectives of TCCC and SOF TTPs 90% of combat casualties that die, die before reaching a MTF Slide 9 3

4 Origins, History, and Objectives of TCCC and SOF TTPs Slide 10 Origins, History, and Objectives of TCCC and SOF TTPs Slide 11 Origins, History, and Objectives of TCCC and SOF TTPs Slide 12 4

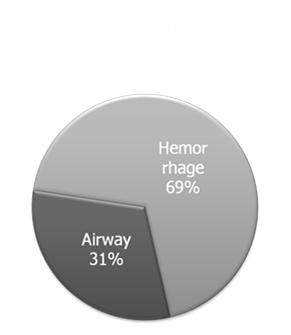
5 Origins, History, and Objectives of TCCC and SOF TTPs Top three preventable deaths on the battlefield: Hemorrhage from extremity wounds Airway compromise from maxillofacial trauma Tension pneumothorax Slide 13 Origins, History, and Objectives of TCCC and SOF TTPs TCCC objectives Treat the casualty Prevent additional casualties Complete the mission TTP additional options Extended field care Slide 14 Three Phases of TCCC and SOF TTPs Slide 15 5

6 Three Phases of TCCC and SOF TTPs Care Under Fire (CUF) (TFC) Extended Considerations Tactical Evacuation Care (TEC) Slide 16 Care Under Fire Treatment Priorities Slide 17 Care Under Fire Return fire and take cover Direct or expect casualty to remain engaged as a combatant if appropriate Direct casualty to move to cover and apply self aid if able Try to keep casualty from sustaining additional wounds Slide 18 6

7 Care Under Fire Casualties should be extricated from burning vehicles or buildings and moved to places of relative safety Do what is necessary to stop the burning process Airway management is best deferred until phase Slide 19 Care Under Fire Stop any life threatening external hemorrhage if tactically feasible Direct casualty to control hemorrhage by self aid if able Use a CoTCCC recommended limb tourniquet for hemorrhage that is anatomically amenable to tourniquet use Apply the limb tourniquet over the uniform clearly proximal to the bleeding site If the bleeding site is not apparent place the tourniquet as proximal as possible Slide 20 Treatment Priorities Slide 21 7
8 Casualties with an altered mental status should be disarmed immediately Airway management Unconscious without airway obstruction Chin lift or jaw thrust maneuver Nasopharyngeal airway Place casualty in recovery position Slide 22 Airway management (cont.) Casualty with/or impending airway obstruction Chin Lift or Jaw Thrust maneuver Nasopharyngeal airway Allow casualty to assume any position that best protects the airway, including sitting up Place unconscious casualty in recovery position Protect spine in blunt and blast trauma patients If measures above are unsuccessful: supraglottic airway, intubation or surgical cricothyroidotomy (CricKey, Bougie aided or standard open surgical) Slide 23 Breathing Consider tension pneumothorax and decompress with 14G 3.25 needle/catheter unit if casualty has known or suspected torso trauma and progressive respiratory distress 2 nd ICS, MCL primary 4 th or 5 th anterior axillary line is the alternate Lateral to nipple line and not directed to heart Remove the needle and leave catheter in place Slide 24 8
9 Breathing (cont.) Repeat decompression as required Consider decompression of opposite side if casualty doesn t improve Consider chest tube for ineffective NDC Treat open chest wounds with a vented chest seal (if unavailable use a non vented seal) Monitor the casualty for development of a subsequent tension pneumothorax Slide 25 Bleeding Assess for unrecognized hemorrhage and control all sources of bleeding Use combat gauze for compressible hemorrhage not amenable to tourniquet use Consider a CoTCCC Junctional tourniquet for lower extremity or groin/inguinal wound not amenable to tourniquet use and cannot be controlled with hemostatic dressings Slide 26 Bleeding (cont.) Reassess prior tourniquet application; expose wound and determine is needed If so, place limb tourniquet directly to skin 2 3 above wound If not needed, use other methods to control bleeding Check distal pulse as situation permits If distal pulse is still present consider additional tightening of tourniquet or use of second tourniquet Slide 27 9
10 Bleeding (cont.) Expose and mark all tourniquet sites with time of application using an indelible marker Limb tourniquets and junctional tourniquets should be converted as soon as possible if three criteria are met: casualty is not in shock, wound can be monitored for bleeding, tourniquet is not on an amputation Apply pelvic binder for suspected pelvic fracture Slide 28 Prevention of hypothermia Minimize casualty s exposure to elements; keep protective gear on or with the casualty Replace wet clothing with dry Get the casualty onto an insulated surface (litter) Apply the Ready Heat Blanket on torso (not directly on skin); wrap in HRS or Blizzard Rescue blanket Slide 29 Prevention of hypothermia (cont.) If mentioned gear is not available, use dry blankets, poncho liners, sleeping bags, body bags, or anything that will retain heat and keep the casualty dry Slide 30 10
11 Intravenous (IV) access Start an 18 gauge IV or saline lock if indicated If resuscitation is required and IV access is not obtainable, use the intraosseous (IO) route Slide 31 Tranexamic Acid (TXA) If a casualty is anticipated to need significant blood transfusion Administer 1 gram of Tranexamic Acid in 100 ml Normal Saline or Lactated Ringers over 10 minutes as soon as possible but NOT later than 3 hours after injury Not in same line as Hextend or blood products Begin second infusion of 1 gm TXA after Hextend or other fluid treatment Mark casualty with amount of TXA given on chest Slide 32 Fluid resuscitation (cont.) Assess for hemorrhagic shock Altered mental status in the absence of head injury and/or weak or absent peripheral pulses Systolic blood pressure less than 80 mmhg Not in hemorrhagic shock No IV fluids are immediately necessary Fluids by mouth are permissible Slide 33 11
12 Fluid resuscitation (cont.) In hemorrhagic shock and blood products are available Whole blood Plasma, RBCs and platelets 1:1:1 Plasma and RBCs 1:1 Plasma or RBCs alone Reassess after each unit and continue until a palpable radial pulse, improved mental status or systolic BP between mmhg Slide 34 Fluid resuscitation (cont.) In hemorrhagic shock and blood products are NOT available Hextend Lactated Ringers or Plasma Lyte A Reassess after each 500 ml bolus and continue until a palpable radial pulse, improved mental status or systolic BP between mmhg Slide 35 Fluid resuscitation (cont.) Altered LOC with suspected TBI should be resuscitated to 90 mmhg systolic BP If shock recurs, reassess all external hemorrhage and repeat fluid resuscitation Continued efforts must be weighed against logistical and tactical considerations and the risk of incurring further casualties Warm fluids if possible to prevent hypothermia Slide 36 12
13 Head injury management Fluid resuscitate hypotension Maintain spo2 > 90%; goal = 95% Controlled mild hyperventilation (20 BPM) Hypertonic saline (3 5%) 250ml bolus Seizure prophylaxis Cerebyx 18 mg/kg IV/IO at mg/min Seizure management Valium 5 10 mg IV/IO q 5 minutes Versed 5 mg IV/IO q 5 minutes Slide 37 Head injury management (cont.) Patient positioning If CSF present elevate degrees If IICP only elevate 30 degrees Don t elevate the head of a hypovolemic casualty Sedation of severe TBI after airway established Versed 1 2 mg/hour IV/IO TCCC/SOF TTPs antibiotic prophylaxis should be started Slide 38 Abdominal evisceration Control visible hemorrhage Irrigate and gently reduce if possible Cover and keep warm Penetrating eye trauma Perform a rapid field test of visual acuity Cover the eye with rigid eye shield (not pressure patch) Start antibiotics Slide 39 13
14 Burns Facial burns, especially those that occur in closed spaces, may be associated with inhalation injury Aggressively monitor airway status and oxygen saturation in such patients and consider early surgical airway for respiratory distress or oxygen desaturation Slide 40 Burns (cont.) Estimate total body surface area (TBSA) burned to the nearest 10% using the Rule of Nines Cover the burn area with dry, sterile dressings For extensive burns (> 20%), consider placing the casualty in the Blizzard Survival Blanket in the Hypothermia Prevention Kit in order to both cover the burned areas and prevent hypothermia Slide 41 Burns (cont.) Fluid resuscitation (USAISR Rule of Ten) If burns are greater than 20% of Total Body Surface Area, fluid resuscitation should be initiated as soon as IV/IO access is established Resuscitation should be initiated with Lactated Ringer s, Normal Saline, or Hextend If Hextend is used, no more than 1000 ml should be given, followed by Lactated Ringer s or Normal Saline as needed Slide 42 14
15 Burns (cont.) Fluid resuscitation (USAISR Rule of Ten) Initial IV/IO fluid rate is calculated as %TBSA x 10 ml/hr for adults weighing kg For every 10 kg ABOVE 80 kg, increase initial rate by 100 ml/hr If hemorrhagic shock is also present, resuscitation for hemorrhagic shock takes precedence over resuscitation for burn shock Administer IV/IO fluids per the TCCC Guidelines Slide 43 Burns (cont.) Analgesia in accordance with the TCCC guidelines may be administered to treat burn pain Prehospital antibiotic therapy is not indicated solely for burns, but antibiotics should be given per the TCCC guidelines if indicated to prevent infection in penetrating wounds All TCCC interventions can be performed on or through burned skin in a burn casualty Slide 44 Inspect and dress known wounds Check for additional wounds Splint fractures and recheck pulses Basic splinting fundamentals apply Crush injury management Immediately ml NS Just before extrication apply tourniquets and give sodium bicarbonate After extrication monitor for cardiac arrest Slide 45 15
