Effect of Foot Orthotics on Calcaneal Eversion During Standing and Treadmill Walking for Subjects With
|
|
|
- Alexis Bates
- 6 years ago
- Views:
Transcription
1 Journal of Orthopaedic & Sports Physical Therapy 2OOO;3O (1 1) : Effect of Foot Orthotics on Calcaneal Eversion During Standing and Treadmill Walking for Subjects With lean Mass6 Genova, MS, P7; OCS, ATC1 Michael T. Gross, PhD, PT2 Study Design: Repeated measures analysis of intervention. Objectives: To determine the effects of foot orthotics and shoewear on calcaneal eversion for standing and treadmill walking. Background: Foot orthotics are commonly used as an intervention for treating lower extremity musculoskeletal pathology. Qualitative research regarding the benefit of foot orthotics tends to be favorable, while the results of quantitative studies often conflict. Methods and Measures: Eight men (mean age = years) and 5 women (mean age = years), who demonstrated abnormal pronation, walked quickly (average velocity = 1.9 mls) on a treadmill with and without foot orthotics. Subjects were filmed using a 2dimensional video system and plastic molds designed to indicate calcaneal position inside the shoe during static standing and treadmill walking. Results: hired t tests indicated that foot orthotics significantly reduced the mean maximum calcaneal eversion angle by 2.2' and the mean calcaneal eversion angle at heel rise by 2.1" during fast walking. Orthotic and nonorthotic conditions did not differ significantly for the remaining kinematic variables. A one-way ANOVA indicated that calcaneal eversion in standing was significantly greater for barefoot standing compared with standing in shoes with or without orthotics. ANOVA also indicated that the plastic molds provided reliable measures of calcaneal position. Conclusions: Foot orthotics have a significant effect on calcaneal eversion and shoes also should be considered in conjunction with foot orthotic prescription. / Orthop Sports Phys Ther 2000;30: Key Words: calcaneal eversion, kinematics, orthotics, rearfoot Physical therapist, Duke Physical Therapy, Mebane Outpatient Community Office, Mebane, NC. Professor, Division of Physical Therapy, Program in Human Movement Science, University of North Carolina at Chapel Hill, NC. This protocol was approved by the Committee for the Protection of the Rights of Human Subjects at the University of North Carolina at Chapel Hill. Send correspondence tolean Mass6 Genova, Duke Physical Therapy, Mebane Outpatient Community Office, I00 A East Dogwood Drive, Mebane, NC masse@ntrnet.net P ronation is a normally occurring motion within the foot that consists of the motions of dorsiflexion, abduction, and eversion.2s Pronation assists with shock absorption and surface adaptation during the early portion of the stance phase of walking. Pronation may become abnormal when it occurs in excess, when its timing during stance is prolonged, or when it occurs at inappropriate times during stance phase." Abnormal pronation within the foot has been implicated in numerous lower extremity pathologies, including pelvic and hip dysfunct i ~ n, ' knee ~ pain,27 bunions," shin splints," stress fractures,i4 arthriti~,~%nd tendinitish Subotnick'" has defined abnormal pronation as maximum pronation occurring beyond 25% of stance phase for walking. Dahle et alquggested a foot type classification system to determine static pronated foot position based on visual observation and measures of the foot. The 3 criteria assessed in standing for abnormal pronation in this classification scheme are more than 3" of calcaneal ever-
2 sion, the presence of a medial talonavicular bulge, and a low magnitude medial longitudinal arch angle. Jonson and GrossIfi suggest a similar classification scheme based on their normative findings in 63 sub jects. They recommend classifying a foot as pronated if measures of calcaneal eversion are more than 1 standard deviation (3.0") larger than the mean (6.3"), and the longitudinal arch angle is more than one standard deviation (7.5") less than the mean (142.1") for their subject sample.* Abnormal subtalar joint pronation may cause prolonged and increased loads on the biologic structures of the foot? and may be evidenced by an increase in maximal calcaneal eversi~n.~.~.*~ Calcaneal eversion, the frontal plane component of subtalar joint pronation, has been used as an indicator of pronation by several inve~tigators.'~;~;~;~~ Abnormal pronation may occur late in stance phase, particularly in feet with forefoot varus malalignment, and may be evidenced by an increased calcaneal eversion angle at heel r i ~ e. ~ Excessive. * ~ pronation and pronation of the foot late in stance phase of gait may result in diminished force transmission and propulsion capabilitie~?*~ in addition to the application of abnormal ground reaction forces on the f o ~ t. ~ ~ ~ * ~ Foot orthotics are often used in the treatment of abnormal pronation to reduce the magnitude of this motion and influence its timing. Clinicians who fab ricate biomechanical foot orthoses may attempt to control abnormal motion with a post, or wedge, a p plied to the orthotic shell at the forefoot, the rearfoot, or both.* A rearfoot post is theorized to reposition the calcaneus in "neutral" to control calcaneal eversion during the initial portion of stance phase of gait.7j'~*s A forefoot post is theorized to normalize the position of the forefoot relative to the calcaneus and the ground by accommodating a forefoot varus or valgus malalignment.7j' This kinematic alteration of the position of the foot during walking may result in a more effective biomechanical relationship, particularly at the subtalar and midtarsal joints. A reduction in the magnitude of pronation and changes in the timing of pronation during stance phase of gait may reduce stress on lower quarter tissues. Qualitative research that examined patient satisfaction and return to function with the use of foot orthotics suggests that they are effective in the treat- ment of abnormal pronation.*.k7j1 Quantitative research regarding the efficacy of orthotic intervention to reduce pronation, however, is limited and controversial. Rodgers and Leveau2' reported no consistent changes in calcaneal kinematics with the use of foot orthotics in runners. They did not, however, describe inclusion criteria for their subjects (ie, abnormal pronation, pes caws, etc), nor did they report any initial * The reference landmarks for these measures are defined in the "Methods" section. effects of the orthotics on the subjects' foot position. McCulloch et all7 reported that foot orthotics significantly decreased calcaneal eversion during stance phase of walking and increased the duration of stance from heel strike to heel rise in their subject sample. Smith et adz5 reported that foot orthotics in a sample of runners significantly decreased maximum calcaneal eversion and the velocity of calcaneal eversion immediately after foot contact. Johanson et all5 reported that foot orthotics significantly reduced the calf-tocalcaneus and calcaneus-to-vertical angles during walking. Further research is needed to clarify existing kinematic studies pertaining to the effects of foot orthotics on lower quarter function. The purpose of this study, therefore, was to investigate the effects of foot orthotics on calcaneal kinematics during treadmill walking. A secondary purpose was to examine the effects of shoes and foot orthotics on static position of the calcaneus. The specific research questions addressed are listed below: 1. What is the effect of shoes and foot orthotics on static position of the calcaneus? 2. Do foot orthotics decrease the maximum calcanea1 eversion angle, the calcaneal eversion angle at heel rise, the time from heel contact to initiation of calcaneal inversion motion, or the percent of stance phase at which initiation of calcaneal inversion motion occurs during fast treadmill walking (60-80% of age-predicted maximum heart rate)? 3. What is the effect of foot orthotics on the duration of stance phase during fast treadmill walking? METHODS Subjects Seventeen potential subjects were recruited by advertising with fliers or by being identified through a review of patient records. These individuals reported they had previously received foot orthotics as ueatment for a lower quarter musculoskeletal complaint. Four of the potential subjects were excluded from the study because they did not meet the inclusion criteria for abnormal pronation that pertained to longitudinal arch angle and calcaneal angle. Thirteen healthy subjects, 8 men and 5 women, between the ages of 1 8 and 55 years were tested. They reported no lower extremity pain at the time of their participation and no history of hypertension, coronary disease, respiratory disease, or balance, metabolic, or neurological disorders. All subjects displayed a standing calcaneal eversion angle equal to or greater than 10" bilaterally and a longitudinal arch angle equal to or less than 134" bilaterally.'wl subjects also wore orthotics and reported being comfortable with them for at least 3 weeks before testing. The subjects were able to maintain a walking speed that allowed their J Orthop Sports Phys Ther.Volume 3O.Number 1 1.November
3 heart rate to remain in an aerobic training range, calculated as 6040% of the subject's maximum agepredicted heart rate. Maximum age-predicted heart rate was calculated as 220 minus the subject's age.g Walking with a heart rate in an aerobic range was incorporated into the study testing procedures to r e p resent a walking speed that might be used by individuals who were walking for aerobic exercise. Each subject signed a statement of informed consent and the study was approved by the Committee for the Protection of the Rights of Human Subjects at the University of North Carolina at Chapel Hill. Instrumentation A super VHS video camcorder filming at a speed of 60 fields per second was used to record 2dimensional calcaneal motion during treadmill ambulation.lj A VCR, time code generator, standard videotape, and television monitor also were used to obtain video records of the subjects. A standard meter stick with retroreflective markers at 0.2-meter increments, torpedo level, and measuring tape were used to define and calibrate the visual filming field. Sliding calipers were used to identify points of bisection of the distal leg and calcaneus. A 20.3-centimeters goniometer marked in ldegree increments was used to measure the subjects' calcaneal position. A Polar heart rate monitor with chest electrode (Polar CIC, Inc, Polar Electro--Oy, Finland) was applied to each subject to monitor heart rate during walking. The video recordings of calcaneal motion were digitized using the Peak Performance Technologies (Englewood, Co) automated digitization software. Subject Screening Procedure Each subject was positioned prone as the first author (J.M.G.) palpated each leg and made observations to record foot deformities such as calcaneal varus, forefoot varus, hallux valgus, and plantar flexed first ray. No attempt was made to measure the exact degree of any observable deformity. The first author palpated and marked the right leg with ink (Figure 1). The distal calcaneal mark was made at the base of the calcaneus, and the proximal calcaneal mark was 3 centimeters above the distal mark. The distal leg mark was 6 centimeters above the palpated proximal margin of the calcaneus, and the proximal leg mark was 8 centimeters above the distal leg mark. These marks were used as reference points for future calculated bisections of the leg. The distal calcaneal bisection was performed with the subject prone because the investigators thought that the calcaneal fat pad might be displaced with the subject standing and might alter the osseous bisection of the calcaneus. Straight edge calipers were placed at the medial and distal proximal "A *=proximal calcaneus I 1 I "=distal calcaneus I FIGURE 1. Schematic of method for bisecting the leg and calcaneus segments. The box on the left represents locations for the leg and calcaneal bisections in the frontal plane. The box on the right depicts the sagittal plane anterior-posterior locations of the calipers for each bisection point. lateral calcaneus at the level of the distal calcaneal mark to measure the width of the calcaneus and then mark the distal bisection point on it. The distance between the subject's anterior superior iliac spine (ASIS) was obtained with calipers to establish a consistent position for each subject to assume for all static standing measures. This measure was used as a reference to establish the distance between the lateral borders of the subject's feet for all static standing calcaneal measures. With the subject in the static standing position, calipers were used to establish the midpoint of the remaining 3 lower extremity marks previously described. At the proximal calcaneal mark, the caliper arms were placed at the medial and lateral calcaneas, 0.5 centimeters anterior to the proximal calcaneal mark (Figure 1). The distal leg bisection was made by placing the medial and lateral caliper arms 1 centimeter anterior to the distal leg mark. The proximal leg bisection was made by placing the medial and lateral caliper arms at the most medial and lateral points of the proximal leg at the level of the proximal leg mark. A line connecting the 2 leg points and a line connecting the 2 calcaneal points was drawn using a pen and a straight edge. Spherical retroreflective markers 14 millimeters in diameter were centered on each of the 4 bisection points of the right leg.ij The left leg and calcaneus were marked in the same manner, excluding the placement of retroreflective markers. The most medial aspects of the medial malleolus, the navicular tuberosity, and the first metatarsal head were marked with ink on both legs of each subject. Two weight-bearing measurements were made, based on the work of Jonson and Grossl%nd Dahle et al.'j Each subject was asked to stand in the static standing position for visualization of the calcaneus. The standing calcaneal eversion angle (Figure 2) was measured for both legs with the goniometer as the acute angle between the leg and calcaneal bisection lines (ICC [intraclass correlation coefficient] = J Orthop Sports Phys Ther.Volume SO Number 1 1 November 2000

