Evaluating the evidence using GRADE. Peter Morley E th October 2012
|
|
|
- Shannon Greene
- 5 years ago
- Views:
Transcription

1 1 Evaluating the evidence using GRADE Peter Morley E th October 2012
2 2 Conflict of interest disclosure Commercial/industry Evidence Evaluation Expert (ILCOR/AHA) Potential intellectual conflicts Deputy Chair Australian Resuscitation Council (ARC) Chair ALS Committee ARC ARC rep on International Liaison Committee on Resuscitation (ILCOR) Evidence Evaluation Expert (ILCOR/AHA)
3 So what is GRADE? 3
4 4 Grading of Recommendations Assessment, Development, and Evaluation (GRADE) Process to take evidence to guidelines Developed by key international groups Widely accepted internationally
5 5
6 GRADE 6 Offers a transparent and structured process for developing and presenting summaries of evidence, including its quality, for systematic reviews and recommendations in health care. Provides guideline developers with a comprehensive and transparent framework for carrying out the steps involved in developing recommendations. Use is appropriate and helpful irrespective of the quality of the evidence: whether high or very low. Does not eliminate the inevitable need for judgments.
7 7
8 GRADE process adopted by: 8 American College of Physicians The Cochrane Collaboration American College of Chest Physicians European Society of Thoracic Surgeons American Thoracic Society Agency for Healthcare Research and Quality Society of Critical Care Medicine Up to Date WHO NIH NICE Endocrine Society

9 GRADE uptake 9
10 10 Lots of educational material existing
11 Journals Journal of Clinical Epidemiology (2011-2) 12 articles (more to come in series) extensive review, major reference for GRADE methodology BMJ Series (2008) 7 articles initial concepts of GRADE and justification documents Multiple other publications 11
 12")
12 Grade (1997) 12
13 13 GRADE (1997) Allows downgrading of quality estimate if involve indirect evidence Population groups? Animals etc! Prognostic or aetiologic studies only useful if their use modifies outcomes! Very good approach to making recommendations
")
14 14 Grade (1997)
15 15 Comparisons and proposal C2010 Study type/approach C2005 Grade SIGN NH&MRC OCEBM Meta-analyses 1 or 2 1 n/a 1++ to 2++ I 1a or 2a RCTs 1 or 2 High/Mod/Low 1/1+/1++ II 1b or 2b 1 Concurrent controls 2 3 High/Mod/Low 2- to 2++ III-1 or III-2 2b to 4 Retrospective controls 3 4 Low n/a III-3?1c! No controls 4 5 Very low 3 IV 4 Animal/Mechanical/Model 5 6? As for extrap n/a n/a n/a Extrapolations 7 Downgraded n/a n/a n/a 5 YES Covers "non-therapy" studies?1to7 Irrelevant! No Detailed Detailed GRADE approach closest to our needs Not numerical Needs additional non-therapy LOEs OCEBM or NH&MRC
16 16 What are the principles behind GRADE?