16 Monitoring Pulse oximetry should be available as an adjunct to clinical monitoring Readings may be misleading in the settings of shock or marked hypothermia Slide 46 Analgesia if able to fight Meloxicam (Mobic) 15 mg PO once a day Acetaminophen 650 mg bilayer caplet, 2 PO every 8 hours Slide 47 Analgesia if unable to fight without IV/IO Hypovolemic shock or respiratory distress Ketamine (Ketalar) 50 mg IM or IN Repeat dose every min Controls pain or nystagmus occurs No hypovolemic shock or respiratory distress Fentanyl Citrate (OTFC) 800 ug transbuccally Reassess in 15 minutes Monitor for respiratory depression Slide 48 16
17 Analgesia if unable to fight with IV/IO Hypovolemic shock or respiratory distress Ketamine 20 mg IV/IO over 1 minute repeat dose every 5 10 min to control pain or until nystagmus occurs (max of 100mg/hr) Consider Versed 1 mg IV for agitation No hypovolemic shock or respiratory distress Morphine 5 10 mg IV/IO repeat dose every 10 minutes as necessary (monitor for respiratory depression) Slide 49 Consider an antiemetic for opioid or trauma induced nausea or vomiting Ondansetron (Zofran) 4 mg ODT/IV/IO/IM every 8 hours Can be repeated once at 15 min Max 8mg in any 8 hour period Promethazine (Phenergan) Must be diluted and given slowly Has a synergistic effect Use only if Zofran is not available Slide 50 Antibiotics: recommended for all open combat wounds Able to take PO Moxifloxacin 400 mg PO one a day Unable to take PO Ertapenem 1 g IV/IM once a day Cefotetan 2g IV (slow push over 3 5 minutes) or IM every 12 hours Slide 51 17

18 Communicate with patient if possible Encourage and reassure Explain care Cardiopulmonary resuscitation Resuscitation on the battlefield for victims of blast or penetrating trauma who have no pulse, no respirations, and no other signs of life will not be successful and should not be attempted Slide 52 Bilateral needle decompression For casualties with torso or multisystem trauma and no pulse or respirations during TFC phase Document Clinical assessments, treatments rendered, and changes in casualty s status on a TCCC Casualty Card Forward this Information with the casualty to the next level of care Slide 53 SOF TTPs Extended Tactical Field Care Considerations Slide 54 18
19 SOF TTPs Extended Tactical Field Care Considerations Airway Suction Consider periodic suctioning of the oropharynx and endotracheal tube Pulmonary toilet Consider periodic saline flushes (2 ml) to clear mucus/blood from ET tube Local wound care at cricothyroidotomy site if applicable Slide 55 SOF TTPs Extended Tactical Field Care Considerations Respiratory management Perform chest tube and apply chest drain Consider rib blocks for pain management Administer oxygen if available Consider the use of a ventilator/assist device if available Consider sedation with midazolam (Versed) 1 2 mg/hour IV/IO for prolonged intubation Slide 56 SOF TTPs Extended Tactical Field Care Considerations Flail chest management Monitor for developing hypoxia secondary to pulmonary contusions Casualty may require positive pressure ventilation Ensure adequate analgesia Consider rib blocks for pain management These casualties frequently fatigue and require intubation/definitive surgical airway Slide 57 19
20 SOF TTPs Extended Tactical Field Care Considerations Fluid management Conscious Instruct casualty to drink clear liquids up to 1 liter per hour; consider oral electrolyte supplementation if available Unconscious Insert Foley catheter and titrate IV/IO/NG/PR crystalloid fluids to maintain urine output of ml per hour Clean water may be utilized in lieu of crystalloid for NG/PR infusion Slide 58 SOF TTPs Extended Tactical Field Care Considerations Fluid management (cont.) Critical burn (> 20% TBSA of 2 nd /3 rd degree burns) Continue fluid resuscitation according to The Rule of Ten Insert Foley catheter and adjust fluid rate to maintain urine output of ml per hour Oral fluid administration may be acceptable in burns up to 40% TBSA if IV supplies are limited Slide 59 SOF TTPs Extended Tactical Field Care Considerations Wound care management Irrigate and redress wounds (any potable water can be used for irrigation) Debride only obviously devitalized tissue Change dressings every 24 hours Consider converting to silver impregnated dressings to reduce frequency of dressing changes Continue antibiotics Repeat moxifloxacin (Avelox) 400 mg PO or ertapenem (Invanz) 1 gm IV/IO/IM every 24 hours Slide 60 20
21 SOF TTPs Extended Tactical Field Care Considerations Analgesia For painful procedures consider the use of procedural anesthesia Dual agent Midazolam (Versed) 2 mg IV/IO over 1 minute Ketamine (Ketalar) 20 mg IV/IO over 1 minute Single agent Morphine 5 mg IV/IO q 5 min Consider local blocks for pain management Slide 61 SOF TTPs Extended Tactical Field Care Considerations Nutrition management Consider oral nutrition if evacuation will be delayed by over 24 hours Orthopedic injury management Traction splints as needed Reassess fractures and adjust splints as needed Slide 62 SOF TTPs Extended Tactical Field Care Considerations Compartment syndrome management Be suspicious of compartment syndrome in the following conditions Fractures Crush injuries Vascular injuries Circumferential burns Multiple penetrating injuries (fragmentation) Slide 63 21
22 SOF TTPs Extended Tactical Field Care Considerations Clinical signs of compartment syndrome Pain out of proportion to injury Pain with passive motion of muscles in the involved compartment Pallor Paresthesias Pulselessness Consider use of compartment pressure monitor if available and trained in its use Slide 64 SOF TTPs Extended Tactical Field Care Considerations Compartment syndrome management Reevaluate every 30 minutes for first two hours then once every hour Maintain extremity at heart level Loosen encircling dressings Fasciotomy Only consider if evacuation is delayed over 6 hours Only perform if within your scope of practice Slide 65 SOF TTPs Extended Tactical Field Care Considerations Blast injuries Tympanic membrane perforation Dexamethasone (Decadron) 10 mg IV/IO/IM/PO QD Lungs Monitor patient for respiratory deterioration Abdomen Monitor for delayed bowel injury Spine Slide 66 22

23 Tactical Evacuation Care Treatment Priorities Slide 67 Tactical Evacuation Care Airway management Continue to monitor the casualty s airway and upgrade as needed Consider replacing advanced airway bulbs with saline prior to aircraft CASEVAC Breathing Continue to reassess Perform thoracostomy if needed Provide oxygen if available Slide 68 Tactical Evacuation Care Bleeding Reassess patient and verify bleeding is controlled Verify distal pulses are absent in extremities with tourniquets Reassess if tourniquet is required or other hemorrhage control means are appropriate Slide 69 23
24 Tactical Evacuation Care Hypothermia management Continue hypothermia prevention management or initiate if not already started Utilize heating system on evacuation platform and avoid wind exposure Use an IV warming device for all fluid administration Slide 70 Tactical Evacuation Care Intravenous (IV) access Reassess IV patency Flush IV lines and saline locks as required TXA If needed and not already started Fluid resuscitation Continue resuscitation as needed Maintain a normal radial pulse or systolic blood pressure between mmhg Slide 71 Tactical Evacuation Care Burn Treatment Continue fluid resuscitation with Rule of Tens Consider urinary catheter to monitor output Head injury management Continue to prevent hypotension and hypoxia Controlled mild hyperventilation If CO2 monitor available pco2 of 30 mmhg If no CO2 monitor 20 BPM Slide 72 24
25 Tactical Evacuation Care Penetrating eye trauma Cover with rigid eye shield if not already done Monitoring Institute pulse oximetry and other electronic monitoring of vital signs, if indicated Inspect and dress known wounds if not already done Check for additional wounds Slide 73 Tactical Evacuation Care Continue analgesia as needed Reassess fractures and recheck pulses Monitor air pressure in extremity air splints during air evacuation Start antibiotic therapy if not already done Slide 74 Tactical Evacuation Care The Pneumatic Antishock Garment (PASG) may be useful for stabilizing pelvic fractures and controlling pelvic and abdominal bleeding Application and extended use must be carefully monitored Contraindicated for casualties with thoracic or brain injuries Slide 75 25
26 Tactical Evacuation Care Document Clinical assessments, treatments rendered, and changes in casualty s status on a TCCC Casualty Card Forward this Information with the casualty to the next level of care Slide 76 Questions? Slide 77 Terminal Learning Objective Action: Communicate knowledge of Tactical Combat Casualty Care (TCCC) and SOF Tactical Trauma Protocols (TTPs) Condition: Given a lecture in a classroom environment Standard: Received a minimum score of 75% on the written exam and a GO on the practical exam IAW course standards Slide 78 26

27 Agenda Outline the origins, history, and objectives of TCCC and SOF TTPs Identify the three phases of TCCC and SOF TTPs Identify the Care Under Fire treatment priorities Identify the treatment priorities Slide 79 Agenda Identify the SOF TTPs extended Tactical Field Care considerations Identify the Tactical Evacuation Care treatment priorities Slide 80 Reason Slide 81 27
Tactical Combat Casualty Care Guidelines
 Tactical Combat Casualty Care Guidelines 18 August 2010 * All changes to the guidelines made since those published in the 2006 Sixth Edition of the PHTLS Manual are shown in bold text. The new material
Tactical Combat Casualty Care Guidelines 18 August 2010 * All changes to the guidelines made since those published in the 2006 Sixth Edition of the PHTLS Manual are shown in bold text. The new material
Tactical Combat Casualty Care Guidelines
 Tactical Combat Casualty Care Guidelines February 2009 * The only change in these updated TCCC guidelines from the July 2008 version is that WoundStat has been removed as a recommended hemostatic agent.