4 for intratester and ICC = 0.86 for intertester reliability16). The static standing calcaneal angle for the right leg was then recorded videographically with the subject remaining in the static standing position. The longitudinal arch angle (Figure 3) was measured as the obtuse angle formed by a line connecting the medial malleolus and the navicular tuberosity, and a line between the navicular tuberosity and the most medial aspect of the first metatarsal head (ICCs for intratester and intertester reliability were 0.90 and 0.81, respectivelyi6). A subject's foot was considered pronated if the calcaneal eversion angle was equal to or more than lo0, and the longitudinal arch angle was less than 134".'~ubjects classified as not having a pronated foot type for both legs were excluded from the study. Only the right leg, however, was used for all analyses. The first author recorded the structural characteristics of each subject's foot orthotics, noting features such as rigidity, location of posting material, and length of the orthotic. The first author also inspected each subject's shoes for qualities of pronation control such as: straight lasting, board lasting, reinforced upper, firm heel counter, increased medial heel flare, decreased lateral heel flare, and increased density of medial midsole material.'2jr Shoes and foot orthotics were assessed qualitatively (Table 1). Subject Preparation Each subject's height, weight, age, and sex were recorded. The 2 calcaneal retroreflective markers were removed and the subject was asked to don shoes and socks without their orthotics. After colored water was applied to the sole of the right shoe, the subject was asked to walk quickly over butcher paper to provide a template modified from McPoillg to determine their preferred foot placement angle. The method for measuring foot placement angle is shown in Figure 4. According to Glaves,lo error for calcaneal angle measurements caused by out of plane motion is minimal for foot placement toe-out angles less than 20". No subject displayed a toe-out angle greater than 20" during this screening procedure (mean toeout angle = "). Each subject then walked on the treadmill at a comfortable walking speed, increasing the treadmill speed until their heart rate remained within their calculated aerobic training range for at least 3 minutes. This speed was recorded and used as the subject's test speed for subsequent data collection procedures. Thermoplastic Mold Preparation and Static Standing Measurements Movement of the posterior aspect of the shoe's heel counter may not reflect movement of the calca- FIGURE 2. Calcaneal eversion angle (8) measured as the acute angle between the distal midline of the leg and the midline of the calcaneus. neus inside the shoe. Polinsky2' devised a method to ensure reliable measurement of calcaneal motion within an unaltered shoe. A calcaneal mold marker was fabricated for each subject. A moldable therme plastic material (KaySplint Basic I, Sammons Preston, Bolingbrook, Ill) was placed on the calcaneus, and then extended upward and posteriorly over the outside of the heel counter of the shoe to represent the calcaneal position within the shoe (Figure 5). The mold was then secured to the subject's calcaneus using adhesive spray and cloth athletic tape. Care was taken to minimize support provided to the foot by the tape or the calcaneal mold. The area of athletic tape application was restricted to the medial and lateral portions of the heel. The subject then stood in the standardized foot width position without shoes. The thermoplastic mold, representing the calcaneal position, was marked to duplicate the previously measured standing calcaneal angle, a goniometer was adjusted to that angle and was aligned with the distal leg bisection and the thermoplastic extension. The line on the distal arm of the goniometer, representing the calcaneal position, was transferred to the thermoplastic material. The distal portion of the thermoplastic segment was then marked with a 14millimeter retroreflective marker. Another retroreflective marker was placed 3 centimeters above the distal marker on the thermoplastic material (Figure 1). J Orthop Sports Phys Ther.Volume SO Number 1 1.November
 measured as the angle between a line connecting the most medial aspects of the medial malleolus (A) and the navicular tubercle (B) and a line connecting the most medial")


5 FIGURE 3. Longitudinal arch angle (4) measured as the angle between a line connecting the most medial aspects of the medial malleolus (A) and the navicular tubercle (B) and a line connecting the most medial aspects of the navicular tubercle and the first metatarsal head (C). Each subject was then asked to stand barefoot on the treadmill in the standardized foot width position with the thermoplastic calcaneal mold in place. The calcaneal angle was measured with a goniometer and then video recorded for validation. Then, subjects donned their shoes without orthotics and assumed the standardized foot width position. The static calcaneal angle was measured again with a goniometer and video recorded. Next, subjects donned their shoes with their foot orthotics while the static standing calcaneal angle was again measured with a goniometer and video recording. TABLE 1. Subject characteristics for demographics, screening exam, orthotics, and shoes. Static Longicalca- tudneat inal Toe-out angle arch angle Motion Medial Medial Rein- Age Height (de- angle (de- control Orthotic Orthotic rearfoot forefoot forced Forefoot Subject Sex (years) (crn) Mass (ks) grees) (degrees) grees) shoes length stiffness post post arch varus 1 F No Full Semirigid No Yes No Yes 2 M Yes Full Semirigid No Yes No Yes 3 M No Full Semirigid No Yes No Yes 4 M Yes Full Semirigid No Yes No Yes 5 F Yes 314 Soft Yes Yes No Yes 6 M Yes 314 Soft Yes Yes Yes Yes 7 F Yes Full Semirigid No Yes No Yes 8 M Yes Full Semirigid No Yes No Yes 9 M Yes Full Semirigid No Yes No Yes 10 F Yes Full Semirigid No Yes No Yes 11 M Yes Full Semirigid No Yes No Yes 12 M Yes Full Semirigid No Yes No Yes 13 F No 314 Soft Yes No Yes No 668 J Orthop Sports P h p Ther.Volume SO. Number 1 1.November 2000
6 Toesut Angle ter of the camera lens was positioned 0.32 meters above the ground. The camera was adjusted and leveled so that the frontal plane of the subject was orthogonal to the optical axis of the camera. The field width was calibrated at 0.5 meters and focused by hand. A studio light was placed adjacent to the camera lens, and directed toward the subject. A black background curtain was placed in front of the treadmill. A linear reference was placed in the viewing field at the focal point of the treadmill and was video recorded before the testing. Testing Procedure FIGURE 4. Schematic of method used to estimate toe-out angle (PI. Toeout angle is measured as the acute angle between a line that bisects the forefoot and rearfoot of the right shoe print and a line that connects the most medial aspects of successive right heel prints. Mean toe-out angle for subjects was 7.7" (s = 4.8). Shoe Preparation Use of a foot orthotic adds weight to the lower extremity and may influence walking gait kinematics. Lead shot, equivalent to the difference in weight between the orthotic and a standard shoe insert, was placed around the external medial and lateral midse le of both shoes and secured with black duct tape. The tape was also placed over any reflective areas of the shoe. A piece of white tape was placed across the plantar surface of the outersole of the heel of the shoe to help identify heel off during the gait cycle. The tape was positioned as far as possible posterior on the outersole of the heel without being visible in the static standing position. Field Preparation The field was prepared to duplicate the field setup of Hirth.lJ The center of the camera lens was placed 4.3 meters from the focal point on the treadmill. The focal point was located centrally, 0.93 meters forward from the back edge of the treadmill. The cen- Each subject walked at a speed that brought their heart rate within 5 beats per minute of their aerobic training range for 5 minutes for each testing condition. The first subject, randomly selected, performed the first walking condition without orthotics. Subjects who followed alternated between orthotic and nonorthotic conditions as the first test condition to ensure equal representation of both possible testing orders. Video data were collected during the last minute of the &minute walking trial for the first test condition. Each subject then sat until their heart rate remained within 5 beats per minute of their resting heart rate for 5 minutes. The next test condition was conducted under the alternate test condition (ie, orthotic or nonorthotic) with all else remaining the same. Care was taken that the position of the thermoplastic marker and the shoe preparation were not altered when the subject changed the test condition. After completing the second trial, each subject removed their shoes and socks carefully and assumed the standardized foot width position on the treadmill for video recording with the calcaneal mold in place. This measurement of calcaneal angle was compared with previous barefoot measurements of calcaneal angle to assess whether the marker had moved relative to the subject's calcaneus during the testing. Data Reduction The Peak (version 5.3 software) automatic digitizing module was used to digitize the position of retroreflective markers on the 2 segments of the right leg. Each of the 5 separate static standing calcaneal angles recorded for measurement was digitized over 16 consecutive fields. The mean of the 16 angles was used for data analysis. Three of the static measures were barefoot standing calcaneal angles to ensure consistent retroreflective marker-thermoplastic mold position throughout the study. The remaining 2 static standing calcaneal angles were the orthotic and nonorthotic shoe condition measures which were used to assess the effects of shoewear and foot orthotics on static standing calcaneus to leg position. J Orthop Sports Php Ther.Volume SO. Number 1 1.November
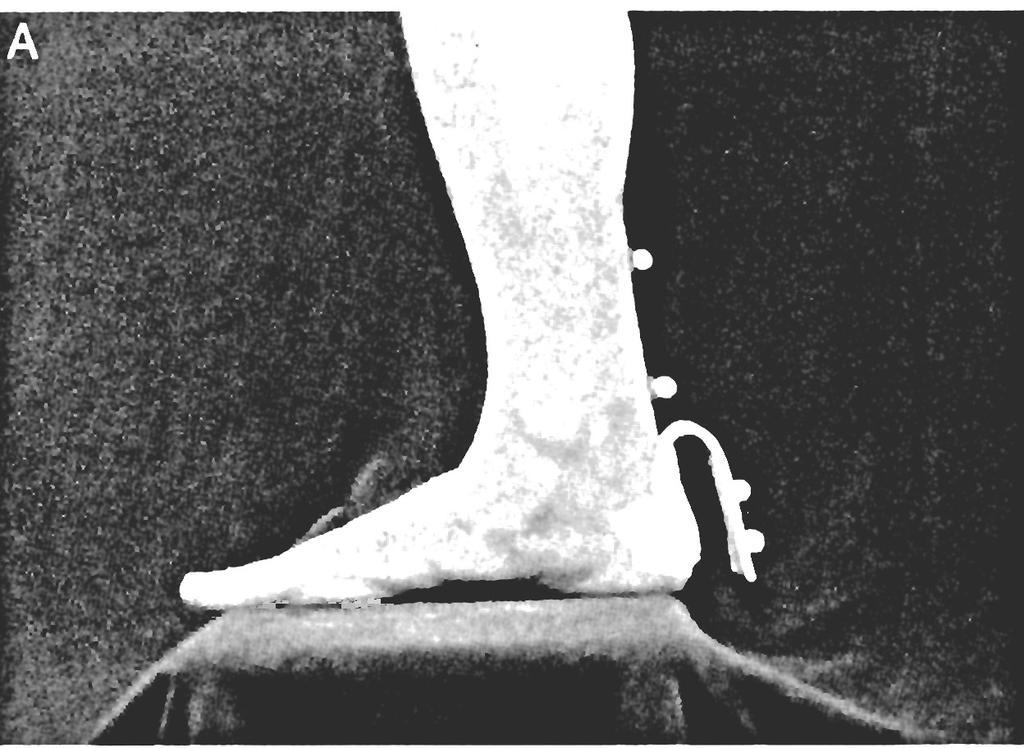






7 FIGURE 5. Thermoplastic marker applied to the calcaneus (A), with the shoe in place (B), and viewed posteriorly with shoe in place (C). 670 J Orthop Sports Phys Ther.Volume SO. Number 1 1.November 2000

8 Five gait cycles, 1 approximately every 10 seconds, were randomly selected from the 1-minute video records and analyzed to represent each subject's gait. Heel strike was the first field in which the outersole of the heel contacted the treadmill. Heel rise was the first field in which the white tape on the bottom of the heel became visible for the entire medial to lateral width of the shoe's outersole. Toe-off was identified to determine the duration of stance phase. Toeoff was recorded as the last field in which the shoe was in contact with the treadmill. Position data were not analyzed after heel rise to minimize measurement error attributable to out of plane Video data were sampled at 60 Hz and filtered with a Butterworth, low-pass, fourth order, zero lag filter. Based on pilot work, a cutoff frequency of 10 Hz was used for static and dynamic measures of the calcaneal angle. The mean values from the 5 gait cycles were computed for the maximum calcaneal eversion angle; calcaneal eversion angle at heel rise; stance phase duration; duration from heel strike to initiation of calcaneal inversion; and percent of stance phase at which initiation of calcaneal inversion occurred. Data Analysis Means and standard deviations were calculated for subjects' age, height, and weight by sex. Intraclass correlation coefficients (ICC [3,5]) were calculated for the 5 gait cycles for each condition to determine the between trial reliability of measuring the kinematic ~ariables.'