17 17 GRADE is outcome-centric Outcome #1 Outcome #2 Outcome #3 Quality: High Quality: Moderate Quality: Low III V II I B Older systems GRADE
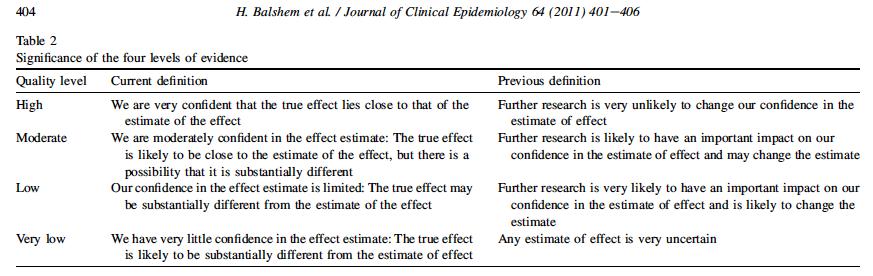
18 GRADE: Quality of evidence The extent to which our confidence in an estimate of the treatment effect is adequate to support a particular recommendation. 18 GRADE defines 4 categories of quality: High Moderate Low Very low 18
19 19 Conceptualizing quality High Moderate Low Very low We are very confident that the true effect lies close to that of the estimate of the effect. Our confidence in the effect is limited: The true effect may be substantially different from the estimate of the effect. We are moderately confident in the estimate of effect: The true effect is likely to be close to the estimate of effect, but possibility to be substantially different. We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect. 19
20 GRADE Recommendations 20 Strong recommendations strong methods large precise effect few downsides of therapy expect non-variant clinician and patient behavior diminished role for clinical expertise focus on implementation & barriers focused role of patient values and preferences emphasis on compliance and barriers Clinical Experience Research Evidence Weak recommendations weak methods imprecise estimate small effect substantial downsides expect variability in clinician and patient actions clinical expertise important focus on decision-making and implementation patient values and preferences important focus on determining values and preferences relative to decision Patient Values and Preferences
21 So why adopt GRADE? 21
22 22 Apart from international consensus Allows more clarity and consistency when move from evidence to recommendations
23 23 So is this really different to the C2010 approach?
24 24 Differences between processes 2010 ILCOR Identify PICO question Search for studies Clear inclusion exclusion criteria Identify studies for detailed review Identify key (critical) outcomes of relevance 2015 ILCOR (GRADE) Identify PICO question Search for studies Clear inclusion exclusion criteria Identify studies for detailed review Identify key (critical) outcomes of relevance
25 25 Differences between processes 2010 ILCOR Allocate study LOE: from LOE 1 to LOE 5 Allocate methodological quality for each study All studies (with outcomes) into grid according to direction for specific question 2015 ILCOR (GRADE) Allocate study type: RCTs or observational Assess risk of bias for each study All studies (with outcomes) into risk of bias table (including overall risk of bias for each study)
26 26 Assessment of methodological quality (risk of bias) of RCTs: similar 2010: ILCOR Quality RCTs (not clearly documented) Adequacy of randomization Allocation concealment Blinding Loss to follow up Intention to Treat (IT) analysis Groups treated equally? Groups similar at the start? 2015: GRADE Risk of bias RCTs (clearly documented) Adequacy of randomization Allocation concealment Blinding Loss to follow-up, Intention to Treat (IT) analysis Any other risks? Early stopping for positive benefit others
27 Allocation of quality 27 vs downgrading for RCTs: similar 2010: Quality for individual RCT Good studies most/all of the relevant quality items Fair studies have some of the relevant quality items Poor studies have few of the relevant quality items (but sufficient value to include for further review). Excluded insufficient relevant quality items to be included 2015: Overall risk of bias for individual RCT Low (?Good) Unclear (?Fair) High (?Poor)
28 Published (extras at 5) 28
29 29 Remember our evidence table Summary of evidence Evidence Supporting Clinical Question Good Fair Poor Level of evidence A = Return of spontaneous circulation C = Survival to hospital discharge E = Other endpoint B = Survival of event neurological survival Italics = Animal studies D = Intact
30 30
31 Overall risk of bias for study: Low, Moderate or High Low risk of bias = most or all key criteria listed are met, and any violations are not crucial. Moderate risk of bias if have a crucial limitation in one criterion or some in multiple criteria, sufficient to lower the confidence in the estimate of effect. High risk of bias if have a crucial limitation in one or more criteria, sufficient to substantially lower the confidence in the estimate of effect. 31