Tactical Combat Casualty Care Guidelines February 2009 * The only change in these updated TCCC guidelines from the July 2008 version is that WoundStat has been removed as a recommended hemostatic agent.
Tactical Combat Casualty Care Guidelines - 8 August Basic Management Plan for Care Under Fire
 Tactical Combat Casualty Care Guidelines - 8 August 2011 * All changes to the guidelines made since those published in the 2010 Seventh Edition of the PHTLS Manual are shown in bold text. The most recent
Tactical Combat Casualty Care Guidelines - 8 August 2011 * All changes to the guidelines made since those published in the 2010 Seventh Edition of the PHTLS Manual are shown in bold text. The most recent
Tactical Combat Casualty Care Guidelines for All Combatants
 Tactical Combat Casualty Care Guidelines for All Combatants August 2017 (Based on TCCC Guidelines for Medical Personnel 170131) These recommendations are intended to be guidelines only and are not a substitute
Tactical Combat Casualty Care Guidelines for All Combatants August 2017 (Based on TCCC Guidelines for Medical Personnel 170131) These recommendations are intended to be guidelines only and are not a substitute
Tactical Combat Casualty Care Guidelines
 Tactical Combat Casualty Care Guidelines 17 September 2012 * All changes to the guidelines made since those published in the 2010 Seventh Edition of the PHTLS Manual are shown in bold text. The most recent
Tactical Combat Casualty Care Guidelines 17 September 2012 * All changes to the guidelines made since those published in the 2010 Seventh Edition of the PHTLS Manual are shown in bold text. The most recent
Tactical Combat Casualty Care Guidelines
 Tactical Combat Casualty Care Guidelines 2 June 2014 (Includes all changes through #14-01) These recommendations are intended to be guidelines only and are not a substitute for clinical judgment. Basic
Tactical Combat Casualty Care Guidelines 2 June 2014 (Includes all changes through #14-01) These recommendations are intended to be guidelines only and are not a substitute for clinical judgment. Basic
Tactical Combat Casualty Care Guidelines
 Tactical Combat Casualty Care Guidelines 2 June 2014 Basic Management Plan for Care Under Fire 1. Return fire and take cover. 2. Direct or expect casualty to remain engaged as a combatant if appropriate.
Tactical Combat Casualty Care Guidelines 2 June 2014 Basic Management Plan for Care Under Fire 1. Return fire and take cover. 2. Direct or expect casualty to remain engaged as a combatant if appropriate.
TCCC Guidelines for Medical Personnel
 TCCC Guidelines for Medical Personnel 31 January 2017 RED text indicates changes to current wording or new text. BLUE text indicates unchanged prior wording that was shifted to a different location in
TCCC Guidelines for Medical Personnel 31 January 2017 RED text indicates changes to current wording or new text. BLUE text indicates unchanged prior wording that was shifted to a different location in
Student Handout - TCCC for Medical Personnel
 Basic Management Plan for Care Under Fire 1. Return fire and take cover. 2. Direct or expect casualty to remain engaged as a combatant if appropriate. 3. Direct casualty to move to cover and apply self-aid
Basic Management Plan for Care Under Fire 1. Return fire and take cover. 2. Direct or expect casualty to remain engaged as a combatant if appropriate. 3. Direct casualty to move to cover and apply self-aid
TCCC Guidelines for Medical Personnel
 TCCC Guidelines for Medical Personnel 1 August 2018 RED text indicates new text in this year s update to the TCCC Guidelines, which includes the recent changes on extraglottic airways and management of
TCCC Guidelines for Medical Personnel 1 August 2018 RED text indicates new text in this year s update to the TCCC Guidelines, which includes the recent changes on extraglottic airways and management of
Tactical Combat Casualty Care for Medical Personnel 03 June Tactical Evacuation Care
 Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Evacuation Care OBJECTIVES DESCRIBE the differences between MEDEVAC and CASEVAC DESCRIBE the differences between Tactical Field
Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Evacuation Care OBJECTIVES DESCRIBE the differences between MEDEVAC and CASEVAC DESCRIBE the differences between Tactical Field
Tactical Combat Casualty Care
 Chapter 37 Introduction For US military men and women wounded on the battlefield, the most critical phase of care is the period from the time of injury until the time that they arrive at a medical treatment
Chapter 37 Introduction For US military men and women wounded on the battlefield, the most critical phase of care is the period from the time of injury until the time that they arrive at a medical treatment
Tactical Evacuation Care
 Tactical Combat Casualty Care for Medical Personnel August 2017 (Based on TCCC-MP Guidelines 170131) Tactical Evacuation Care OBJECTIVES DESCRIBE the differences between MEDEVAC and CASEVAC DESCRIBE the
Tactical Combat Casualty Care for Medical Personnel August 2017 (Based on TCCC-MP Guidelines 170131) Tactical Evacuation Care OBJECTIVES DESCRIBE the differences between MEDEVAC and CASEVAC DESCRIBE the
Tactical Emergency Casualty Care (TECC) First Care Provider Guidelines
 First Care Provider Guidelines") Adopted from The Committee for TECC: Current as of June 2016 DIRECT THREAT CARE (DTC) / HOT ZONE GUIDELINES 1. In the presence of a direct threat to life, take definitive action towards mitigating that
Adopted from The Committee for TECC: Current as of June 2016 DIRECT THREAT CARE (DTC) / HOT ZONE GUIDELINES 1. In the presence of a direct threat to life, take definitive action towards mitigating that
Tactical Emergency Casualty Care (TECC)
") Tactical Emergency Casualty Care (TECC) Guidelines For First Care Providers Current as of June 2016 DIRECT THREAT CARE (DTC) / HOT ZONE GUIDELINES 1) In the presence of a direct threat to life, take definitive
Tactical Emergency Casualty Care (TECC) Guidelines For First Care Providers Current as of June 2016 DIRECT THREAT CARE (DTC) / HOT ZONE GUIDELINES 1) In the presence of a direct threat to life, take definitive
PRE-TRANSFUSION GUIDELINES
 PRE-TRANSFUSION GUIDELINES TACTICAL COMBAT CASUALTY CARE PATIENT STABILIZATION REQUIREMENTS HEMORRHAGE Bleeding is CONTROLLED by use of pressure dressing, tourniquet or fibrin bandage AIRWAY Secured and
PRE-TRANSFUSION GUIDELINES TACTICAL COMBAT CASUALTY CARE PATIENT STABILIZATION REQUIREMENTS HEMORRHAGE Bleeding is CONTROLLED by use of pressure dressing, tourniquet or fibrin bandage AIRWAY Secured and
TACTICAL COMBAT CASUALTY CARE (TCCC / TC3)
") tactical combat casualty care quick reference guide first edition Copyright 2017 (TCCC / TC3) EDITOR: HAROLD R. MONTGOMERY, ATP MSG(RET), U.S. ARMY CONSULTANTS & REVIEWERS FRANK K. BUTLER, MD CAPT(RET),
tactical combat casualty care quick reference guide first edition Copyright 2017 (TCCC / TC3) EDITOR: HAROLD R. MONTGOMERY, ATP MSG(RET), U.S. ARMY CONSULTANTS & REVIEWERS FRANK K. BUTLER, MD CAPT(RET),
Tactical Emergency Casualty Care (TECC) Guidelines for First Responders with a Duty to Act
 Guidelines for First Responders with a Duty to Act") Tactical Emergency Casualty Care (TECC) Guidelines for First Responders with a Duty to Act (Law Enforcement, Fire fighters not trained as EMS providers) Current as of March 2019 DIRECT THREAT CARE (DTC)
Tactical Emergency Casualty Care (TECC) Guidelines for First Responders with a Duty to Act (Law Enforcement, Fire fighters not trained as EMS providers) Current as of March 2019 DIRECT THREAT CARE (DTC)