~ Static standing analyses An intraclass correlation coefficient (ICC [3,1]) was used to determine consistency among the 3 static standing barefoot calcaneal angle measures: initial barefoot standing calcaneal angle without the thermoplastic mold, the pretest barefoot calcaneal angle with the mold, and the posttest barefoot calcaneal angle with the mold. This analysis was conducted using a 2-way ANOVA procedure (13 subjects X 3 times of measurement). A 1- way repeated measures ANOVA also was performed to determine any differences among the following pretest calcaneal static standing angles: barefoot with thermoplastic mold, shoes with thermoplastic mold and no orthotics, and shoes with orthotics and thermoplastic mold. A Tukey Honestly Significant Difference analysis was used for any post hoc comparison of cell means. Treadmill waking analyses Individual paired t tests compared the effects of orthotic and nonorthotic shoewear conditions for: maximum calcaneal eversion angle; calcaneal eversion angle at heeldf; duration of stance phase; duration of heel strike to initiation of calcaneal inversion; and percent stance phase for initiation of calcaneal inversion. A 1-tailed test with alpha of 0.05 was conducted for all dependent TABLE 2. lntraclass correlation coefficients (ICC) for reliability of dependent variables for nonorthotic and orthotic test conditions.* Nonor- or- Variable thotic thotic Peak calcaneal eversion angle Calcaneal eversion angle at heel rise Stance phase duration Time to the initiation of calcaneal inversion Percent of stance phase to the initiation of calcaneal inversion ICCs for kinematic variables are ICC version ICC (3,5), computed using a 2-way ANOVA procedure (13 subjects X 5 trials).24 variables for which the investigators hypothesized a decrease in magnitude effected by foot orthotics. We hypothesized that foot orthotics would effect a decrease in peak calcaneal eversion angle, calcaneal eversion angle at heel rise, time to initiation of calcaneal inversion, and percent of stance phase to the initiation of calcaneal inversion. A 2-tailed test (alpha = 0.05), however, was used for the duration of stance variable because the investigators did not establish an a priori direction for the effects of foot orthotics on this variable. RESULTS Eight men with a mean age of years, height of centimeters, and a mass of kilograms participated in the study. The 5 women who participated in the study had a mean age of years, a mean height of t 4.6 centimeters, and a mean mass of k i b grams. The mean for the static standing arch angle was t 4.5". Twelve subjects demonstrated a forefoot varus upon prone observation. Ten subjects wore full length semirigid orthoses. Two subjects wore three-fourths length soft orthoses and 1 subject wore three-fourths length rigid orthoses. Ten subjects wore shoes with pronation control features, as previously described. Subjects maintained an average heart rate of % of their calculated maximum age-predicted heart rate during the nonorthotic condition and % of maximum age-predicted heart rate for the orthotic condition. The demographic data for each subject, their screening exam results, and the shoe and orthotic characteristics for each subject are given in Table 1. The ICC values for reliability of the kinematic variables are listed in Table 2. All ICC values were equal to or greater than Means and standard deviaitions for the treadmill walking variables are provided in Table 3. Static Standing Results The subjects demonstrated a mean static standing calcaneal eversion angle of " for the bare- J Orthop Sports P h y Ther.Volume SO. Number 1 1. November
9 TABLE 3. Means (standard deviations) for heart rate and treadmill variables for orthotic and nonorthotic conditions.' Condition Variable Nonorthotic Orthotic t P Power Effect size Heart rate (bpm) (10.5) (9.7) Peak calcaneal eversion angle (degrees) 14.7 (6.6)t 12.5 (5.1) Calcaneal eversion angle atheel (se (degrees) 12.3 (6.0)t 10.2 (4.8) Stance time (seconds) 0.57 (0.05) 0.57 (0.05) Time to initiation of calcaneal inversion (seconds) (0.07) (0.06) Percent stance for calcaneal inversion initiation ( O h ) 28 (13) 25 (11) * Power analyses were conducted only for the nonsignificant results for the last 3 variables in the table. Means are based on data for 13 subjects (5 gait cycles for each subject). df = 12 for all contrasts. t Nonorthotic mean value significantly greater than orthotic value ( P < 0.05). foot condition with no marker in place; " for the pretest barefoot condition with thermoplastic mold in place; and " for the posttest barefoot condition with thermoplastic mold in place. The ICC value for consistency among the 3 measures of calcaneal eversion angle was ICC (3,l) = The mean calcaneal eversion angle with subjects standing in their shoes with the thermoplastic mold was ". The mean calcaneal eversion angle with subjects standing in their shoes with their orthotics in place and with the thermoplastic mold was ". The ANOVA results indicated significant differences among these means and the mean pretest barefoot standing value with the mold in place (F = 39.15; df = 2,24; P = ). A Tukey Honestly Significant Difference post hoc analysis indicated that the calcaneal eversion angle for barefoot standing was significantly ( P < 0.01) greater than the calcaneal eversion angles for the shoe and the shoe plus orthotic conditions. The calcaneal eversion angles for the 2 shoe conditions were not significantly different from each other. Figure 6 depicts static standing calcaneal eversion angles for the following calcaneal mold conditions: pretest barefoot; shoes without orthotics; and shoes with orthotics. Subject FIGURE 6. Effects of shoes and shoes with orthotics on static standing calcaneal eversion angle for the 13 study subjects. 0 = Barefoot; = Shoes; A = Shoes and Orthotics. A single measure is depicted for each subject in each condition. Treadmill Walking Results The results for the 5 gait variables indicated that foot orthotics caused a significant reduction (P < 0.05) in the peak calcaneal eversion angle and the calcaneal eversion angle at heel rise (Table 3). The mean reduction in peak calcaneal eversion angle was 2.2" and the mean reduction in calcaneal eversion angle at heel rise was 2.1". Foot orthotics had no significant effect on stance time, time to initiation of calcaneal inversion, and the percent stance time at which calcaneal inversion was initiated. A post hoc power analysis was conducted for these last 3 variables (Table 3). Using an effect size based on the study data and an alpha level of 0.05, the power to detect a statistically significant difference for these 3 variables varied from 0.07 to These results indicate that we were unable to detect a significant difference between orthotic and nonorthotic conditions for these 3 variables, if differences truly existed. DISCUSSION The mean calcaneal eversion angle of 15.5" during static standing for subjects in this study was greater than 2 standard deviations (>12") from the mean calcaneal eversion angle reported by Jonson and Gross.'"ubjects also demonstrated a longitudinal arch angle of 127.3". Our subjects, therefore, would be defined as pronators according to the classification system suggested by Jonson and Gross,'%nd would have been classified as severe pronators if the mean arch angle of the group had been one-third of 1" less. Ten of the 13 subjects in our study wore shoes with various pronation control features. The interaction of the orthotics used in this study with shoes having predominantly motion control features may have enhanced the effect of the orthotics across all study variables. The results of this study, therefore, may apply only to orthotic wearers who have moderate to severe pronation, and who wear shoes with pronation control features. We could not reach any conclusions about effects that might be attributed to 672 J Orthop Sports Phys Ther-Volume 3O.Number 1 1.November 2000
10 specific shoewear and foot orthotic characteristics because of the relatively low number of subjects. Subjects were asked to "walk quickly" over butcher paper so we could estimate each subject's preferred foot placement angle. We cannot guarantee that each subject's walking speed during this screening procedure matched their walking speed for their treadmill walking trials. No guarantee exists, either, that each subject's foot placement angle for over ground walking would have been the same as their foot placement angle for treadmill walking even if the 2 walking speeds were equivalent. Only the right foot of each subject was analyzed. Rogers and LeveauZ2 reported that foot orthotics significantly decreased pronation in runners, but for the left foot only. This suggests that foot orthotics may not have symmetric effects. This factor, coupled with the relatively small sample size, may also limit the generalizeability of the results. Additionally, data reduction in our study was limited to the percentage of stance phase before heel rise. Several subjects demonstrated their peak calcaneal eversion angle at heel rise. Peak calcaneal eversion may have actually occurred after heel rise for some of the subjects. As a result, the timing and value of the peak calcaneal eversion angle may have been underestimated for several subjects for the entirety of the stance phase. Our study was designed to provide information about the effects of foot orthotics on calcaneal kinematics for individuals who pronate excessively. No attempt was made to constrain shoe type or orthotic type so that the results might be more generalizeable to a clinical population. The ICCs for variability among trials for all test variables varied from 0.79 to 0.99 for orthotic and nonorthotic conditions. These data suggest acceptable reliability for the testing method. A limitation of our study, however, was the use of only one examiner for all measurements. No attempt was made to examine interrater reliability for the variables measured. Static Standing The ICC results suggest consistency among the 3 barefoot measures of calcaneal eversion angle. Consistency between the barefoot measurement without the marker and the 2 barefoot measures with the thermoplastic marker suggest that the thermoplastic marker provided valid measures of calcaneal eversion angle. Consistency between the barefoot calcaneal eversion angles with the thermoplastic marker before and after treadmill walking suggests that the thermoplastic marker remained welladhered to the calcaneus during the treadmill walking. We are unaware of other studies in which investigators have been able to monitor reliably calcaneal position inside the shoe without altering the physical appearance of the shoe and possibly the mechanical characteristics of the shoe. Considerable effort was required to remove the calcaneal mold after testing, except for 1 subject who demonstrated hyperhydrosis. This suggests that the mold was rigidly fixed to each subject's calcaneus during the testing procedures. However, the possibility does exist that the shoe produced movement of the thermoplastic marker relative to the calcaneus during the dynamic walking trials. The static calcaneal eversion angle when the sub jects stood barefoot was significantly greater than the calcaneal eversion angle for standing with shoes alone or standing with shoes and orthotics. There was no significant difference between the static calcaneal to leg angle with shoes alone and with shoes plus orthotics. These "static" findings may not be generalized to dynamic conditions. Bates et al,' however, reported similar results for dynamic running gait "... with greater changes having occurred between the barefoot condition and the other two (shoe and shoe with orthotic) conditions." l(pm2) These findings indicate that shoes alone may have a significant effect in reducing the calcaneal eversion angle both statically and dynamically. Our results indicate that motion control shoes effectively reduce certain measures of pronation. Clinical experience suggests that many individuals with abnormal pronation report musculoskeletal complaints with p r e longed standing and that these complaints diminish with interventions designed to reduce excessive pronation, such as shoewear, orthotics, or both. Treadmill Walking Foot orthotics significantly reduced the mean peak calcaneal eversion angle by 2.2" (Table 3) during fast treadmill walking for the subjects in this study. This result confirms the ability of foot orthotic devices to restrict the magnitude of total pronation during fast walking. The reduction in peak calcaneal eversion in our study is less than the 4.3"-reduction reported by Novick and K e l l e ~ McCulloch. ~ ~ et all7 reported a reduction in the peak calcaneal eversion angle of 4.0 and 2.7" for walking velocities of 0.9 and 1.3 m/s, respectively. The predominance of rigid orthoses used by subjects in the Novick and Kelley study and by subjects in the McCulloch et a1 study may explain the greater reductions in the magnitude of calcaneal eversion because a rigid orthosis may impose more resistance to calcaneal motion than the semirigid orthotics used by most of our subjects. The average walking speed for subjects in the present study was 1.9 m/s, which was appreciably faster than the walking speed of subjects in the studies by Novick and Kelley and by McCulloch et al, and may have also had an effect on the magnitude of the calcaneal eversion angle during walking. Finally, a normalization procedure was described by Novick and Kelley,2O and later used by McCulloch J Orthop Sports Phys Ther-Volume SO. Number 1 1. November 2000