32 32 Differences between processes 2010 ILCOR Narrative description of key information from all studies 2015 ILCOR (GRADE) Narrative description of key information from all studies Plus specific information regarding evidence for each key outcome Evidence profile table(s) Summary of findings table(s)
33 33 Major difference in approach for GRADE Key outcome measures are allocated a numerical rating Critical 9, 8, 7 Important 6, 5, 4 Limited importance 3, 2, 1 Quality of evidence is assessed (across studies) for each key outcome
34 34 How is the evidence for each outcome collated? Evidence Profile table(s) Summary of Findings table(s) Narrative description Consensus on Science statement
35 Evidence Profile table(s) 35 PICO question Outcome to which evidence applies No of studies that report data for that outcome Study Design (RCT, Observational etc) Risk of bias (: no serious, serious, very serious) Inconsistency (: no serious, serious, very serious) Indirectness (: no serious, serious, very serious) Imprecision (: no serious, serious, very serious) Other including publication bias (Undetected, strongly suspected) Overall Quality of evidence for outcome High, Moderate, Low, Very low
36 Evidence profile table 36
37 Classification across all studies for each outcome 37 Risk of Bias/Inconsistency/Indirectness/Imprecision No serious : Most information is from studies at low risk of bias. Do not downgrade Serious : Most information is from studies at moderate risk of bias. Rate down one level Very serious : Most information is from studies at high risk of bias. Rate down two levels
38 Classification across all studies for each outcome Publication Bias Undetected Strongly suspected Quality of Evidence across all included studies for outcome High Moderate Low Very Low 38
39 39
40 40
41 Quality of evidence for outcome (across all studies) Four final categories High Moderate Low Very low Start with high for RCTs Start with low for observational Can be modified according to a number of factors 41
42 42 RCTs can be downgraded all or most of the studies had sufficient problems to make estimate unreliable or uncertain design and execution (risk of bias) consistency of results directness of comparisons precision publication bias
43 Overall quality of evidence: for each key outcome across studies 43
44 44 What about even lower levels of evidence? Case series (LOE 4) Manikin/Models/Animals (LOE 5)
45 45 Case series Start at low/very low quality Can be upgraded
46 46

47 47 Case series Start at low quality Can be upgraded BUT not if would be downgraded first!
48 48
 49 Starting point depends on methodology BUT RCTs at high quality Observational at low quality")
49 Manikin/Models/Animals (LOE 5) (NB. GRADE not created for these) 49 Starting point depends on methodology BUT RCTs at high quality Observational at low quality Even RCTs can be downgraded Very serious indirectness = -2 Can be explained in comments
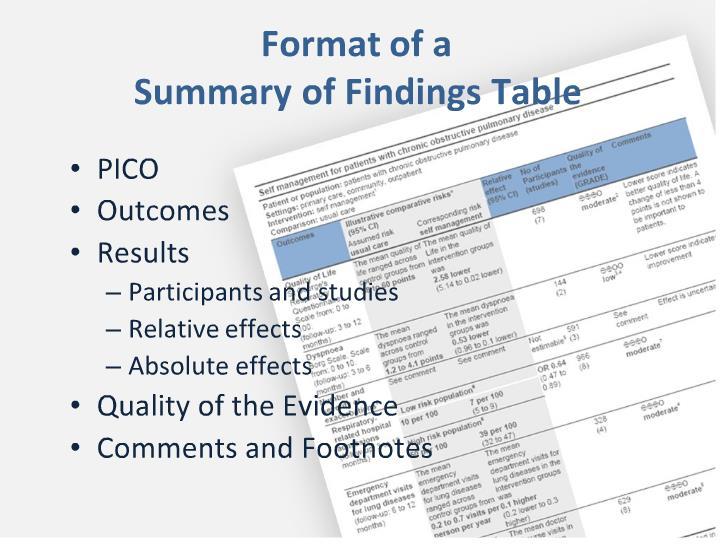
50 50 Summary of Findings table: columns PICO Key Outcomes Illustrative comparative risks (categorical or continuous with 95% CI) Control group Intervention group Relative effect (95% CI) No of Participants (studies) Overall quality of the evidence (GRADE) Comments/Footnotes
51 51 Summary of findings table Present a key summary graph or table Citation #1 Citation #2
52 52 Next = CoSTR Consensus on Science statement and Treatment Recommendations
53 53 Differences between processes 2010 Consensus on Science statement (based on listing of levels of evidence for specific outcomes) Treatment recommendation: using behavioral wording, based largely on quality of evidence 2015 Consensus on Science statement (based on overall quality of evidence for critical outcomes ) Treatment recommendation: strong or weak (with behavioral correlates), based on evidence quality (high, moderate, low, very low)
54 54 So how will our Consensus on Science statement and Treatment Recommendations differ? COS: Quality level of evidence (GRADE) TR: Strength of Recommendation (GRADE)
55 55 GRADE Strength of Recommendation Strong: the desirable effects of an intervention clearly outweigh the undesirable effects, or clearly do not. Weak: the trade-offs are less certain either because of low quality evidence or because evidence suggests that desirable and undesirable effects are closely balanced.