TCCC Critical Decision Case Studies
 TCCC Critical Decision Case Studies August 2017 The Biggest Challenge in TCCC Knowing WHEN to use the interventions taught in TCCC Based on a suggestion by COL Bob Mabry TCCC Critical Decision Case Studies
TCCC Critical Decision Case Studies August 2017 The Biggest Challenge in TCCC Knowing WHEN to use the interventions taught in TCCC Based on a suggestion by COL Bob Mabry TCCC Critical Decision Case Studies
Tactical Emergency Casualty Care (TECC) Guidelines for BLS/ALS Medical Providers Current as of May 2017
 Guidelines for BLS/ALS Medical Providers Current as of May 2017") Tactical Emergency Casualty Care (TECC) Guidelines for BLS/ALS Medical Providers Current as of May 2017 DIRECT THREAT CARE (DTC) / HOT ZONE Guidelines : 1. Mitigate any immediate threat and move to a safer
Tactical Emergency Casualty Care (TECC) Guidelines for BLS/ALS Medical Providers Current as of May 2017 DIRECT THREAT CARE (DTC) / HOT ZONE Guidelines : 1. Mitigate any immediate threat and move to a safer
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE #2 IN TCCC-MP
 INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE #2 IN TCCC-MP 160603 1 1. Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Field Care #2 2. 5. Intravenous (IV) access Start an 18-gauge
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE #2 IN TCCC-MP 160603 1 1. Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Field Care #2 2. 5. Intravenous (IV) access Start an 18-gauge
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 504 Conduct Triage TERMINAL LEARNING OBJECTIVES 1. Given multiple casualties in a tactical environment, conduct
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 504 Conduct Triage TERMINAL LEARNING OBJECTIVES 1. Given multiple casualties in a tactical environment, conduct
INSTRUCTOR GUIDE FOR TCCC CRITICAL DECISION CASE STUDIES IN TCCC-MP
 INSTRUCTOR GUIDE FOR TCCC CRITICAL DECISION CASE STUDIES IN TCCC-MP 180801 1 1. TCCC Critical Decision Case Studies August 2017 2. Disclaimer The opinions or assertions contained herein are the private
INSTRUCTOR GUIDE FOR TCCC CRITICAL DECISION CASE STUDIES IN TCCC-MP 180801 1 1. TCCC Critical Decision Case Studies August 2017 2. Disclaimer The opinions or assertions contained herein are the private
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 509 Perform Casualty Assessment TERMINAL LEARNING OBJECTIVE 1. Given a patient in an operational environment,
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 509 Perform Casualty Assessment TERMINAL LEARNING OBJECTIVE 1. Given a patient in an operational environment,
Tactical Combat Casualty Care for Medical Personnel 03 June Tactical Field Care #3
 Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Field Care #3 Tactical Field Care Guidelines 14. Splint fractures and recheck pulse. Fractures: Open or Closed Open Fracture associated
Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Field Care #3 Tactical Field Care Guidelines 14. Splint fractures and recheck pulse. Fractures: Open or Closed Open Fracture associated
INSTRUCTOR GUIDE FOR TCCC SCENARIOS
 INSTRUCTOR GUIDE FOR TCCC SCENARIOS 180801 1 1. Tactical Combat Casualty Care for Medical Personnel August 2017 (Based on TCCC-MP Guidelines 180801) TCCC Scenarios We ve talked about the basic TCCC trauma
INSTRUCTOR GUIDE FOR TCCC SCENARIOS 180801 1 1. Tactical Combat Casualty Care for Medical Personnel August 2017 (Based on TCCC-MP Guidelines 180801) TCCC Scenarios We ve talked about the basic TCCC trauma
TCCC for All Combatants 1708 Tactical Field Care Instructor Guide 1
 TCCC for All Combatants 1708 Tactical Field Care Instructor Guide 1 1. Tactical Combat Casualty Care for All Combatants August 2017 (Based on TCCC-MP Guidelines 170131) Tactical Field Care Next we ll be
TCCC for All Combatants 1708 Tactical Field Care Instructor Guide 1 1. Tactical Combat Casualty Care for All Combatants August 2017 (Based on TCCC-MP Guidelines 170131) Tactical Field Care Next we ll be
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE #2 IN TCCC-MP
 INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE #2 IN TCCC-MP 1708 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 170131) Tactical Field Care #2 We will continue
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE #2 IN TCCC-MP 1708 1 Tactical Combat Casualty Care for Medical Personnel 1. August 2017 (Based on TCCC-MP Guidelines 170131) Tactical Field Care #2 We will continue
AIRWAY Management. How to manage an airway on the battlefield TRAININGGROUNDS
 TRAININGGROUNDS How to manage an airway on the battlefield CRAWL TRAININGGROUNDS What is Airway? A Compromised airway is one of the three leading cause of preventable death on the battlefield Airway management
TRAININGGROUNDS How to manage an airway on the battlefield CRAWL TRAININGGROUNDS What is Airway? A Compromised airway is one of the three leading cause of preventable death on the battlefield Airway management
Tactical Combat Casualty Care for Medical Personnel August (Based on TCCC-MP Guidelines ) TCCC Scenarios
 TCCC Scenarios") Tactical Combat Casualty Care for Medical Personnel August 2017 (Based on TCCC-MP Guidelines 170131) TCCC Scenarios Tactical Casualty Scenarios If the basic TCCC combat trauma management plan doesn t work
Tactical Combat Casualty Care for Medical Personnel August 2017 (Based on TCCC-MP Guidelines 170131) TCCC Scenarios Tactical Casualty Scenarios If the basic TCCC combat trauma management plan doesn t work
JOINT TRAUMA SYSTEM CLINICAL PRACTICE GUIDELINE
 JOINT TRAUMA SYSTEM CLINICAL PRACTICE GUIDELINE Burn Care Approved November 2013 Burn Care Goal. The goal of this CPG is to provide practical, evidence-based, recommendations for optimal care of burn casualties
JOINT TRAUMA SYSTEM CLINICAL PRACTICE GUIDELINE Burn Care Approved November 2013 Burn Care Goal. The goal of this CPG is to provide practical, evidence-based, recommendations for optimal care of burn casualties
Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Cardiac Arrest General This protocol should be followed for all adult cardiac arrests. Medical cardiac arrest patients undergoing attempted resuscitation should not
Date: November 15, 2012 Page 1 of 5 Cardiac Arrest General This protocol should be followed for all adult cardiac arrests. Medical cardiac arrest patients undergoing attempted resuscitation should not
Bleeding: Chapter 22 page 650
 Bleeding: Chapter 22 page 650 The Significance of Bleeding When patient have serious external blood loss it is often difficult to determine the amount of blood that is present because it may be absorbed
Bleeding: Chapter 22 page 650 The Significance of Bleeding When patient have serious external blood loss it is often difficult to determine the amount of blood that is present because it may be absorbed
ADMINISTRATIVE PROBLEMS
 ADMINISTRATIVE PROBLEMS Questions of an administrative nature (missing pages in subcourse, etc.) should be addressed to your primary instructor (group leader). If you have questions of an administrative
ADMINISTRATIVE PROBLEMS Questions of an administrative nature (missing pages in subcourse, etc.) should be addressed to your primary instructor (group leader). If you have questions of an administrative
Chapter 9 Airway Respirations Metabolism Oxygen Requirements Respiratory Anatomy Respiratory Anatomy Respiratory Anatomy Diaphragm