11 et al,17 in which to "more accurately represent the position of the calcaneus inside the shoe,... markers were placed on the posterior heel counter at the same angle as in weight-bearing, barefoot, [and] resting stance." 20(pS04) The investigators then measured the calcaneal eversion angle's of the subjects as they stood barefoot on their orthotics. The researchers subtracted the barefoot on orthotic calcaneal angle from the barefoot alone calcaneal angle and defined this angular value as the static normalization value. This value was then subtracted from all angular measures involving the calcaneus during the dynamic orthotic condition trials. This procedure essentially guarantees a difference, in the amount of the normalization value, between nonorthotic and orthotic conditions. In recognizing the problems with considering motion of the shoe heel counter as representative of motion of the heel, these researchers made several questionable assumptions. They assumed that the shoe would have no effect on the static calcaneal angle and that the shoe would not interact significantly with the orthotic to affect the calcaneal angle. They also assumed that a statically derived normalization value can be applied universally across dynamic walking conditions. The results of our study indicate that foot orthotics caused a statistically significant reduction of 2.1" in the calcaneal eversion angle at heel rise (Table 3). This variable has been suggested as an indicator of the timing of pronation during stance phase. Pronation at inappropriate times in the gait cycle has been suggested as more problematic than the total magnitude of pr~nation.~." The normal calcaneus inverts during supination at heel rise to position the foot for propulsion. By reducing the calcaneal eversion angle at heel rise, a foot orthotic causes the foot to become relatively more supinated, or rigid, during propulsion. This effect may reduce the incidence of pathologies associated with forward propulsion on a hypermobile, pronated foot. McCulloch et all7 reported foot orthotics caused a 4.0" reduction in the angle of calcaneal eversion at heel rise among the 10 subjects in their study. Again, the predominance of rigid orthoses, differences in walking speed, and a normalization procedure may explain the larger magnitude reductions in calcaneal eversion reported by these researchers, compared with our results. We are unable to say with certainty that the 2.2" reduction of peak calcaneal eversion and the 2.1" reduction in calcaneal eversion angle at heel rise are clinically significant for the foot orthotics used in our study. We can report that before this study, each of the 13 subjects had received foot orthotics as treatment for a lower quarter musculoskeletal complaint. In each instance, the foot orthotic intervention either diminished or eliminated symptoms associated with each subject's musculoskeletal complaint, and all subjects reported being pain free at the time of this study. Foot orthotics had no statistically significant effect on stance time, time to initiation of calcaneal inversion, or percent of stance time for the initiation of calcaneal inversion. McCulloch et all7 reported that foot orthotics caused an increase in the period from maximum calcaneal eversion to heel rise. The measurement of time to initiation of calcaneal inversion in our study is a different variable than the period from maximum calcaneal eversion to heel rise in the McCulloch et al study.i7 Both measures assess the timing of pronation in stance. The time at which maximum calcaneal eversion first occurs, however, is not necessarily the time at which initiation of calcaneal inversion occurs. Once at maximum calcaneal eversion, the foot may remain at that position for an unknown time period before beginning motion towards calcaneal inversion. This difference in referencing the relative timing of maximum calcaneal eversion during stance does not permit direct comparisons between our results and those of McCulloch et al.17 The use of primarily rigid foot orthotics by McCulloch's subjects also may have had a greater effect in limiting pronation so that maximum calcaneal eversion occurred earlier in stance phase than it did in our subjects. This result would effectively increase the time between maximum calcaneal eversion and heel rise. The predominantly semirigid foot orthotics used in our study may have been less effective in reducing maximum calcaneal eversion. Additionally, 12 of our 13 subjects demonstrated a forefoot varus malalignment, which may increase the complexity of a pronation If subjects in previous studies demonstrated a predominance of calcaneal dysfunction, or if they were less severe pronators than our subjects, then orthotic correction at the rearfoot may have more effectively decreased the eversion time during stance for the subjects in the previous studies. These factors may explain the foot orthotics nonsignificant effect on the time to initiation of inversion in our study. Our results also indicate no significant difference in the total duration of stance phase between orthotic and nonorthotic conditions. There was no difference, therefore, between conditions with regard to the percentage of stance time at which the initiation of calcaneal inversion motion occurs since this variable is a function of the values for stance time and time to initiation of calcaneal inversion. The results of the power analysis indicated an inability to detect a difference in the shoe plus orthotic and shoe alone conditions for stance duration time and the 2 variables related to initiation of calcaneal inversion. Factors such as small sample size and between subject variability may have contributed to the relatively low power values. 674 J Orthop Sports Phys Ther.Volume SO. Number 1 1.November 2000
12 Clinical Implications The results o f this study may only be generalizeable to patients who are moderate to severe pronators and who use foot orthotics with motion control shoes during fast walking. Foot orthotics decreased the maximum calcaneal eversion angle and the calcaneal eversion angle at heel rise. The reduction in both cases was slightly more than 2". While this reduction appears small in magnitude, clinical experience suggests that slight modifications in the weightbearing relationship between the foot and the ground are often associated with a reduction, o r the complete elimination, o f clinical symptoms o f foot o r lower extremity pathology. Another clinically significant result was the difference in the static standing calcaneal eversion angle between the barefoot and shoe conditions. The results suggest that shoes with motion control features may significantly reduce the static standing calcaneal eversion angle. Other researchers have demonstrated similar results under dynamic conditions.' Patients often are offered orthotics before their shoes are evaluated for motion control features. Orthotics also may be judged as ineffective in instances in which the patient's shoes have not been evaluated. Clinicians, therefore, should consider having patients use appropriate shoes before prescribing orthotics. Clinicians also should consider the possible interaction between structural characteristics o f shoes and foot orthoses. CONCLUSIONS The results o f this study indicate that foot orthotics cause a significant reduction in maximum calcaneal eversion and calcaneal eversion at heel rise during treadmill walking for subjects with abnormal pronation. Shoes with a variety o f motion control features, as well as the same shoes with foot orthotics, significantly reduced the static standing calcaneal eversion angle. REFERENCES 1. Bates BT, Osternig LR, Mason MS, James LS. Foot orthotic devices to modify selected aspects of lower extremity mechanics. Am / Sports Med. 1979;71: Blake RL, Denton JA. Functional foot orthoses for athletic injuries. 1 Am Pod Med Assoc. 1985;75: Blake RL, Ferguson H. Foot orthosis for the severe flatfoot in sports. / Am Pod Mec Assoc ;81: Brown LP, Yavorsky BS. Locomotor biomechanics and pathomechanics. / Orthop Sports Phys Ther. 1987;9: Cornwall MW, McPoil TG. Reducing 2-dimensional calcaneal motion variability during walking. / Am Podiatr ASSOC. 1993;83: Dahle LK, Mueller M, Delitto A, Diamond JE. Visual assessment of foot type and relationship of foot type to lower extremity injury. / Orthop ~ p o r t s ' ~ h The'r.' ~ s 1991;14: Donatelli R, Hurlbert C, Conaway D, St Pierre R. Biomechanical foot orthotics: A retrospective study. / Orthop Sports Phys Ther. 1988;10: Donatelli R. Abnormal biomechanics of the foot and ankle. / Orthop Sports Phys Ther. 1987;9: Fox SM, Naughton JP, Gorman PA. Physical activity and cardiovascular health II. The exercise prescription: intensity and duration. Mod Concepts Cardiovasc Dis. 1972;16: Glaves A. The accuracy of P e a P two and three dimensional videography analysis for a calcaneal model Ithesisl. Chapel Hill, NC: University of North Carolina at Chapel Hill; Gross ML, Davlin LB, Evanski PM. Effectiveness of orthotic shoe inserts in the long-distance runner. Am / Sports Med. l991;19: Gross MT. Lower quarter screening for skeletal malalignment--suggestions for orthotics and shoewear. / Orthop Sports Phys Ther. 1 9%;2 1 : Hirth CJ. Accuracy of the Peak@ two-dimensional videography analysis for a calcaneal model during overground and treadmill locomotion [thesis]. Chapel Hill, NC: University of North Carolina at Chapel Hill; Hughes L. Biomechanical analysis of the foot and ankle for predisposition to developing stress fractures. / Orthop Sports Phys Ther. 1985;7: Johanson MA, Donatelli R, Wooden MJ, Andrew PD, Cummings GS. Effects of three different posting methods on controlling abnormal subtalar pronation. Phys Ther. 1994;74: Jonson SR, Gross MT. lntraexaminer reliability, interexaminer reliability, and normal values for nine lower extremity skeletal measures. / Orthop Sports Phys Thec 1997;25: McCulloch MU, Brunt D, Vander Linden D. The effect of foot orthotics and gait velocity on lower limb kinematics and temporal events of stance. / Orthop Sports Phys Ther. 1993;17: McPoil TG. Footwear. Phys Ther. 1988;68: McPoil TG, Knecht HG, Schuit D. A survey of foot types in normal females between the ages of 18 and 30 years. / Orthop Sports Phys Ther. 1988;9: Novick A, Kelley DL. Position and movement changes of the foot with orthotic intervention during the loading response of gait. / Orthop Sports Phys Ther. 1990; 1 1 : Polinsky KL. The effects of running shoe and marker system on calcaneal kinematics in runners [thesis]. Chapel Hill, NC: University of North Carolina at Chapel Hill; Rodgers M, LeVeau B. Effectiveness of foot orthotic devices used to modify pronation in runners. / Orthop Sports Phys Ther. 1982;4: Root ML, Orien WP, Weed JH. Clinical Biomechanics. Normal and Abnormal Function of the Foot. Vol II. Los Angeles, Calif: Clinical Biomechanics Corporation; Schrout PE, Fleiss JL. lntraclass correlations: uses in assessing rater reliability. Psych Bull. 1979;86: Smith LS, Clarke TE, Hamill CL, Santopeitro F. The effects of soft and semi-rigid orthoses upon calcaneal movement in running. Pod Sports Med. 1986;76: Subotnick SI. Biomechanics of the subtalar and midtarsal joints. / Am Pod Assoc. 1975;65: Tiberio D. Pathomechanics of structural foot deformities. Phys Ther. 1988;68: Tiberio D. The effect of excessive subtalar joint pronation on patellfemoral mechanics: a theoretical model. / Orthop Sports Phys Ther. 1987;9: J Orthop Sports Phys Ther-Volume SO. Number 11. November 2000
New research that enhances our knowledge of foot mechanics as well as the effect of
 The Tissue Stress Model: Justification based on Current Best Evidence New research that enhances our knowledge of foot mechanics as well as the effect of bone alignment on foot mobility during activity
The Tissue Stress Model: Justification based on Current Best Evidence New research that enhances our knowledge of foot mechanics as well as the effect of bone alignment on foot mobility during activity
EFFECT OF ORTHOTICS AND FOOTWEAR ON STATIC
 Journal of Sports Science and Medicine (2006) 5, 466-472 http://www.jssm.org Young investigator Research article EFFECT OF ORTHOTICS AND FOOTWEAR ON STATIC REARFOOT KINEMATICS Molly Winkelmeyer 1, Brita
Journal of Sports Science and Medicine (2006) 5, 466-472 http://www.jssm.org Young investigator Research article EFFECT OF ORTHOTICS AND FOOTWEAR ON STATIC REARFOOT KINEMATICS Molly Winkelmeyer 1, Brita
Longitudinal Arch Angle (LAA): Inter-rater reliability comparing Relaxed Calcaneal Stance with Toe Off
: Inter-rater reliability comparing Relaxed Calcaneal Stance with Toe Off") The Foot and Ankle Online Journal Official Publication of the International Foot & Ankle Foundation faoj.org / ISSN 1941-6806 Longitudinal Arch Angle (LAA): Inter-rater reliability comparing Relaxed Calcaneal
The Foot and Ankle Online Journal Official Publication of the International Foot & Ankle Foundation faoj.org / ISSN 1941-6806 Longitudinal Arch Angle (LAA): Inter-rater reliability comparing Relaxed Calcaneal
Ankle biomechanics demonstrates excessive and prolonged time to peak rearfoot eversion (see Foot Complex graph). We would not necessarily expect
. We would not necessarily expect") Case Study #1 The first case study is a runner presenting with bilateral shin splints with pain and tenderness along the medial aspect of the tibia. The symptoms have increased significantly over the last
Case Study #1 The first case study is a runner presenting with bilateral shin splints with pain and tenderness along the medial aspect of the tibia. The symptoms have increased significantly over the last
Recent Advances in Orthotic Therapy for. Plantar Fasciitis. An Evidence Based Approach. Lawrence Z. Huppin, D.P.M.