56 56 Strong Recommendation For patients most people in your situation would want the recommended course of action and only a small proportion would not; request discussion if the intervention is not offered For clinicians most patients should receive the recommended course of action
57 57 Weak Recommendation For patients most people in your situation would want the recommended course of action, but many would not For clinicians you should recognize that different choices will be appropriate for different patients and that you must help each patient to arrive at a management decision consistent with her or his values and preferences
58 58 So what might a GRADE review for ILCOR look like?
59 59 In adult cardiac arrest (prehospital [OHCA], in-hospital [IHCA]), does the use of an ITD (I) compared with no ITD (C), improve any outcomes (e.g. survival) (O)? Worksheet identifier: TBA Author: Peter Morley Affiliation: ANZCOR Taskforce: ALS/BLS Other Worksheet Authors: TBA
60 60 C2015 PICO Population: adult cardiac arrest (prehospital [OHCA], in-hospital [IHCA]) Intervention: the use of an ITD Comparison: compared with no ITD Outcomes Neurologically intact survival (critical 9) Discharge from hospital alive (critical 8) Return of spontaneous circulation (important 6)
61 61 Inclusion/Exclusion/Articles Found Included all studies with concurrent controls. Excluded review articles, studies with historical controls, animal studies, and studies that did not specifically answer the question. Excluded unpublished studies, studies only published in abstract form, unless accepted for publication. 8 Articles Finally Evaluated
62 62 Risk of Bias in studies table(s) Impedance Threshold Device + Standard CPR (I) vs Standard CPR (C) Study Random -ization Allocation concealment Blinding Loss to follow-up, Intention to Treat (IT) analysis Aufderheide 2005, 734 ITD+SCPR vs ShamITD+SCPR Pirallo 2005, 13 ITD+SCPR vs ShamITD+SCPR Aufderheide 2011, 798 ITD+SCPR vs ShamITD+SCPR Any other risks Outcomes to which these assessments apply Low Low Low Low Discontinued early. Indirectness: 2000 guidelines. All Low Unclear Low Low Changed device halfway into All Low study. Equipment problems Indirectness: 2000 guidelines. Low Low Low Low Indirectness: 2005 guidelines All Low Overall risk of bias for outcome(s) for study** Low Impedance Threshold Device + Active Compression Decompression CPR (I) vs Active Compression Decompression CPR (C) Study Random -ization Allocation concealment Blinding Any other risks Plaisance 2000, 989 ITD+ACD vs ACD Plaisance 2004, 265 ITD+ACD vs ShamITD+ACD Plaisance 2005, 990 ITD+ACD vs ShamITD+ACD Loss to follow-up, IT principle observed or per protocol analysis Low Low Low Low No description primary outcome/power. Indirectness: 1992 guidelines Low Low Low Low Automatic ventilator. Indirectness: 2000 guidelines. Low (order of use) Low Low Low Crossover trial. Indirectness: 2000 guidelines Outcomes to which these assessments apply All All All Overall risk of bias for outcome(s) for study** Low Low Moderate Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Study Random -ization Allocation concealment Blinding Loss to follow-up, IT principle observed or per Any other risks Wolcke 2003, 2201 ITD+ACD vs SCPR Aufderheide 2011, 301 ITD+ACD vs SCPR protocol analysis Low High High Low Indirectness:?1992/2000 guidelines Low Unclear High High: Significant differences in (only real time feedback about CPR outcome quality. Increase enrollment assessor) numbers then stop early. Unclear, some exclusions based on difficultly with airway border on deviation from IT analysis. Outcomes to which these assessments apply All All Overall risk of bias for outcome(s) for study** High High
63 63 Risk of Bias in studies table: ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Study Wolcke 2003, 2201 ITD+ACD vs SCPR Aufderheide 2011, 301 ITD+ACD vs SCPR Random -ization Allocation concealment Blinding Loss to follow-up, IT principle observed or per protocol analysis Any other risks Low High High Low Indirectness:?1992/2000 guidelines Low Unclear High High: Significant differences in (only real time feedback about CPR outcome quality. Increase enrollment assessor) numbers then stop early. Unclear, some exclusions based on difficultly with airway border on deviation from IT analysis. Outcomes to which these assessments apply All All Overall risk of bias for outcome(s) for study** High High