 1 Chapter 9 Airway 2 Respirations Every cell of the body requires to survive Oxygen must come in and carbon must go out 3 Metabolism Metabolism--Process where the body s cells convert food to Adequate
1 Chapter 9 Airway 2 Respirations Every cell of the body requires to survive Oxygen must come in and carbon must go out 3 Metabolism Metabolism--Process where the body s cells convert food to Adequate
Virginia Office of Emergency Medical Services Scope of Practice - Procedures for EMS Personnel
 Specific tasks in this document shall refer to the Virginia Education Standards. AIRWAY TECHNIQUES Airway Adjuncts Airway Maneuvers Alternate Airway Devices Oropharyngeal Airway Nasopharyngeal Airway Head
Specific tasks in this document shall refer to the Virginia Education Standards. AIRWAY TECHNIQUES Airway Adjuncts Airway Maneuvers Alternate Airway Devices Oropharyngeal Airway Nasopharyngeal Airway Head
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC FMST 501. Blast Related Injuries
 UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 501 Blast Related Injuries TERMINAL LEARNING OBJECTIVE. 1. Given a mission, Commander's guidance and intent,
UNITED STATES MARINE CORPS FIELD MEDICAL TRAINING BATTALION Camp Lejeune, NC 28542-0042 FMST 501 Blast Related Injuries TERMINAL LEARNING OBJECTIVE. 1. Given a mission, Commander's guidance and intent,
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES
 CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Subject References Emergency Medical Services Administrative Policies and Procedures Critical
CENTRAL CALIFORNIA EMERGENCY MEDICAL SERVICES A Division of the Fresno County Department of Public Health Manual Subject References Emergency Medical Services Administrative Policies and Procedures Critical
Prehospital Hemorrhage Control and Resuscitation
 Prehospital Hemorrhage Control and Resuscitation John B. Holcomb, MD, FACS Professor of Surgery Chief, Division of Acute Care Surgery Director, Center for Translational Injury Research University of Texas
Prehospital Hemorrhage Control and Resuscitation John B. Holcomb, MD, FACS Professor of Surgery Chief, Division of Acute Care Surgery Director, Center for Translational Injury Research University of Texas
Rescue Swimmer Refresher Course. Practical First Aid Training/Mock Trauma LT 2.2
 Rescue Swimmer Refresher Course Practical First Aid Training/Mock Trauma LT 2.2 Enabling Objectives Respond to an emergency per current American Red Cross standards. Administer CPR per current American
Rescue Swimmer Refresher Course Practical First Aid Training/Mock Trauma LT 2.2 Enabling Objectives Respond to an emergency per current American Red Cross standards. Administer CPR per current American
1 out of every 5,555 of drivers dies in car accidents 1 out of every 7692 pregnant women die from complications 1 out of every 116,666 skydives ended
 1 out of every 5,555 of drivers dies in car accidents 1 out of every 7692 pregnant women die from complications 1 out of every 116,666 skydives ended in a fatality in 2000 1 out of every 126,626 marathon
1 out of every 5,555 of drivers dies in car accidents 1 out of every 7692 pregnant women die from complications 1 out of every 116,666 skydives ended in a fatality in 2000 1 out of every 126,626 marathon
SALT LAKE EMS DISTRICT (Official Protocol No.06)
") Protocol No. 06 MASS CASUALTY INCIDENT PLAN Revised 2003 The Salt Lake EMS District has adopted the Utah Mass Casualty Incident Plan. Several modifications particular to the Salt Lake EMS District have
Protocol No. 06 MASS CASUALTY INCIDENT PLAN Revised 2003 The Salt Lake EMS District has adopted the Utah Mass Casualty Incident Plan. Several modifications particular to the Salt Lake EMS District have
WARNING WARNING BATTLEFIELD CASUALTY DRILLS AIDE MEMOIRE FIFTH EDITION JANUARY Crown Copyright ALL RIGHTS RESERVED
 BATTLEFIELD CASUALTY DRILLS WARNING Disposable gloves to be worn where possible to prevent cross infection of blood borne diseases WARNING AIDE MEMOIRE ARMY CODE 71638 FIFTH EDITION JANUARY 2007 Crown
BATTLEFIELD CASUALTY DRILLS WARNING Disposable gloves to be worn where possible to prevent cross infection of blood borne diseases WARNING AIDE MEMOIRE ARMY CODE 71638 FIFTH EDITION JANUARY 2007 Crown
OUTLINE SHEET Respond to an emergency per current American Red Cross standards.
 INTRODUCTION OUTLINE SHEET 2.2-1 PRACTICAL FIRST AID TRAINING/MOCK TRAUMA PAGE 1 of 8 First Aid, in any situation, consists of emergency treatment of the sick or injured before medical help can be obtained.
INTRODUCTION OUTLINE SHEET 2.2-1 PRACTICAL FIRST AID TRAINING/MOCK TRAUMA PAGE 1 of 8 First Aid, in any situation, consists of emergency treatment of the sick or injured before medical help can be obtained.
The development of this workbook was undertaken by trainers and developers within SAMPLE
 FOREWORD This publication is one of a number of workbooks produced by The Australian Medical Association (WA) Inc as a resource for the health sector. It is utilised within AMA Recruitment and Training
FOREWORD This publication is one of a number of workbooks produced by The Australian Medical Association (WA) Inc as a resource for the health sector. It is utilised within AMA Recruitment and Training
War Surgery Dr. Abdulwahid INTRODUCTION: AIRWAY, BREATHING
 War Surgery Dr. Abdulwahid INTRODUCTION: AIRWAY, BREATHING The aims of war surgery: Save life Avoid infectious complications Save limbs Minimize residual disability The outcome is influenced by: Type of
War Surgery Dr. Abdulwahid INTRODUCTION: AIRWAY, BREATHING The aims of war surgery: Save life Avoid infectious complications Save limbs Minimize residual disability The outcome is influenced by: Type of
Other diseases or age process
 1 BLS For Healthcare Providers 2 Time is Critical! begins to die in 4 to 6 minutes Brain matter cannot regenerate itself In order to sustain life, the human body must have going in and out and must be
1 BLS For Healthcare Providers 2 Time is Critical! begins to die in 4 to 6 minutes Brain matter cannot regenerate itself In order to sustain life, the human body must have going in and out and must be
CANDIDATE S RANK AND NAME CANDIDATE #
 EFMB Test Score Sheet TCCC PERFORM A TACTICAL COMBAT CASUALTY CARE PATIENT ASSESSMENT (For use of this form, see AMEDDC&S Pam 350-10, the proponent is MCCS-OP-T) CANDIDATE S RANK AND NAME CANDIDATE # TASK:
EFMB Test Score Sheet TCCC PERFORM A TACTICAL COMBAT CASUALTY CARE PATIENT ASSESSMENT (For use of this form, see AMEDDC&S Pam 350-10, the proponent is MCCS-OP-T) CANDIDATE S RANK AND NAME CANDIDATE # TASK:
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE #1 IN TCCC-MP
 INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE #1 IN TCCC-MP 160603 1 1. Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Field Care #1 Next we ll be moving into the Tactical Field Care
INSTRUCTOR GUIDE FOR TACTICAL FIELD CARE #1 IN TCCC-MP 160603 1 1. Tactical Combat Casualty Care for Medical Personnel 03 June 2016 Tactical Field Care #1 Next we ll be moving into the Tactical Field Care
2.This section will move into the Airway Management, Rescue Breaths & Cardiopulmonary Resuscitation (CPR).
.") Wilderness First Aid Fundamentals The period between the World Wars saw an increased awareness in personal first aid training. To cover all eventualities, from accidents at work to travel in foreign lands.
Wilderness First Aid Fundamentals The period between the World Wars saw an increased awareness in personal first aid training. To cover all eventualities, from accidents at work to travel in foreign lands.