 Recent Advances in Orthotic Therapy for Plantar Fasciitis An Evidence Based Approach Lawrence Z. Huppin, D.P.M. Assistant Clinical Professor, Western University of Health Sciences, College of Podiatric
Recent Advances in Orthotic Therapy for Plantar Fasciitis An Evidence Based Approach Lawrence Z. Huppin, D.P.M. Assistant Clinical Professor, Western University of Health Sciences, College of Podiatric
SECTION 4 - POSITIVE CASTING
 4-1 SECTION 4 - POSITIVE CASTING THE SHAPE OF THE SHELL IS DERIVED FROM THE SHAPE OF THE CAST Thermo-forming plastic for orthopedic intervention was originally developed at the University of California
4-1 SECTION 4 - POSITIVE CASTING THE SHAPE OF THE SHELL IS DERIVED FROM THE SHAPE OF THE CAST Thermo-forming plastic for orthopedic intervention was originally developed at the University of California
Smita Rao PT PhD. Judith F. Baumhauer MD Josh Tome MS Deborah A. Nawoczenski PT PhD
 Smita Rao PT PhD Judith F. Baumhauer MD Josh Tome MS Deborah A. Nawoczenski PT PhD Strong Foot and Ankle Institute Department of Orthopaedics University of Rochester Rochester, NY Center for Foot and Ankle
Smita Rao PT PhD Judith F. Baumhauer MD Josh Tome MS Deborah A. Nawoczenski PT PhD Strong Foot and Ankle Institute Department of Orthopaedics University of Rochester Rochester, NY Center for Foot and Ankle
The relationship between the structure of the foot and its
 The Relationship Between Forefoot, Midfoot, and Rearfoot Static Alignment in Pain-Free Individuals Kirsten Rossner Buchanan, PT, PhD, ATC 1 Irene Davis, PT, PhD 2 Journal of Orthopaedic & Sports Physical
The Relationship Between Forefoot, Midfoot, and Rearfoot Static Alignment in Pain-Free Individuals Kirsten Rossner Buchanan, PT, PhD, ATC 1 Irene Davis, PT, PhD 2 Journal of Orthopaedic & Sports Physical
Effectiveness of Foot Orthotic Devices Used to Modify Pronation in Runners*
 0196-6011 /82/0402-0086$02.00/0 THE JOURNAL OF ORTHOPAEDIC AND SPORTS PHYSICAL THERAPY Copyright O 1982 by The Orthopaedic and Sports Physical Therapy Sections of the American Physical Therapy Association
0196-6011 /82/0402-0086$02.00/0 THE JOURNAL OF ORTHOPAEDIC AND SPORTS PHYSICAL THERAPY Copyright O 1982 by The Orthopaedic and Sports Physical Therapy Sections of the American Physical Therapy Association
Custom Ankle Foot Orthoses
 A Comparison of Negative Casting Techniques Used for the Fabrication of Custom Ankle Foot Orthoses How you cast makes a big difference in correctly capturing an impression foot. By Doug Richie DPM and
A Comparison of Negative Casting Techniques Used for the Fabrication of Custom Ankle Foot Orthoses How you cast makes a big difference in correctly capturing an impression foot. By Doug Richie DPM and
ATHLETES AND ORTHOTICS. January 29, 2014
 ATHLETES AND ORTHOTICS January 29, 2014 TOPICS TO COVER TODAY Why use an orthotic? What athlete would benefit from wearing orthotics? What device should I use: Custom versus off of the shelf orthotics?
ATHLETES AND ORTHOTICS January 29, 2014 TOPICS TO COVER TODAY Why use an orthotic? What athlete would benefit from wearing orthotics? What device should I use: Custom versus off of the shelf orthotics?
Normal Gait and Dynamic Function purpose of the foot in ambulation. Normal Gait and Dynamic Function purpose of the foot in ambulation
 Normal Gait and Dynamic Function purpose of the foot in ambulation Edward P. Mulligan, PT, DPT, OCS, SCS, ATC Assistant Professor; Residency Chair UT Southwestern School of Health Professions Department
Normal Gait and Dynamic Function purpose of the foot in ambulation Edward P. Mulligan, PT, DPT, OCS, SCS, ATC Assistant Professor; Residency Chair UT Southwestern School of Health Professions Department
Effect of Ankle Dorsiflexion Range of Motion on Rearfoot Motion During Walking
 Effect of Ankle Dorsiflexion Range of Motion on Rearfoot Motion During Walking MARK W. CORNWALL, PhD, PT, CPed* THOMAS G. McPOIL, PhD, PT, ATC* The purpose of this study was to investigate whether the
Effect of Ankle Dorsiflexion Range of Motion on Rearfoot Motion During Walking MARK W. CORNWALL, PhD, PT, CPed* THOMAS G. McPOIL, PhD, PT, ATC* The purpose of this study was to investigate whether the
The Problem. An Innovative Approach to the Injured Runner. Dosage. Mechanics. Structure! Postural Observations. Lower Quarter Assessment
 The Problem An Innovative Approach to the Injured Runner Irene S. Davis, PhD, PT, FAPTA, FACSM Director, Spaulding National Running Center Harvard Medical School Healthy People 2020 Initiative 76% runners
The Problem An Innovative Approach to the Injured Runner Irene S. Davis, PhD, PT, FAPTA, FACSM Director, Spaulding National Running Center Harvard Medical School Healthy People 2020 Initiative 76% runners
Giovanni Alfonso Borelli Father of Biomechanics
 Giovanni Alfonso Borelli Father of Biomechanics 1608-1679 Peter Guy BSc DCh Private practice Whitby and Peterborough Professor Chiropody Faculty Michener Institute of Education at UHN Advisory Board Member
Giovanni Alfonso Borelli Father of Biomechanics 1608-1679 Peter Guy BSc DCh Private practice Whitby and Peterborough Professor Chiropody Faculty Michener Institute of Education at UHN Advisory Board Member
The Effects of Vacuum-Molded Orthotics on Lower Extremity Overuse Injuries
 Journal of Sport Rehabilifation, 1993, 2, 251-260 0 1993 Human Kinetics Publishers. Inc. The Effects of Vacuum-Molded Orthotics on Lower Extremity Overuse Injuries Matthew P. Callahan, Craig R. Denegar,
Journal of Sport Rehabilifation, 1993, 2, 251-260 0 1993 Human Kinetics Publishers. Inc. The Effects of Vacuum-Molded Orthotics on Lower Extremity Overuse Injuries Matthew P. Callahan, Craig R. Denegar,
ASSESMENT Introduction REPORTS Running Reports Walking Reports Written Report
 ASSESMENT REPORTS Introduction Left panel Avatar Playback Right Panel Patient Gait Parameters Report Tab Click on parameter to view avatar at that point in time 2 Introduction Software will compare gait
ASSESMENT REPORTS Introduction Left panel Avatar Playback Right Panel Patient Gait Parameters Report Tab Click on parameter to view avatar at that point in time 2 Introduction Software will compare gait
THE ANKLE-HIP TRANSVERSE PLANE COUPLING DURING THE STANCE PHASE OF NORMAL WALKING
 THE ANKLE-HIP TRANSVERSE PLANE COUPLING DURING THE STANCE PHASE OF NORMAL WALKING Thales R. Souza, Rafael Z. Pinto, Renato G. Trede, Nadja C. Pereira, Renata N. Kirkwood and Sérgio T. Fonseca. Movement
THE ANKLE-HIP TRANSVERSE PLANE COUPLING DURING THE STANCE PHASE OF NORMAL WALKING Thales R. Souza, Rafael Z. Pinto, Renato G. Trede, Nadja C. Pereira, Renata N. Kirkwood and Sérgio T. Fonseca. Movement
IJSPT ORIGINAL RESEARCH ABSTRACT
 IJSPT ORIGINAL RESEARCH THE USE OF A STATIC MEASURE TO PREDICT FOOT POSTURE AT MIDSUPPORT DURING RUNNING Michael B. Bade, PT, DPT, PhD 1 Timothy L. Chi, SPT 1 Kelly C. Farrell, SPT 1 Amanda J. Gresl, SPT
IJSPT ORIGINAL RESEARCH THE USE OF A STATIC MEASURE TO PREDICT FOOT POSTURE AT MIDSUPPORT DURING RUNNING Michael B. Bade, PT, DPT, PhD 1 Timothy L. Chi, SPT 1 Kelly C. Farrell, SPT 1 Amanda J. Gresl, SPT
Foot Biomechanics Getting Back to the Base
 Foot Biomechanics Getting Back to the Base Christopher J. Mehallo, D.O. Rothman Institute Orthopaedics Objectives Understand basic foot biomechanics during walking and running Understand common sports
Foot Biomechanics Getting Back to the Base Christopher J. Mehallo, D.O. Rothman Institute Orthopaedics Objectives Understand basic foot biomechanics during walking and running Understand common sports
The scientific basis for the use of biomechanical foot
 Br J Sp Med 1994; 28(3) The scientific basis for the use of biomechanical foot orthoses in the treatment of lower limb sports injuries - a review of the literature Timothy E. Kilmartin MChS FPodA and W.
Br J Sp Med 1994; 28(3) The scientific basis for the use of biomechanical foot orthoses in the treatment of lower limb sports injuries - a review of the literature Timothy E. Kilmartin MChS FPodA and W.
Foot mechanics & implications on training, posture and movement
 Foot mechanics & implications on training, posture and movement Three Arches Three Arches These arches are not reciprocal. When the foot pronates ALL arches should fall. If the medial arch falls and the
Foot mechanics & implications on training, posture and movement Three Arches Three Arches These arches are not reciprocal. When the foot pronates ALL arches should fall. If the medial arch falls and the
Research Report. Measurements Used to Characterize the Foot and the Medial Longitudinal Arch: Reliability and Validity. Key Words:
 Research Report Measurements Used to Characterize the Foot and the Medial Longitudinal Arch: Reliability and Validity Background and Purpose. Abnormality in the structure of the medial longitudinal arch
Research Report Measurements Used to Characterize the Foot and the Medial Longitudinal Arch: Reliability and Validity Background and Purpose. Abnormality in the structure of the medial longitudinal arch
Shin Splints and Forefoot Contact Running: A Case Report
 Shin Splints and Forefoot Contact Running: A Case Report Michael 1. Cibulka, MHS, PT, OCS' David R. Sinacore, PhD, PTZ Michael 1. Mueller, PhD, PT3 Copyright 1994. All rights reserved. S hin splints are
Shin Splints and Forefoot Contact Running: A Case Report Michael 1. Cibulka, MHS, PT, OCS' David R. Sinacore, PhD, PTZ Michael 1. Mueller, PhD, PT3 Copyright 1994. All rights reserved. S hin splints are
Dynamix Ankle Foot Orthoses Range
 The Restyled Dynamix Ankle Foot Orthoses Range Supporting your wellbeing Product Range Introduction Index Product Range Introduction... 3 Puffin - Dynamix Supramalleolar... 4 Penguin - Dynamix Plantarflexion...
The Restyled Dynamix Ankle Foot Orthoses Range Supporting your wellbeing Product Range Introduction Index Product Range Introduction... 3 Puffin - Dynamix Supramalleolar... 4 Penguin - Dynamix Plantarflexion...