64 64 Risk of Bias in studies table: ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Study Wolcke 2003, 2201 ITD+ACD vs SCPR Aufderheide 2011, 301 ITD+ACD vs SCPR Random -ization Allocation concealment Blinding Loss to follow-up, IT principle observed or per protocol analysis Any other risks Low High High Low Indirectness:?1992/2000 guidelines Low Unclear High High: Significant differences in (only real time feedback about CPR outcome quality. Increase enrollment assessor) numbers then stop early. Unclear, some exclusions based on difficultly with airway border on deviation from IT analysis. Outcomes to which these assessments apply All All Overall risk of bias for outcome(s) for study** High High
65 65 Risk of Bias in studies table: ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Study Wolcke 2003, 2201 ITD+ACD vs SCPR Aufderheide 2011, 301 ITD+ACD vs SCPR Random -ization Allocation concealment Blinding Loss to follow-up, IT principle observed or per protocol analysis Any other risks Low High High Low Indirectness:?1992/2000 guidelines Low Unclear High High: Significant differences in (only real time feedback about CPR outcome quality. Increase enrollment assessor) numbers then stop early. Unclear, some exclusions based on difficultly with airway border on deviation from IT analysis. Outcomes to which these assessments apply All All Overall risk of bias for outcome(s) for study** High High
66 66 Risk of Bias in studies table: ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Study Wolcke 2003, 2201 ITD+ACD vs SCPR Aufderheide 2011, 301 ITD+ACD vs SCPR Random -ization Allocation concealment Blinding Loss to follow-up, IT principle observed or per protocol analysis Any other risks Low High High Low Indirectness:?1992/2000 guidelines Low Unclear High High: Significant differences in (only real time feedback about CPR outcome quality. Increase enrollment assessor) numbers then stop early. Unclear, some exclusions based on difficultly with airway border on deviation from IT analysis. Outcomes to which these assessments apply All All Overall risk of bias for outcome(s) for study** High High
67 67 Risk of Bias in studies table: ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Study Wolcke 2003, 2201 ITD+ACD vs SCPR Aufderheide 2011, 301 ITD+ACD vs SCPR Random -ization Allocation concealment Blinding Loss to follow-up, IT principle observed or per protocol analysis Any other risks Low High High Low Indirectness:?1992/2000 guidelines Low Unclear High High: Significant differences in (only real time feedback about CPR outcome quality. Increase enrollment assessor) numbers then stop early. Unclear, some exclusions based on difficultly with airway border on deviation from IT analysis. Outcomes to which these assessments apply All All Overall risk of bias for outcome(s) for study** High High
68 68 Risk of Bias in studies table: ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Study Wolcke 2003, 2201 ITD+ACD vs SCPR Aufderheide 2011, 301 ITD+ACD vs SCPR Random -ization Allocation concealment Blinding Loss to follow-up, IT principle observed or per protocol analysis Any other risks Low High High Low Indirectness:?1992/2000 guidelines Low Unclear High High: Significant differences in (only real time feedback about CPR outcome quality. Increase enrollment assessor) numbers then stop early. Unclear, some exclusions based on difficultly with airway border on deviation from IT analysis. Outcomes to which these assessments apply All All Overall risk of bias for outcome(s) for study** High High
69 69 Risk of Bias in studies table: ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Study Wolcke 2003, 2201 ITD+ACD vs SCPR Aufderheide 2011, 301 ITD+ACD vs SCPR Random -ization Allocation concealment Blinding Loss to follow-up, IT principle observed or per protocol analysis Any other risks Low High High Low Indirectness:?1992/2000 guidelines Low Unclear High High: Significant differences in (only real time feedback about CPR outcome quality. Increase enrollment assessor) numbers then stop early. Unclear, some exclusions based on difficultly with airway border on deviation from IT analysis. Outcomes to which these assessments apply All All Overall risk of bias for outcome(s) for study** High High