Nitrous Oxide Sedation
 Princess Margaret Hospital for Children GUIDELINE Nitrous Oxide Sedation Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
Princess Margaret Hospital for Children GUIDELINE Nitrous Oxide Sedation Scope (Staff): Scope (Area): All Emergency Department Clinicians Emergency Department This document should be read in conjunction
SPEMS SKILLS PROFICIENCY CRITERIA Paramedic
 SPEMS SKILLS PROFICIENCY CRITERIA Paramedic The following skills are required at the Paramedic Level: 1. King Airway 2. IV 3. Endotracheal Intubation 4. Adult EZ IO 5. Pedi EZ IO 6. Pleural Decompression
SPEMS SKILLS PROFICIENCY CRITERIA Paramedic The following skills are required at the Paramedic Level: 1. King Airway 2. IV 3. Endotracheal Intubation 4. Adult EZ IO 5. Pedi EZ IO 6. Pleural Decompression
BASIC KNOWLEDGE OF LABORATORY FIRST AID
 BASIC KNOWLEDGE OF LABORATORY FIRST AID RV: 02/02/2015 prevencio@uv.es Page 1 of 7 . General issues to be considered by the rescuer in the event of an accident are described below: - Proceed as follows:
BASIC KNOWLEDGE OF LABORATORY FIRST AID RV: 02/02/2015 prevencio@uv.es Page 1 of 7 . General issues to be considered by the rescuer in the event of an accident are described below: - Proceed as follows:
A V A L A N C H E R E S C U E
 AVALANCHE RESCUE The On-Site Triage And Evacuation Of Avalanche Victims Statistics De Quervain s Mortality Curve 1945 to 1979 and 1979 to 1989 2,611 cases, buried at average 1.06 m After 1 hour 30-40%
AVALANCHE RESCUE The On-Site Triage And Evacuation Of Avalanche Victims Statistics De Quervain s Mortality Curve 1945 to 1979 and 1979 to 1989 2,611 cases, buried at average 1.06 m After 1 hour 30-40%
Emergency Medical Retrieval Service (EMRS) Standard Operating Procedure Public Distribution
 Standard Operating Procedure Public Distribution") Emergency Medical Retrieval Service (EMRS) www.emrs.scot.nhs.uk Standard Operating Procedure Public Distribution Title Burns Version 7 Related Documents British Burns Care Review Author A. Inglis, R. Price,
Emergency Medical Retrieval Service (EMRS) www.emrs.scot.nhs.uk Standard Operating Procedure Public Distribution Title Burns Version 7 Related Documents British Burns Care Review Author A. Inglis, R. Price,
Guarding for Organized Swim Groups
 Day 2 Inspection Guarding for Organized Swim Groups Organized groups may visit your facility. Day care groups Camps Youth organizations Groups can be part of your facility or an outside group They should
Day 2 Inspection Guarding for Organized Swim Groups Organized groups may visit your facility. Day care groups Camps Youth organizations Groups can be part of your facility or an outside group They should
Breathing Process: Inhalation
 Airway Chapter 6 Breathing Process: Inhalation Active part of breathing Diaphragm and intercostal muscles contract, allowing the lungs to expand. The decrease in pressure allows lungs to fill with air.
Airway Chapter 6 Breathing Process: Inhalation Active part of breathing Diaphragm and intercostal muscles contract, allowing the lungs to expand. The decrease in pressure allows lungs to fill with air.
COALINGA STATE HOSPITAL. Effective Date: August 31, 2006
 COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION Emergency Procedures POLICY NUMBER: 702 Effective Date: August 31, 2006 SUBJECT: CARDIOPULMONARY RESUSCITATION (CPR) 1. PURPOSE: To provide
COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION Emergency Procedures POLICY NUMBER: 702 Effective Date: August 31, 2006 SUBJECT: CARDIOPULMONARY RESUSCITATION (CPR) 1. PURPOSE: To provide
Adult Trauma Care. Space Coast Regional Emergency Medical Services. Adult Trauma Care
 2013 Standard Trauma Care Procedures Traumatic Injuries require prompt care and handling. Always suspect cervical injury. Note the mechanism of injury and other conditions that may affect patient care.
2013 Standard Trauma Care Procedures Traumatic Injuries require prompt care and handling. Always suspect cervical injury. Note the mechanism of injury and other conditions that may affect patient care.
FIELD FIRST AID CIOMR GUIDELINE
 FIELD FIRST AID CIOMR GUIDELINE v2.5 2016 ALGORITHM details on following pages - Always think security and call for help ASAP! - Master Drill: under fire / hostile / safe page 3 - Multiple casualties:
FIELD FIRST AID CIOMR GUIDELINE v2.5 2016 ALGORITHM details on following pages - Always think security and call for help ASAP! - Master Drill: under fire / hostile / safe page 3 - Multiple casualties:
FIRST AID. Study Topics. At a minimum, the following topics are to be studied for the first aid exam.
 FIRST AID Study Topics At a minimum, the following topics are to be studied for the first aid exam. TOPIC Avoid getting air in stomach during rescue breathing Burns Kinds of Burns & Care Calling for Help
FIRST AID Study Topics At a minimum, the following topics are to be studied for the first aid exam. TOPIC Avoid getting air in stomach during rescue breathing Burns Kinds of Burns & Care Calling for Help
Evidence Summary Recommendations for Pediatric Prehospital Protocols
 Evidence Summary Recommendations for Pediatric Prehospital Protocols Emergency Medical Services for Children State Partnership Purpose To provide summaries of existing evidence to address clinically-relevant
Evidence Summary Recommendations for Pediatric Prehospital Protocols Emergency Medical Services for Children State Partnership Purpose To provide summaries of existing evidence to address clinically-relevant
First Aid at Work Book (A4) First edition January 2013 (Reprinted August 2014) ISBN
 First edition January 2013 (Reprinted August 2014) ISBN") First Aid at Work Book (A4) First edition January 2013 (Reprinted August 2014) ISBN 978-1-907751-88-2 Second edition January 2016 ISBN 978-1-910964-16-3 Page number and previous content Page number and
First Aid at Work Book (A4) First edition January 2013 (Reprinted August 2014) ISBN 978-1-907751-88-2 Second edition January 2016 ISBN 978-1-910964-16-3 Page number and previous content Page number and
Mechanical Ventilation
 Mechanical Ventilation Chapter 4 Mechanical Ventilation Equipment When providing mechanical ventilation for pediatric casualties, it is important to select the appropriately sized bag-valve mask or endotracheal
Mechanical Ventilation Chapter 4 Mechanical Ventilation Equipment When providing mechanical ventilation for pediatric casualties, it is important to select the appropriately sized bag-valve mask or endotracheal
Adult, Child and Infant Exam
 CPR Pro for the Professional Rescuer Adult, Child and Infant Exam Instructions: Read each of the following questions carefully and then place an X over the correct answer on the separate answer sheet provided.
CPR Pro for the Professional Rescuer Adult, Child and Infant Exam Instructions: Read each of the following questions carefully and then place an X over the correct answer on the separate answer sheet provided.
JTTS CLINICAL PRACTICE GUIDELINES FOR HYPOTHERMIA PREVENTION, MONITORING AND MANAGEMENT
 1. REFERENCES: a. DoD Directive 6000.12, Health Services Operations and Readiness, 29 Apr 96 b. DoD Instruction 6430.2, DoD Medical Standardization Board, 17 Mar 97 c. HA Policy: 06-005, Defense-wide Policy
1. REFERENCES: a. DoD Directive 6000.12, Health Services Operations and Readiness, 29 Apr 96 b. DoD Instruction 6430.2, DoD Medical Standardization Board, 17 Mar 97 c. HA Policy: 06-005, Defense-wide Policy
MEDICAL GUIDANCE NOTE. Title: PROVISION OF MEDICAL CARE IN AN AUSTERE ENVIRONMNET, SPECIFICALLY IN A CONFINED SPACE Last revised: January 2011
 Title: PROVISION OF MEDICAL CARE IN AN AUSTERE ENVIRONMNET, SPECIFICALLY IN A CONFINED SPACE Last revised: January 2011 1. Background 1. The USAR environment presents the USAR medic with an array of ethical,
Title: PROVISION OF MEDICAL CARE IN AN AUSTERE ENVIRONMNET, SPECIFICALLY IN A CONFINED SPACE Last revised: January 2011 1. Background 1. The USAR environment presents the USAR medic with an array of ethical,
TCCC Guidelines Comprehensive Review and Update
 TCCC Guidelines Comprehensive Review and Update TCCC Guidelines Change 16-03 Harold R. Montgomery, ATP; Frank K. Butler, MD; Win Kerr, ATP; Curtis C. Conklin, ATP; Daniel M. Morissette, ATP; Michael A.