Steffen Willwacher, Katina Fischer, Gert Peter Brüggemann Institute of Biomechanics and Orthopaedics, German Sport University, Cologne, Germany
 P01-3 ID126 SURFACE STIFFNESS AFFECTS JOINT LOADING IN RUNNING Steffen Willwacher, Katina Fischer, Gert Peter Brüggemann Institute of Biomechanics and Orthopaedics, German Sport University, Cologne, Germany
P01-3 ID126 SURFACE STIFFNESS AFFECTS JOINT LOADING IN RUNNING Steffen Willwacher, Katina Fischer, Gert Peter Brüggemann Institute of Biomechanics and Orthopaedics, German Sport University, Cologne, Germany
Treating Foot Pain in Alpine Skiers with
 SPORTS PODIATry Treating Foot Pain in Alpine Skiers with Pes Planus What role should the podiatrist play? 103 By Lawrence Z. Huppin, DPM and Paul R. Scherer, DPM Jakub Gojda Dreamstime The foot plays a
SPORTS PODIATry Treating Foot Pain in Alpine Skiers with Pes Planus What role should the podiatrist play? 103 By Lawrence Z. Huppin, DPM and Paul R. Scherer, DPM Jakub Gojda Dreamstime The foot plays a
Case Report: The Infant Flatfoot
 Sergio Puigcerver (1) ; Juan Carlos González (1) ; Roser Part (1) ; Eduardo Brau (1) ; Luis Ramón Mollá (2) (1) Instituto de Biomecánica de Valencia, UPV. Valencia, Spain; ibv@ibv.upv.es ; www.ibv.org
Sergio Puigcerver (1) ; Juan Carlos González (1) ; Roser Part (1) ; Eduardo Brau (1) ; Luis Ramón Mollá (2) (1) Instituto de Biomecánica de Valencia, UPV. Valencia, Spain; ibv@ibv.upv.es ; www.ibv.org
PATHOLOGICAL CONDITIONS REQUIRING THE USE OF CUSTOMIZED LASTS
 ICAMS 2014 5 th International Conference on Advanced Materials and Systems PATHOLOGICAL CONDITIONS REQUIRING THE USE OF CUSTOMIZED LASTS DANIEL PETCU, GHEORGHE BERIJAN INCDTP Division: Leather and Footwear
ICAMS 2014 5 th International Conference on Advanced Materials and Systems PATHOLOGICAL CONDITIONS REQUIRING THE USE OF CUSTOMIZED LASTS DANIEL PETCU, GHEORGHE BERIJAN INCDTP Division: Leather and Footwear
Case Study: Chronic Plantar Heel Pain/Plantar Fasciopathy. CASE STUDY PRESENTATION by Resonance Podiatry and Gait Labs
 Case Study: Chronic Plantar Heel Pain/Plantar Fasciopathy CASE STUDY PRESENTATION by Resonance Podiatry and Gait Labs THE PATIENT 43yo female, professional netball umpire 6 month history right plantar
Case Study: Chronic Plantar Heel Pain/Plantar Fasciopathy CASE STUDY PRESENTATION by Resonance Podiatry and Gait Labs THE PATIENT 43yo female, professional netball umpire 6 month history right plantar
As a physiotherapist I see many runners in my practice,
 When rubber meets road Mark Richardson reveals the story that our running shoes can tell us, and how it can help you avoid running injury at a glance This article: Shows you how to analyse the sole of
When rubber meets road Mark Richardson reveals the story that our running shoes can tell us, and how it can help you avoid running injury at a glance This article: Shows you how to analyse the sole of
A comparison of semi-custom and custom foot orthotic devices in high- and low-arched individuals during walking
 Available online at www.sciencedirect.com Clinical Biomechanics 23 (2008) 1287 1293 www.elsevier.com/locate/clinbiomech A comparison of semi-custom and custom foot orthotic devices in high- and low-arched
Available online at www.sciencedirect.com Clinical Biomechanics 23 (2008) 1287 1293 www.elsevier.com/locate/clinbiomech A comparison of semi-custom and custom foot orthotic devices in high- and low-arched
The Influence of Load Carrying Modes on Gait variables of Healthy Indian Women
 The Influence of Load Carrying Modes on Gait variables of Healthy Indian Women *Guha Thakurta A, Iqbal R and De A National Institute of Industrial Engineering, Powai, Vihar Lake, Mumbai-400087, India,
The Influence of Load Carrying Modes on Gait variables of Healthy Indian Women *Guha Thakurta A, Iqbal R and De A National Institute of Industrial Engineering, Powai, Vihar Lake, Mumbai-400087, India,
Purpose. Outline. Angle definition. Objectives:
 Disclosure Information AACPDM 69 th Annual Meeting October 21-24, 2015 Speaker Names: Sylvia Õunpuu, MSc and Kristan Pierz, MD Gait Analysis Data Interpretation: Understanding Kinematic Relationships Within
Disclosure Information AACPDM 69 th Annual Meeting October 21-24, 2015 Speaker Names: Sylvia Õunpuu, MSc and Kristan Pierz, MD Gait Analysis Data Interpretation: Understanding Kinematic Relationships Within
PLANTAR FASCIITIS. Points of Confusion. TREATING SUBCALCANEAL PAIN: Who gets the best outcomes?
 TREATING SUBCALCANEAL PAIN: Who gets the best outcomes? DOUGLAS H. RICHIE, JR., D.P.M. Seal Beach, California Points of Confusion Pathomechanics of Plantar Fascia overload: Foot Pronation STJ Pronation
TREATING SUBCALCANEAL PAIN: Who gets the best outcomes? DOUGLAS H. RICHIE, JR., D.P.M. Seal Beach, California Points of Confusion Pathomechanics of Plantar Fascia overload: Foot Pronation STJ Pronation
AllPro Foot. Posterior Mount Product Manual
 AllPro Foot Posterior Mount Product Manual Instructions The AllPro PM foot system has been designed and manufactured for specific patient weights. Failure to follow the weight guidelines and/or overload
AllPro Foot Posterior Mount Product Manual Instructions The AllPro PM foot system has been designed and manufactured for specific patient weights. Failure to follow the weight guidelines and/or overload
Impact of heel position on leg muscles during walking
 Original article Niigata Journal of Health and Welfare Vol. 14, No. 1 Impact of heel position on leg muscles during walking Koichi Akaishi Graduate School of Health and Welfare, Niigata University of Health
Original article Niigata Journal of Health and Welfare Vol. 14, No. 1 Impact of heel position on leg muscles during walking Koichi Akaishi Graduate School of Health and Welfare, Niigata University of Health
RUNNING SHOE STIFFNESS: THE EFFECT ON WALKING GAIT
 RUNNING SHOE STIFFNESS: THE EFFECT ON WALKING GAIT Stephen N Stanley, Peter J M c Nair, Angela G Walker, & Robert N Marshall Auckland Institute of Technology, Auckland, New Zealand University of Auckland,
RUNNING SHOE STIFFNESS: THE EFFECT ON WALKING GAIT Stephen N Stanley, Peter J M c Nair, Angela G Walker, & Robert N Marshall Auckland Institute of Technology, Auckland, New Zealand University of Auckland,
The importance of physical activity throughout an individual's life is indisputable. As healthcare
 What to Expect When They re Expecting: A Look at Biomechanical Changes in Walking/Running During Pregnancy Jennifer Bruer-Vandeweert, Megan Hotchkiss, Jamie Kronenberg, Kristin Olson Dr. Rumit Singh Kakar,
What to Expect When They re Expecting: A Look at Biomechanical Changes in Walking/Running During Pregnancy Jennifer Bruer-Vandeweert, Megan Hotchkiss, Jamie Kronenberg, Kristin Olson Dr. Rumit Singh Kakar,
THE EFFECTS OF TWO ARCH TAPING TECHNIQUES ON NAVICULAR HEIGHT AND PLANTAR PRESSURES THROUGHOUT EXERCISE. Tim Newell
 THE EFFECTS OF TWO ARCH TAPING TECHNIQUES ON NAVICULAR HEIGHT AND PLANTAR PRESSURES THROUGHOUT EXERCISE Tim Newell Submitted to the faculty of the University Graduate School in partial fulfillment of the
THE EFFECTS OF TWO ARCH TAPING TECHNIQUES ON NAVICULAR HEIGHT AND PLANTAR PRESSURES THROUGHOUT EXERCISE Tim Newell Submitted to the faculty of the University Graduate School in partial fulfillment of the
video Outline Pre-requisites of Typical Gait Case Studies Case 1 L5 Myelomeningocele Case 1 L5 Myelomeningocele
 Outline Evaluation of Orthosis Function in Children with Neuromuscular Disorders Using Motion Analysis Outcomes Terminology Methods Typically developing Case examples variety of pathologies Sylvia Õunpuu,
Outline Evaluation of Orthosis Function in Children with Neuromuscular Disorders Using Motion Analysis Outcomes Terminology Methods Typically developing Case examples variety of pathologies Sylvia Õunpuu,
Assessments SIMPLY GAIT. Posture and Gait. Observing Posture and Gait. Postural Assessment. Postural Assessment 6/28/2016
 Assessments 2 SIMPLY GAIT Understanding movement Evaluations of factors that help therapist form professional judgments Include health, palpatory, range of motion, postural, and gait assessments Assessments
Assessments 2 SIMPLY GAIT Understanding movement Evaluations of factors that help therapist form professional judgments Include health, palpatory, range of motion, postural, and gait assessments Assessments
Comparison of Langer Biomechanic s DynaFlange to Traditional Legacy Rearfoot Posted Orthotics
 Comparison of Langer Biomechanic s DynaFlange to Traditional Legacy Rearfoot Posted Orthotics This study demonstrates the advantages of these devices. BY SALLY M. CRAWFORD, MS Background Motion control,
Comparison of Langer Biomechanic s DynaFlange to Traditional Legacy Rearfoot Posted Orthotics This study demonstrates the advantages of these devices. BY SALLY M. CRAWFORD, MS Background Motion control,
BIOMECHANICAL EVALUATION OF RUNNING AND SOCCER SHOES: METHODOLOGY AND TESTING PROCEDURES. Ewald M. Hennig
 BIOMECHANICAL EVALUATION OF RUNNING AND SOCCER SHOES: METHODOLOGY AND TESTING PROCEDURES Ewald M. Hennig Biomechanics Laboratory, University Duisburg-Essen, Essen, Germany Running shoes are the footwear,
BIOMECHANICAL EVALUATION OF RUNNING AND SOCCER SHOES: METHODOLOGY AND TESTING PROCEDURES Ewald M. Hennig Biomechanics Laboratory, University Duisburg-Essen, Essen, Germany Running shoes are the footwear,
Diabetes and Orthoses. Rob Bradbury Talar Made
 Diabetes and Orthoses Rob Bradbury Talar Made Diabetes High prevalence disease 4-6% in UK (over 2.5 mill diagnosed and a further 0.5 ) 6+% in USA 40% in some parts of Middle East (may be higher in Indian
Diabetes and Orthoses Rob Bradbury Talar Made Diabetes High prevalence disease 4-6% in UK (over 2.5 mill diagnosed and a further 0.5 ) 6+% in USA 40% in some parts of Middle East (may be higher in Indian
Assessment of Subtalar Joint Neutral Position: Study of Image Processing for Rear Foot Image
 Assessment of Subtalar Joint Neutral Position: Study of Image Processing for Rear Foot Image C. H. Lin, C. C. Yeh, and Z. H. Qiu Abstract The subtalar joint is in neutral when it is neither pronated nor
Assessment of Subtalar Joint Neutral Position: Study of Image Processing for Rear Foot Image C. H. Lin, C. C. Yeh, and Z. H. Qiu Abstract The subtalar joint is in neutral when it is neither pronated nor
Palacký Univerzity in Olomouc Faculty of Physical Culture
 Project: Sophisticated biomechanic diagnostics of human movement Registration number: CZ.1.07/2.3.00/09.0209 Palacký Univerzity in Olomouc Faculty of Physical Culture Tento projekt je spolufinancován Evropským
Project: Sophisticated biomechanic diagnostics of human movement Registration number: CZ.1.07/2.3.00/09.0209 Palacký Univerzity in Olomouc Faculty of Physical Culture Tento projekt je spolufinancován Evropským
Aeris Performance 2. Product Manual
 Aeris Performance 2 Product Manual Instructions The Aeris Performance 2 is designed to be maintenance free. The foot is water resistant; however, if the foot is submerged in water, the foot and foot shell
Aeris Performance 2 Product Manual Instructions The Aeris Performance 2 is designed to be maintenance free. The foot is water resistant; however, if the foot is submerged in water, the foot and foot shell
Static postural control, or
 Comparison of Different Structural Foot Types for Measures of Standing Postural Control Liang-Ching Tsai, PT, MS 1 Bing Yu, PhD 2 Vicki S. Mercer, PT, PhD 2 Michael T. Gross, PT, PhD 3 Journal of Orthopaedic
Comparison of Different Structural Foot Types for Measures of Standing Postural Control Liang-Ching Tsai, PT, MS 1 Bing Yu, PhD 2 Vicki S. Mercer, PT, PhD 2 Michael T. Gross, PT, PhD 3 Journal of Orthopaedic
Customized rocker sole constructions
 Customized rocker sole constructions German guidelines to improve results in daily practice Stief, Thomas Registered Association for the Encouragement of Research and Education Management in Orthopedic
Customized rocker sole constructions German guidelines to improve results in daily practice Stief, Thomas Registered Association for the Encouragement of Research and Education Management in Orthopedic
Is it important to position foot in subtalar joint neutral position during non-weight-bearing molding for foot orthoses?