70 70 Risk of Bias in studies table: ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Study Wolcke 2003, 2201 ITD+ACD vs SCPR Aufderheide 2011, 301 ITD+ACD vs SCPR Random -ization Allocation concealment Blinding Loss to follow-up, IT principle observed or per protocol analysis Any other risks Low High High Low Indirectness:?1992/2000 guidelines Low Unclear High High: Significant differences in (only real time feedback about CPR outcome quality. Increase enrollment assessor) numbers then stop early. Unclear, some exclusions based on difficultly with airway border on deviation from IT analysis. Outcomes to which these assessments apply All All Overall risk of bias for outcome(s) for study** High High
71 71 Risk of Bias in studies table: ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Study Wolcke 2003, 2201 ITD+ACD vs SCPR Aufderheide 2011, 301 ITD+ACD vs SCPR Random -ization Allocation concealment Blinding Loss to follow-up, IT principle observed or per protocol analysis Any other risks Low High High Low Indirectness:?1992/2000 guidelines Low Unclear High High: Significant differences in (only real time feedback about CPR outcome quality. Increase enrollment assessor) numbers then stop early. Unclear, some exclusions based on difficultly with airway border on deviation from IT analysis. Outcomes to which these assessments apply All All Overall risk of bias for outcome(s) for study** High High
72 72 Risk of Bias in studies table: ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Study Wolcke 2003, 2201 ITD+ACD vs SCPR Aufderheide 2011, 301 ITD+ACD vs SCPR Random -ization Allocation concealment Blinding Loss to follow-up, IT principle observed or per protocol analysis Any other risks Low High High Low Indirectness:?1992/2000 guidelines Low Unclear High High: Significant differences in (only real time feedback about CPR outcome quality. Increase enrollment assessor) numbers then stop early. Unclear, some exclusions based on difficultly with airway border on deviation from IT analysis. Outcomes to which these assessments apply All All Overall risk of bias for outcome(s) for study** High High
73 73 Next create an Evidence Profile table
74 Evidence profile table: 74 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) Outcome 2 Survival to hospital discharge Critical (8) No of studies Author Year 1 st page 1 Aufderheide Aufderheide Wolcke Study Design RCT RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious No serious No serious Serious (Wolcke : 1992/2000 guidelines) Serious (ARR CI overlap 1%) Serious (ARR CI overlap 1%) Undetected (sponsor involvement). More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Undetected (sponsor involvement) More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias and imprecision) Low (rated down for risk of bias, indirectness and imprecision)
75 Evidence profile table: 75 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) Outcome 2 Survival to hospital discharge Critical (8) No of studies Author Year 1 st page 1 Aufderheide Aufderheide Wolcke Study Design RCT RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious No serious No serious Serious (Wolcke : 1992/2000 guidelines) Serious (ARR CI overlap 1%) Serious (ARR CI overlap 1%) Undetected (sponsor involvement). More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Undetected (sponsor involvement) More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias and imprecision) Low (rated down for risk of bias, indirectness and imprecision)
76 Evidence profile table: 76 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) No of studies Author Year 1 st page 1 Aufderheide Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious No serious Serious (ARR CI overlap 1%) Undetected (sponsor involvement). More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias and imprecision)
77 Evidence profile table: 77 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) No of studies Author Year 1 st page 1 Aufderheide Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious No serious Serious (ARR CI overlap 1%) Undetected (sponsor involvement). More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias and imprecision)