TCCC Guidelines Comprehensive Review and Update TCCC Guidelines Change 16-03 Harold R. Montgomery, ATP; Frank K. Butler, MD; Win Kerr, ATP; Curtis C. Conklin, ATP; Daniel M. Morissette, ATP; Michael A.
Surface Rescue Swimmer Course
 Surface Rescue Swimmer Course Secondary Survey LT 5.5 December 2003 1 Objective List the procedures for a secondary survey. Demonstrate secondary survey procedures in a mock trauma (moulage) scenario without
Surface Rescue Swimmer Course Secondary Survey LT 5.5 December 2003 1 Objective List the procedures for a secondary survey. Demonstrate secondary survey procedures in a mock trauma (moulage) scenario without
Basic Life Support Adult
 1/3.4.1 Version 4, 03/2016 Basic Life Support Adult CFR - A EFR Collapse Initiate mobilisation of 3 to 4 practitioners / responders Unresponsive and breathing abnormally or gasping 112 / 999 Go to Primary
1/3.4.1 Version 4, 03/2016 Basic Life Support Adult CFR - A EFR Collapse Initiate mobilisation of 3 to 4 practitioners / responders Unresponsive and breathing abnormally or gasping 112 / 999 Go to Primary
Soft Tissue Trauma. Lesson Goal. Lesson Objectives 9/10/2012. Recognize and manage various types of soft tissue injuries. State function of skin
 Soft Tissue Trauma Lesson Goal Recognize and manage various types of soft tissue injuries Lesson Objectives State function of skin List and describe 3 layers of skin Explain why BSI is a critical safety
Soft Tissue Trauma Lesson Goal Recognize and manage various types of soft tissue injuries Lesson Objectives State function of skin List and describe 3 layers of skin Explain why BSI is a critical safety
MICHIGAN. Table of Contents. State Protocols. Trauma and Environmental Emergencies
 MICHIGAN State Protocols Protocol Number Protocol Name Trauma and Environmental Emergencies Table of Contents 2.2 General Trauma 2.3 Burns 2.4 Crush Injury 2.5 Soft Tissue and Orthopedic Injuries 2.6 Spinal
MICHIGAN State Protocols Protocol Number Protocol Name Trauma and Environmental Emergencies Table of Contents 2.2 General Trauma 2.3 Burns 2.4 Crush Injury 2.5 Soft Tissue and Orthopedic Injuries 2.6 Spinal
AMBULANCE MAN. Name of Scout/Guide:
 AMBULANCE MAN Name of Scout/Guide: BIODATA Name: Troop: District: Patrol: BADGE REQUIREMENTS Date of Commencement: Date of Completion: Court of Honour Permission to Earn Badge Date:. Scout / Guide has
AMBULANCE MAN Name of Scout/Guide: BIODATA Name: Troop: District: Patrol: BADGE REQUIREMENTS Date of Commencement: Date of Completion: Court of Honour Permission to Earn Badge Date:. Scout / Guide has
RECOMMENDATIONS FOR THE MANAGEMENT OF CRUSH VICTIMS IN MASS DISASTERS
 ISSN 0931-0509 (Print) ISSN 1460-2385 (Online) Volume 27 Supplement 1 April 2012 RECOMMENDATIONS FOR THE MANAGEMENT OF CRUSH VICTIMS IN MASS DISASTERS (SHORT FIELD VERSION) Recommendations for the management
ISSN 0931-0509 (Print) ISSN 1460-2385 (Online) Volume 27 Supplement 1 April 2012 RECOMMENDATIONS FOR THE MANAGEMENT OF CRUSH VICTIMS IN MASS DISASTERS (SHORT FIELD VERSION) Recommendations for the management
INITIATE APPROPRIATE RESUSCITATION PER POLICY/PROTOCOL
 PATIENT ASSESSMENT ASSURE PATIENT HAS A PATENT AIRWAY LOOK, LISTEN AND FEEL TO CONFIRM APNEA CHECK F PULSE F MINIMUM OF 60 SECONDS TO CONFIRM PULSELESS CHECK PUPILLARY RESPONSE DOES PATIENT MEET OBVIOUS
PATIENT ASSESSMENT ASSURE PATIENT HAS A PATENT AIRWAY LOOK, LISTEN AND FEEL TO CONFIRM APNEA CHECK F PULSE F MINIMUM OF 60 SECONDS TO CONFIRM PULSELESS CHECK PUPILLARY RESPONSE DOES PATIENT MEET OBVIOUS
Pennsylvania Department of Health Behavioral & Poisoning 8031 ALS Adult/Peds POISONING/TOXIN EXPOSURE STATEWIDE ALS PROTOCOL
 INITIAL PATIENT CONTACT- SEE PROTOCOL #201 WARNING: EMS personnel must not enter confined spaces with potential toxic gases (e.g. manure pits, silos, spaces with carbon monoxide, spaces with industrial
INITIAL PATIENT CONTACT- SEE PROTOCOL #201 WARNING: EMS personnel must not enter confined spaces with potential toxic gases (e.g. manure pits, silos, spaces with carbon monoxide, spaces with industrial
Increasing the Ability to Survive in Critical Trauma Incidents. Richard M. Smith President, Con10gency Consulting, LLC
 Increasing the Ability to Survive in Critical Trauma Incidents Richard M. Smith President, Con10gency Consulting, LLC In 2017-346 Reported Mass Shooting Source: Gun Violence Archive gunviolencearchive.org
Increasing the Ability to Survive in Critical Trauma Incidents Richard M. Smith President, Con10gency Consulting, LLC In 2017-346 Reported Mass Shooting Source: Gun Violence Archive gunviolencearchive.org
Individual First Aid Kit (IFAK) Training
 Training") Individual First Aid Kit (IFAK) Training Individual First Aid Kit (IFAK) Product Description The IFAK is issued to every Soldier. Weighing one pound, the IFAK consists of the following six (6) expendable
Individual First Aid Kit (IFAK) Training Individual First Aid Kit (IFAK) Product Description The IFAK is issued to every Soldier. Weighing one pound, the IFAK consists of the following six (6) expendable
TACTICAL COMBAT CASUALTY CARE AND WOUND TREATMENT
 U.S. ARMY MEDICAL DEPARTMENT CENTER AND SCHOOL FORT SAM HOUSTON, TEXAS 78234-6100 TACTICAL COMBAT CASUALTY CARE AND WOUND TREATMENT SUBCOURSE MD0554 EDITION 200 DEVELOPMENT This subcourse is approved for
U.S. ARMY MEDICAL DEPARTMENT CENTER AND SCHOOL FORT SAM HOUSTON, TEXAS 78234-6100 TACTICAL COMBAT CASUALTY CARE AND WOUND TREATMENT SUBCOURSE MD0554 EDITION 200 DEVELOPMENT This subcourse is approved for
Life Support Programme
 Life Support Programme Summary of Changes to RLSS UK Life Support Programme Qualified deliverers The Life Support awards can be taught and assessed by: Lifesaving Instructor (and higher) Pool or Beach
Life Support Programme Summary of Changes to RLSS UK Life Support Programme Qualified deliverers The Life Support awards can be taught and assessed by: Lifesaving Instructor (and higher) Pool or Beach
LESSON ASSIGNMENT. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 1 Chest Trauma LESSON ASSIGNMENT Paragraphs 1-1 through 1-13. LESSON OBJECTIVES After completing this lesson, you should be able to: 1-1. Identify common signs, common treatment,
LESSON ASSIGNMENT LESSON 1 Chest Trauma LESSON ASSIGNMENT Paragraphs 1-1 through 1-13. LESSON OBJECTIVES After completing this lesson, you should be able to: 1-1. Identify common signs, common treatment,
First Aid - immediate care that is given to the victim of an injury or illness until experts can take over - Oftentimes, it s the difference between
 First Aid First Aid - immediate care that is given to the victim of an injury or illness until experts can take over - Oftentimes, it s the difference between life and death or recovery vs permanent disability
First Aid First Aid - immediate care that is given to the victim of an injury or illness until experts can take over - Oftentimes, it s the difference between life and death or recovery vs permanent disability
South Carolina Approved Skills by Certification Level
 Established 4/4/2010 Revised 2/13/2017 South Carolina Approved Skills by Certification Level The following checklist provides the approved Skills / Scope of practice for all levels of certification within
Established 4/4/2010 Revised 2/13/2017 South Carolina Approved Skills by Certification Level The following checklist provides the approved Skills / Scope of practice for all levels of certification within
An average of 700 people a year in the U.S. are murdered on the job.