 University of Wollongong Research Online Faculty of Engineering and Information Sciences - Papers: Part A Faculty of Engineering and Information Sciences 2012 Is it important to position foot in subtalar
University of Wollongong Research Online Faculty of Engineering and Information Sciences - Papers: Part A Faculty of Engineering and Information Sciences 2012 Is it important to position foot in subtalar
L A B Mask 8 Mask 5 Mask 6 Mask 3 Mask 9 Mask 10 Mask 7 Mask 4 Mask 1 Mask 2 Figure 1. Imprint Index calculation. L = line drawn along medial border o
 The effect of low-dye taping on peak plantar pressures of normal feet during gait Sonia J Russo and Lucy S Chipchase University of South Australia This study investigated whether low-dye anti-pronation
The effect of low-dye taping on peak plantar pressures of normal feet during gait Sonia J Russo and Lucy S Chipchase University of South Australia This study investigated whether low-dye anti-pronation
Element DS. Product Manual
 Element DS Product Manual Instructions The Element DS is designed to be maintenance free. The foot is water resistant; however, if the foot is submerged in water, the foot and foot shell should be rinsed
Element DS Product Manual Instructions The Element DS is designed to be maintenance free. The foot is water resistant; however, if the foot is submerged in water, the foot and foot shell should be rinsed
Chapter 1 - Injury overview Chapter 2 - Fit for Running Assessment Chapter 3 - Soft Tissue Mobilization... 21
 Table of Contents Introduction Chapter 1 - Injury overview... 6 Chapter 2 - Fit for Running Assessment... 13 Chapter 3 - Soft Tissue Mobilization... 21 Chapter 4 - Dynamic Warm-up... 28 Chapter 5 - Strengthening...
Table of Contents Introduction Chapter 1 - Injury overview... 6 Chapter 2 - Fit for Running Assessment... 13 Chapter 3 - Soft Tissue Mobilization... 21 Chapter 4 - Dynamic Warm-up... 28 Chapter 5 - Strengthening...
Footwear and Foot Orthotic Effectiveness Research: A New Approach
 Footwear and Foot Orthotic Effectiveness Research: A New Approach Mark W. Cornwall, PhD, PT ' Thomas G. McPoil, PhD, PT, ATC Mark W. Cornwall Thomas G. McPoil inematic analysis of the rearfoot has been
Footwear and Foot Orthotic Effectiveness Research: A New Approach Mark W. Cornwall, PhD, PT ' Thomas G. McPoil, PhD, PT, ATC Mark W. Cornwall Thomas G. McPoil inematic analysis of the rearfoot has been
Figure 1 betois (bending torsion insole system) system with five measuring points and A/D- converter.
 system with five measuring points and A/D- converter.") Bending and Torsional Moments - A new measuring system for gait analysis Nora Dawin & Annette Kerkhoff & Klaus Peikenkamp, University of Applied Sciences Münster, Germany Abstract The Laboratory of Biomechanics
Bending and Torsional Moments - A new measuring system for gait analysis Nora Dawin & Annette Kerkhoff & Klaus Peikenkamp, University of Applied Sciences Münster, Germany Abstract The Laboratory of Biomechanics
A Comparison of Different Casting Methods and How They Affect the Orthotic Device Produced.
 A Comparison of Different Casting Methods and How They Affect the Orthotic Device Produced. University of Western Ontario Pedorthics Program PED 121 A. Brian Stoodley The exact essay title that was suggested
A Comparison of Different Casting Methods and How They Affect the Orthotic Device Produced. University of Western Ontario Pedorthics Program PED 121 A. Brian Stoodley The exact essay title that was suggested
Arch Height and Running Shoes: The Best Advice to Give Patients
 Arch Height and Running Shoes: The Best Advice to Give Patients by Thomas C. Michaud, DC Published May 1, 2014 by Dynamic Chiropractic Magazine Because runners with different arch heights are prone to
Arch Height and Running Shoes: The Best Advice to Give Patients by Thomas C. Michaud, DC Published May 1, 2014 by Dynamic Chiropractic Magazine Because runners with different arch heights are prone to
The Starting Point. Prosthetic Alignment in the Transtibial Amputee. Outline. COM Motion in the Coronal Plane
 Prosthetic Alignment in the Transtibial Amputee The Starting Point David C. Morgenroth, MD, Department of Rehabilitation Medicine University of Washington VAPSHCS Outline COM Motion in the Coronal Plane
Prosthetic Alignment in the Transtibial Amputee The Starting Point David C. Morgenroth, MD, Department of Rehabilitation Medicine University of Washington VAPSHCS Outline COM Motion in the Coronal Plane
Aeris Activity. Product Manual
 Aeris Activity Product Manual Instructions The Aeris Activity Foot System has been designed and manufactured for specific patient weights. Failure to follow the weight guidelines and/or overload conditions
Aeris Activity Product Manual Instructions The Aeris Activity Foot System has been designed and manufactured for specific patient weights. Failure to follow the weight guidelines and/or overload conditions
BIOMECHANICAL ASSESSMENT & ORTHOTIC SALES SCRIPTS
 BIOMECHANICAL ASSESSMENT & ORTHOTIC SALES SCRIPTS 1 Categories the client Categorise who the potential client actually is, as this will guide how you present the sale. a) Current patient of yours pre-existing
BIOMECHANICAL ASSESSMENT & ORTHOTIC SALES SCRIPTS 1 Categories the client Categorise who the potential client actually is, as this will guide how you present the sale. a) Current patient of yours pre-existing
Throw the Baby Out with the Bath Water? Challenging the Paradigm of Root Biomechanics
 Throw the Baby Out with the Bath Water? Challenging the Paradigm of Root Biomechanics Faculty Jarrod Shapiro, DPM, FACFAS, FACFAOM Associate Professor Western University of Health Sciences College of Podiatric
Throw the Baby Out with the Bath Water? Challenging the Paradigm of Root Biomechanics Faculty Jarrod Shapiro, DPM, FACFAS, FACFAOM Associate Professor Western University of Health Sciences College of Podiatric
'Supporting' the Foot 2 May 2002
 'Supporting' the Foot 2 May 2002 Proper alignment of the foot is widely considered as being necessary for normal function during gait. Poor alignment of the foot is associated with symptoms such as metatarsalgia,
'Supporting' the Foot 2 May 2002 Proper alignment of the foot is widely considered as being necessary for normal function during gait. Poor alignment of the foot is associated with symptoms such as metatarsalgia,
Orthotic intervention in forefoot and rearfoot strike running patterns
 Clinical Biomechanics 19 (24) 64 7 www.elsevier.com/locate/clinbiomech Orthotic intervention in forefoot and rearfoot strike running patterns Carrie Laughton Stackhouse a, *, Irene McClay Davis b,c, Joseph
Clinical Biomechanics 19 (24) 64 7 www.elsevier.com/locate/clinbiomech Orthotic intervention in forefoot and rearfoot strike running patterns Carrie Laughton Stackhouse a, *, Irene McClay Davis b,c, Joseph
Purpose A patented technology designed to improve stability of the human foot.
 The Richie ArchLock Technology Purpose A patented technology designed to improve stability of the human foot. Description A platform of specific dimension, strategically placed under the human foot. This
The Richie ArchLock Technology Purpose A patented technology designed to improve stability of the human foot. Description A platform of specific dimension, strategically placed under the human foot. This
10/22/15. Walking vs Running. Normal Running Mechanics. Treadmill vs. Overground Are they the same? Importance of Gait Analysis.
 2 angle (deg) 1/22/1 Normal Running Mechanics Walking vs Running Irene Davis, PhD, PT, FACSM, FAPTA, FASB Director, Spaulding National Running Center Walking Periods of DOUBLE SUPPORT Running Periods of
2 angle (deg) 1/22/1 Normal Running Mechanics Walking vs Running Irene Davis, PhD, PT, FACSM, FAPTA, FASB Director, Spaulding National Running Center Walking Periods of DOUBLE SUPPORT Running Periods of
The DAFO Guide to Brace Selection
 The DAFO Guide to Brace Selection Cascade Dafo believes... better mobility gives children a wider range of experiences, more success in the activities they choose, and ultimately more control over their
The DAFO Guide to Brace Selection Cascade Dafo believes... better mobility gives children a wider range of experiences, more success in the activities they choose, and ultimately more control over their
WalkOn product range. Dynamic Ankle-Foot Orthoses. Information for specialist dealers
 WalkOn product range Dynamic Ankle-Foot Orthoses Information for specialist dealers WalkOn Flex WalkOn WalkOn Trimable WalkOn Reaction WalkOn Reaction plus One range Many different applications The WalkOn
WalkOn product range Dynamic Ankle-Foot Orthoses Information for specialist dealers WalkOn Flex WalkOn WalkOn Trimable WalkOn Reaction WalkOn Reaction plus One range Many different applications The WalkOn
AllPro Foot. Product Manual
 AllPro Foot Product Manual Instructions The AllPro Foot System has been designed and manufactured for specific patient weights. Failure to follow the weight guidelines and/or overload conditions caused
AllPro Foot Product Manual Instructions The AllPro Foot System has been designed and manufactured for specific patient weights. Failure to follow the weight guidelines and/or overload conditions caused
GROUND REACTION FORCE DOMINANT VERSUS NON-DOMINANT SINGLE LEG STEP OFF
 GROUND REACTION FORCE DOMINANT VERSUS NON-DOMINANT SINGLE LEG STEP OFF Sara Gharabaghli, Rebecca Krogstad, Sara Lynch, Sofia Saavedra, and Tamara Wright California State University, San Marcos, San Marcos,
GROUND REACTION FORCE DOMINANT VERSUS NON-DOMINANT SINGLE LEG STEP OFF Sara Gharabaghli, Rebecca Krogstad, Sara Lynch, Sofia Saavedra, and Tamara Wright California State University, San Marcos, San Marcos,
Running Gait Mechanics. Walking vs Running. Ankle Joint Complex Sagittal Plane. As speed increases, when has walking ended and running begun?
 Running Gait Mechanics Walking vs Running As speed increases, when has walking ended and running begun? Ankle Joint Complex Sagittal Plane 1 Ankle Joint Complex Sagittal Plane Pos. @FS 5 o DF Absorption
Running Gait Mechanics Walking vs Running As speed increases, when has walking ended and running begun? Ankle Joint Complex Sagittal Plane 1 Ankle Joint Complex Sagittal Plane Pos. @FS 5 o DF Absorption
The Human Foot. The Three Major Sections of the Foot
 The Human Foot You ve heard the phrase I have one foot bigger than the other. A closer truth would be no two feet are alike, and yes in many cases one foot is larger than the other. Handling the challenge
The Human Foot You ve heard the phrase I have one foot bigger than the other. A closer truth would be no two feet are alike, and yes in many cases one foot is larger than the other. Handling the challenge
Does Changing Step Width Alter Lower Extremity Biomechanics During Running?
 University of Tennessee, Knoxville Trace: Tennessee Research and Creative Exchange Masters Theses Graduate School 5-2012 Does Changing Step Width Alter Lower Extremity Biomechanics During Running? Richard
University of Tennessee, Knoxville Trace: Tennessee Research and Creative Exchange Masters Theses Graduate School 5-2012 Does Changing Step Width Alter Lower Extremity Biomechanics During Running? Richard
Biofeedback Insole can help to Increase Performance and Comfort, and Reduce Injury.