78 Evidence profile table: 78 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) No of studies Author Year 1 st page 1 Aufderheide Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious No serious Serious (ARR CI overlap 1%) Undetected (sponsor involvement). More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias and imprecision)
79 Evidence profile table: 79 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) No of studies Author Year 1 st page 1 Aufderheide Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious No serious Serious (ARR CI overlap 1%) Undetected (sponsor involvement). More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias and imprecision)
80 Evidence profile table: 80 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) No of studies Author Year 1 st page 1 Aufderheide Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious No serious Serious (ARR CI overlap 1%) Undetected (sponsor involvement). More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias and imprecision)
81 Evidence profile table: 81 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) No of studies Author Year 1 st page 1 Aufderheide Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious No serious Serious (ARR CI overlap 1%) Undetected (sponsor involvement). More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias and imprecision)
82 Evidence profile table: 82 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) No of studies Author Year 1 st page 1 Aufderheide Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious No serious Serious (ARR CI overlap 1%) Undetected (sponsor involvement). More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias and imprecision)
83 Evidence profile table: 83 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) No of studies Author Year 1 st page 1 Aufderheide Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious No serious Serious (ARR CI overlap 1%) Undetected (sponsor involvement). More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias and imprecision)
84 84
85 85
86 Overall quality of evidence: for each key outcome across studies 86
87 Evidence profile table: 87 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) No of studies Author Year 1 st page 1 Aufderheide Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious No serious Serious (ARR CI overlap 1%) Undetected (sponsor involvement). More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias and imprecision)
88 88
89 Evidence profile table: 89 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 2 Survival to hospital discharge Critical (8) No of studies Author Year 1 st page 2 Aufderheide Wolcke Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious Serious (Wolcke : 1992/2000 guidelines) Serious (ARR CI overlap 1%) Undetected (sponsor involvement) More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias, indirectness and imprecision)
90 Evidence profile table: 90 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 2 Survival to hospital discharge Critical (8) No of studies Author Year 1 st page 2 Aufderheide Wolcke Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious Serious (Wolcke : 1992/2000 guidelines) Serious (ARR CI overlap 1%) Undetected (sponsor involvement) More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias, indirectness and imprecision)
91 Evidence profile table: 91 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 2 Survival to hospital discharge Critical (8) No of studies Author Year 1 st page 2 Aufderheide Wolcke Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious Serious (Wolcke : 1992/2000 guidelines) Serious (ARR CI overlap 1%) Undetected (sponsor involvement) More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias, indirectness and imprecision)
92 Evidence profile table: 92 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 2 Survival to hospital discharge Critical (8) No of studies Author Year 1 st page 2 Aufderheide Wolcke Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious Serious (Wolcke : 1992/2000 guidelines) Serious (ARR CI overlap 1%) Undetected (sponsor involvement) More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias, indirectness and imprecision)