 P R E P A R I N G F O R & R E S P O N D I N G T O A N ACTIVE SHOOTER OR INTENTIONAL MASS-CASUALTY An average of 700 people a year in the U.S. are murdered on the job. U.S. Bureau of Labor Statistics 1
P R E P A R I N G F O R & R E S P O N D I N G T O A N ACTIVE SHOOTER OR INTENTIONAL MASS-CASUALTY An average of 700 people a year in the U.S. are murdered on the job. U.S. Bureau of Labor Statistics 1
Accidents happen anywhere
 Bulletin 2325 Maine Farm Safety Program by Dawna L. Cyr, farm safety project assistant, and Steven B. Johnson, Ph.D., Extension crops specialist Basic First Aid Accidents happen anywhere and anytime. The
Bulletin 2325 Maine Farm Safety Program by Dawna L. Cyr, farm safety project assistant, and Steven B. Johnson, Ph.D., Extension crops specialist Basic First Aid Accidents happen anywhere and anytime. The
Basic Life Support Adult
 1/2.4.1 Version 4, 03/2016 Basic Life Support Adult Collapse If physically unable to ventilate perform compression only CPR Unresponsive and breathing abnormally or gasping 112 / 999 Shout for help 112
1/2.4.1 Version 4, 03/2016 Basic Life Support Adult Collapse If physically unable to ventilate perform compression only CPR Unresponsive and breathing abnormally or gasping 112 / 999 Shout for help 112
NOTE: If not used, provider must document reason(s) for deferring mechanical ventilation in a patient with an advanced airway
 for deferring mechanical ventilation in a patient with an advanced airway") APPENDIX: TITLE: Mechanical Ventilator Use REVISED: November 1, 2017 I. Introduction: Mechanical Ventilation is the use of an automated device to deliver positive pressure ventilation to a patient. Proper
APPENDIX: TITLE: Mechanical Ventilator Use REVISED: November 1, 2017 I. Introduction: Mechanical Ventilation is the use of an automated device to deliver positive pressure ventilation to a patient. Proper
National Registry of Emergency Medical Technicians Emergency Medical Technician Psychomotor Examination PATIENT ASSESSMENT/MANAGEMENT TRAUMA
 PATIENT ASSESSMENT/MANAGEMENT TRAUMA Scenario # Note: Areas denoted by ** may be integrated within sequence of Primary Survey/Resuscitation SCENE SIZE-UP Determines the scene/situation is safe 1 Determines
PATIENT ASSESSMENT/MANAGEMENT TRAUMA Scenario # Note: Areas denoted by ** may be integrated within sequence of Primary Survey/Resuscitation SCENE SIZE-UP Determines the scene/situation is safe 1 Determines
Chapter 10 First Aid and Field Sanitation
 Review Questions Chapter 10 First Aid and Field Sanitation 1. True or False. The three reasons for performing first aid are to save lives, prevent further injuries, and prevent infection? 1. True 2. False
Review Questions Chapter 10 First Aid and Field Sanitation 1. True or False. The three reasons for performing first aid are to save lives, prevent further injuries, and prevent infection? 1. True 2. False
LESSON PLAN January COURSE TITLE: Surface Rescue Swimmer Course, A TERMINAL OBJECTIVE: Partially supported by this lesson topic:
 LESSON PLAN January 2007 COURSE TITLE: Surface Rescue Swimmer Course, A-050-0500 CLASSIFICATION: Unclassified LESSON PLAN NUMBER: 5.4 LESSON TOPIC: Primary Survey ALLOTTED LESSON TIME: INSTRUCTIONAL SUPPORT:
LESSON PLAN January 2007 COURSE TITLE: Surface Rescue Swimmer Course, A-050-0500 CLASSIFICATION: Unclassified LESSON PLAN NUMBER: 5.4 LESSON TOPIC: Primary Survey ALLOTTED LESSON TIME: INSTRUCTIONAL SUPPORT:
PATIENT ASSESSMENT/MANAGEMENT TRAUMA
 Start Time: Stop Time: Date: Candidate s Name: Evaluator s Name: PATIENT ASSESSMENT/MANAGEMENT TRAUMA Takes, or verbalizes, body substance isolation precautions 1 SCENE SIZE-UP Determines the scene is
Start Time: Stop Time: Date: Candidate s Name: Evaluator s Name: PATIENT ASSESSMENT/MANAGEMENT TRAUMA Takes, or verbalizes, body substance isolation precautions 1 SCENE SIZE-UP Determines the scene is
EASTERN ARIZONA COLLEGE First Aid and CPR
 EASTERN ARIZONA COLLEGE First Aid and CPR Course Design 2016-2017 Course Information Division Allied Health Course Number EMT 122 Title First Aid and CPR Credits 2 Developed by Amy Ollerton Lecture/Lab
EASTERN ARIZONA COLLEGE First Aid and CPR Course Design 2016-2017 Course Information Division Allied Health Course Number EMT 122 Title First Aid and CPR Credits 2 Developed by Amy Ollerton Lecture/Lab
Lebanese Red Cross - Emergency Medical Services First Aid Training course Skills Summary Adult Airways Obstruction
 s Summary Adult Airways Obstruction Choking is recognized Rescuer asks if victim can speak, cough or breathe Rescuer encourages victim to cough in case of a partial obstruction 1 Adult Airway Obsturction
s Summary Adult Airways Obstruction Choking is recognized Rescuer asks if victim can speak, cough or breathe Rescuer encourages victim to cough in case of a partial obstruction 1 Adult Airway Obsturction
South Carolina Approved Skills by Certification Level
 Established 4/4/2010 Revised 1/2/2018 South Carolina Approved Skills by Certification Level The following checklist provides the approved Skills / Scope of practice for all levels of certification within
Established 4/4/2010 Revised 1/2/2018 South Carolina Approved Skills by Certification Level The following checklist provides the approved Skills / Scope of practice for all levels of certification within
Nitrous Oxide Oxygen Administration Protocol July 2002
 Nitrous Oxide Oxygen Administration Protocol July 2002 Preamble A patient s self-administration of a nitrous oxide-oxygen mixture can provide relief of acute pain, provided there are no contraindications
Nitrous Oxide Oxygen Administration Protocol July 2002 Preamble A patient s self-administration of a nitrous oxide-oxygen mixture can provide relief of acute pain, provided there are no contraindications
eacls TM Skill Performance
 eacls TM Skill Performance Directions for Instructors and Course Coordinators: The evaluation forms that follow are used to verify that participants in the ACEP eacls TM program can demonstrate competency
eacls TM Skill Performance Directions for Instructors and Course Coordinators: The evaluation forms that follow are used to verify that participants in the ACEP eacls TM program can demonstrate competency
Written Exam. Basic Life Support
 Written Exam Basic Life Support Instructions: Read each of the following questions carefully and then place an X over the correct answer on the separate answer sheet provided. Please do not write on the
Written Exam Basic Life Support Instructions: Read each of the following questions carefully and then place an X over the correct answer on the separate answer sheet provided. Please do not write on the
EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES
 GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
First Aid Lukáš Dadák, M.D. Dept. of Anesthesia &ICU FN USA
 First Aid 2011 Lukáš Dadák, M.D. Dept. of Anesthesia &ICU FN USA 15740@mail.muni.cz How to survive? Do not kill the patient. Reason of lectures - to pass the exam - to know important information for life
First Aid 2011 Lukáš Dadák, M.D. Dept. of Anesthesia &ICU FN USA 15740@mail.muni.cz How to survive? Do not kill the patient. Reason of lectures - to pass the exam - to know important information for life
Do your share as a good citizen in your school, community, country, and the world
 Lesson 3 Controlling Bleeding What You Will Learn to Do Determine first aid procedures for bleeding victim Linked Core Abilities Do your share as a good citizen in your school, community, country, and
Lesson 3 Controlling Bleeding What You Will Learn to Do Determine first aid procedures for bleeding victim Linked Core Abilities Do your share as a good citizen in your school, community, country, and