 Biofeedback Insole can help to Increase Performance and Comfort, and Reduce Injury. During independent third party testing for consumer acceptance and evaluation purposes the device was found to provide
Biofeedback Insole can help to Increase Performance and Comfort, and Reduce Injury. During independent third party testing for consumer acceptance and evaluation purposes the device was found to provide
SAPPHIRE PHYSICAL THERAPY
 www.fisiokinesiterapia.biz SAPPHIRE PHYSICAL THERAPY PRESENTATION OUTLINE Foot Facts Foot & Ankle Anatomy Shoe Anatomy Common Foot Injuries Orthotics Sport & Activity Specific Shoes Questions & Answers
www.fisiokinesiterapia.biz SAPPHIRE PHYSICAL THERAPY PRESENTATION OUTLINE Foot Facts Foot & Ankle Anatomy Shoe Anatomy Common Foot Injuries Orthotics Sport & Activity Specific Shoes Questions & Answers
Running from injury 2
 Created as a free resource by Clinical Edge Based on Physio Edge podcast 049 with Dr Rich Willy Get your free trial of online Physio education by clicking here Running injuries & assessment Running assessment
Created as a free resource by Clinical Edge Based on Physio Edge podcast 049 with Dr Rich Willy Get your free trial of online Physio education by clicking here Running injuries & assessment Running assessment
REPORT. A comparative study of the mechanical and biomechanical behaviour of natural turf and hybrid turf for the practise of sports
 REPORT A comparative study of the mechanical and biomechanical behaviour of natural turf and hybrid turf for the practise of sports Addressed to: PSF - PALAU TURF Date: May 2015 Table of Contents SHEET
REPORT A comparative study of the mechanical and biomechanical behaviour of natural turf and hybrid turf for the practise of sports Addressed to: PSF - PALAU TURF Date: May 2015 Table of Contents SHEET
IJPHY ABSTRACT. Int J Physiother. Vol 4(6), , December (2017) ISSN: ORIGINAL ARTICLE
, , December (2017) ISSN: ORIGINAL ARTICLE") Int J Physiother. Vol 4(6), 343-347, December (2017) ISSN: 2348-8336 ORIGINAL ARTICLE IJPHY ABSTRACT VALIDITY AND REPRODUCIBILITY OF MEASURING THE KINEMATIC COUPLING BEHAVIOR OF CALCANEAL PRONATION/SUPINATION
Int J Physiother. Vol 4(6), 343-347, December (2017) ISSN: 2348-8336 ORIGINAL ARTICLE IJPHY ABSTRACT VALIDITY AND REPRODUCIBILITY OF MEASURING THE KINEMATIC COUPLING BEHAVIOR OF CALCANEAL PRONATION/SUPINATION
The Lateralized Foot & Ankle Pattern and the Pronated Left Chest
 The Lateralized Foot & Ankle Pattern and the Pronated Left Chest Presented by: James Anderson, MPT, PRC Director of Affiliate Programs, Faculty & Board of Certification Postural Restoration Institute Pronate
The Lateralized Foot & Ankle Pattern and the Pronated Left Chest Presented by: James Anderson, MPT, PRC Director of Affiliate Programs, Faculty & Board of Certification Postural Restoration Institute Pronate
Introduction to Biomechanical Evaluation Qualitative Biomechanics Peter G. Guy B.Sc., D.Ch.
 Introduction to Biomechanical Evaluation Qualitative Biomechanics Peter G. Guy B.Sc., D.Ch. During the course of a biomechanical evaluation the findings are recorded in either a qualitative or quantitative
Introduction to Biomechanical Evaluation Qualitative Biomechanics Peter G. Guy B.Sc., D.Ch. During the course of a biomechanical evaluation the findings are recorded in either a qualitative or quantitative
Pathomechanics of Structural Foot Deformities
 Pathomechanics of Structural Foot Deformities DAVID TIBERIO This article presents the most common structural foot deformities encountered in clinical practice. The deformities are defined, and the expected
Pathomechanics of Structural Foot Deformities DAVID TIBERIO This article presents the most common structural foot deformities encountered in clinical practice. The deformities are defined, and the expected
THE EFFECTS OF ORTHOTICS ON LOWER EXTREMITY VARIABILITY DURING RUNNING. Samuel Brethauer
 THE EFFECTS OF ORTHOTICS ON LOWER EXTREMITY VARIABILITY DURING RUNNING. By Samuel Brethauer Submitted to the graduate degree program in Health, Sport, and Exercise Science and the Graduate Faculty of the
THE EFFECTS OF ORTHOTICS ON LOWER EXTREMITY VARIABILITY DURING RUNNING. By Samuel Brethauer Submitted to the graduate degree program in Health, Sport, and Exercise Science and the Graduate Faculty of the
Normal and Abnormal Gait
 Normal and Abnormal Gait Adrielle Fry, MD EvergreenHealth, Division of Sport and Spine University of Washington Board Review Course March 6, 2017 What are we going to cover? Definitions and key concepts
Normal and Abnormal Gait Adrielle Fry, MD EvergreenHealth, Division of Sport and Spine University of Washington Board Review Course March 6, 2017 What are we going to cover? Definitions and key concepts
PHASIC POSTING Putting The Function Into Foot Orthoses. Bob Longworth MSc DPodM Lee Short MSc
 PHASIC POSTING Putting The Function Into Foot Orthoses Bob Longworth MSc DPodM Lee Short MSc A Phasic Posting approach to insoles AGENDA 1. What is a functional foot orthotic? 2. Problems with the theories
PHASIC POSTING Putting The Function Into Foot Orthoses Bob Longworth MSc DPodM Lee Short MSc A Phasic Posting approach to insoles AGENDA 1. What is a functional foot orthotic? 2. Problems with the theories
RUNNING. Normal Running 10/10/2016. Reliability and Concurrent Validity of a 2D Observational Gait Analysis Tool
 Reliability and Concurrent Validity of a 2D Observational Gait Analysis Tool Kevin Yu, SPT Robert Wayner, PT, DPT Jennifer Smith, PT, DPT RUNNING Stance Phase (Single Limb Support) Initial Contact / Foot
Reliability and Concurrent Validity of a 2D Observational Gait Analysis Tool Kevin Yu, SPT Robert Wayner, PT, DPT Jennifer Smith, PT, DPT RUNNING Stance Phase (Single Limb Support) Initial Contact / Foot
Plantar Foot Pressures After the Augmented Low Dye Taping Technique
 Journal of Athletic Training 2007;42(3):374 380 by the National Athletic Trainers Association, Inc www.journalofathletictraining.org Plantar Foot Pressures After the Augmented Low Dye Taping Technique
Journal of Athletic Training 2007;42(3):374 380 by the National Athletic Trainers Association, Inc www.journalofathletictraining.org Plantar Foot Pressures After the Augmented Low Dye Taping Technique
Running injuries - what are the most important factors
 Created as a free resource by Clinical Edge Based on Physio Edge podcast 59 with Greg Lehman, Tom Goom and Dr Christian Barton Get your free trial of online Physio education at Why do runners get injured?
Created as a free resource by Clinical Edge Based on Physio Edge podcast 59 with Greg Lehman, Tom Goom and Dr Christian Barton Get your free trial of online Physio education at Why do runners get injured?
Biomechanical Foot Orthotics: A Retrospective Study
 0196-601 l/88/1 005-0205$02.00/0 THE JOURNAL OF ORTHOPAED~C AND SPORTS PHYSICAL THERAPY Copyright C3 1988 by The Orthopaedic and Sports Physical Therapy Sections of the American Physical Therapy Association
0196-601 l/88/1 005-0205$02.00/0 THE JOURNAL OF ORTHOPAED~C AND SPORTS PHYSICAL THERAPY Copyright C3 1988 by The Orthopaedic and Sports Physical Therapy Sections of the American Physical Therapy Association
A Biomechanical Assessment of Gait Patterns and Risk of Associated Overuse Conditions among Mature Female Runners.
 A Biomechanical Assessment of Gait Patterns and Risk of Associated Overuse Conditions among Mature Female Runners. Submitted by Kim Louise Lilley to the University of Exeter as a thesis for the degree
A Biomechanical Assessment of Gait Patterns and Risk of Associated Overuse Conditions among Mature Female Runners. Submitted by Kim Louise Lilley to the University of Exeter as a thesis for the degree
The Unified Theory of Foot Function
 The Unified Theory of Foot Function Paul Harradine MSc FCPodMed CertEd Podiatrist / Director The Podiatry and Chiropody Centre, Cosham. Hants www.podiatryandchiropodycentre.com The Podiatry Centre, Farnham,
The Unified Theory of Foot Function Paul Harradine MSc FCPodMed CertEd Podiatrist / Director The Podiatry and Chiropody Centre, Cosham. Hants www.podiatryandchiropodycentre.com The Podiatry Centre, Farnham,
Foot Posture Biomechanics and MASS Theory
 The Foot and Ankle Online Journal Official Publication of the International Foot & Ankle Foundation faoj.com / ISSN 1941-6806 Foot Posture Biomechanics and MASS Theory by Edward S Glaser 1 and David Fleming
The Foot and Ankle Online Journal Official Publication of the International Foot & Ankle Foundation faoj.com / ISSN 1941-6806 Foot Posture Biomechanics and MASS Theory by Edward S Glaser 1 and David Fleming
A bit of background. Session Schedule 3:00-3:10: Introduction & session overview. Overarching research theme: CPTA
 A Cognitive-Biomechanical Perspective for the Management of Common Chronic Musculoskeletal Conditions Skulpan Asavasopon, PT, PhD Loma Linda University Christopher M. Powers, PT, PhD, FAPTA University
A Cognitive-Biomechanical Perspective for the Management of Common Chronic Musculoskeletal Conditions Skulpan Asavasopon, PT, PhD Loma Linda University Christopher M. Powers, PT, PhD, FAPTA University
THE INFLUENCE OF SLOW RECOVERY INSOLE ON PLANTAR PRESSURE AND CONTACT AREA DURING WALKING
 March 12, 2015 5:39:44pm WSPC/170-JMMB 1540005 ISSN: 0219-51942nd Reading Journal of Mechanics in Medicine and Biology Vol. 15, No. 2 (2015) 1540005 (6 pages) c World Scientific Publishing Company DOI:
March 12, 2015 5:39:44pm WSPC/170-JMMB 1540005 ISSN: 0219-51942nd Reading Journal of Mechanics in Medicine and Biology Vol. 15, No. 2 (2015) 1540005 (6 pages) c World Scientific Publishing Company DOI:
Evidence-Based Medicine: Foot Imaging for Custom Functional Foot Orthoses
 Evidence-Based Medicine: Foot Imaging for Custom Functional Foot Orthoses Lawrence Z. Huppin, DPM* and Paul R. Scherer, DPM** The purpose of this article is to: 1. Review the literature to determine evidencebased
Evidence-Based Medicine: Foot Imaging for Custom Functional Foot Orthoses Lawrence Z. Huppin, DPM* and Paul R. Scherer, DPM** The purpose of this article is to: 1. Review the literature to determine evidencebased
Ice skating in all its various forms. Living on the Edge: The Biomechanics of Power Skating
 Living on the Edge: The Biomechanics of Power Skating There are some very specific overuse injury patterns seen in the ice hockey population. 135 By R. Neil Humble, DPM Ice skating in all its various forms
Living on the Edge: The Biomechanics of Power Skating There are some very specific overuse injury patterns seen in the ice hockey population. 135 By R. Neil Humble, DPM Ice skating in all its various forms
Gait analysis through sound
 Invited article Niigata Journal of Health and Welfare Vol. 15, No. 1 Gait analysis through sound Kaoru Abe Graduate School of Health and Welfare, Niigata University of Health and Welfare, Niigata, Japan
Invited article Niigata Journal of Health and Welfare Vol. 15, No. 1 Gait analysis through sound Kaoru Abe Graduate School of Health and Welfare, Niigata University of Health and Welfare, Niigata, Japan
11/11/2012. Associations of Foot Forces and Pressures to Regional Foot Pain: The Framingham Foot Study. Acknowledgements & Disclosures
 11/11/2012 Associations of Foot Forces and Pressures to Regional Foot Pain: The Jody L. Riskowski, PhD, CSCS Institute for Aging Research (IFAR), Hebrew SeniorLife Harvard Medical School Boston, MA, USA
11/11/2012 Associations of Foot Forces and Pressures to Regional Foot Pain: The Jody L. Riskowski, PhD, CSCS Institute for Aging Research (IFAR), Hebrew SeniorLife Harvard Medical School Boston, MA, USA
Abstract. Introduction
 Measurement of Medial Malleolar Drift and Medial Longitudinal Arch Height: A Reliability Study of Two Novel Devices Katie Long, SPT, Leigh Miller, SPT, Jacob Manly, SPT, Nicole Vo, SPT, AJ Lievre, PT,
Measurement of Medial Malleolar Drift and Medial Longitudinal Arch Height: A Reliability Study of Two Novel Devices Katie Long, SPT, Leigh Miller, SPT, Jacob Manly, SPT, Nicole Vo, SPT, AJ Lievre, PT,
Mobility Lab provides sensitive, valid and reliable outcome measures.
 Mobility Lab provides sensitive, valid and reliable outcome measures. ith hundreds of universities and hospitals using this system worldwide, Mobility Lab is the most trusted wearable gait and balance
Mobility Lab provides sensitive, valid and reliable outcome measures. ith hundreds of universities and hospitals using this system worldwide, Mobility Lab is the most trusted wearable gait and balance
Axis of rotation is always perpendicular to the plane of movement
 Sports scientists and medical practitioners use formal terms to describe directionality, joint movement, and muscle movement. These universal terms let us use fewer words when describing movement, teaching,
Sports scientists and medical practitioners use formal terms to describe directionality, joint movement, and muscle movement. These universal terms let us use fewer words when describing movement, teaching,