93 Evidence profile table: 93 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 2 Survival to hospital discharge Critical (8) No of studies Author Year 1 st page 2 Aufderheide Wolcke Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious Serious (Wolcke : 1992/2000 guidelines) Serious (ARR CI overlap 1%) Undetected (sponsor involvement) More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias, indirectness and imprecision)
94 Evidence profile table: 94 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 2 Survival to hospital discharge Critical (8) No of studies Author Year 1 st page 2 Aufderheide Wolcke Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious Serious (Wolcke : 1992/2000 guidelines) Serious (ARR CI overlap 1%) Undetected (sponsor involvement) More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias, indirectness and imprecision)
95 Evidence profile table: 95 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 2 Survival to hospital discharge Critical (8) No of studies Author Year 1 st page 2 Aufderheide Wolcke Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious Serious (Wolcke : 1992/2000 guidelines) Serious (ARR CI overlap 1%) Undetected (sponsor involvement) More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias, indirectness and imprecision)
96 Evidence profile table: 96 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 2 Survival to hospital discharge Critical (8) No of studies Author Year 1 st page 2 Aufderheide Wolcke Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious Serious (Wolcke : 1992/2000 guidelines) Serious (ARR CI overlap 1%) Undetected (sponsor involvement) More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias, indirectness and imprecision)
97 Evidence profile table: 97 ITD+ACDCPR vs Standard CPR Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Population: Patients in cardiac arrest Settings: OOHCA Intervention: Impedance Threshold Device + Active Compression Decompression CPR Comparison: Standard CPR Outcome Outcome 2 Survival to hospital discharge Critical (8) No of studies Author Year 1 st page 2 Aufderheide Wolcke Study Design RCT Risk of bias* Very serious (blinding, feedback about CPR quality, exclusions/ IT analysis) Inconsistency* Indirectness* Imprecision* Other (including publication bias)** No serious Serious (Wolcke : 1992/2000 guidelines) Serious (ARR CI overlap 1%) Undetected (sponsor involvement) More pulmonary oedema I 94/840 (11%) vs C 62/813 (7%) Quality of evidence for outcome*** Low (rated down for risk of bias, indirectness and imprecision)
98 98 Next create a summary of findings table
99 99
100 100 Summary of findings table(s) Present a key summary graph or table Citation #1 Citation #2
101 101 Summary of findings table: 1 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) 47/813 (5.8%) 75/840 (8.9%) Difference 3.15% (0.64 to 5.66) NNT 31.8 OR 1.60 (1.09 to 2.33) 2470 (1)** Low1 Unblinded study with unbalanced control for quality of CPR.
102 102 Summary of findings table: 1 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) 47/813 (5.8%) 75/840 (8.9%) Difference 3.15% (0.64 to 5.66) NNT 31.8 OR 1.60 (1.09 to 2.33) 2470 (1)** Low1 Unblinded study with unbalanced control for quality of CPR.
103 103 Summary of findings table: 1 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) 47/813 (5.8%) 75/840 (8.9%) Difference 3.15% (0.64 to 5.66) NNT 31.8 OR 1.60 (1.09 to 2.33) 2470 (1)** Low1 Unblinded study with unbalanced control for quality of CPR.
104 104 Summary of findings table: 1 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) 47/813 (5.8%) 75/840 (8.9%) Difference 3.15% (0.64 to 5.66) NNT 31.8 OR 1.60 (1.09 to 2.33) 2470 (1)** Low1 Unblinded study with unbalanced control for quality of CPR.
105 105 Summary of findings table: 1 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) 47/813 (5.8%) 75/840 (8.9%) Difference 3.15% (0.64 to 5.66) NNT 31.8 OR 1.60 (1.09 to 2.33) 2470 (1)** Low1 Unblinded study with unbalanced control for quality of CPR.
106 106 Summary of findings table: 1 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) 47/813 (5.8%) 75/840 (8.9%) Difference 3.15% (0.64 to 5.66) NNT 31.8 OR 1.60 (1.09 to 2.33) 2470 (1)** Low1 Unblinded study with unbalanced control for quality of CPR.
107 107 Summary of findings table: 1 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) 47/813 (5.8%) 75/840 (8.9%) Difference 3.15% (0.64 to 5.66) NNT 31.8 OR 1.60 (1.09 to 2.33) 2470 (1)** Low1 Unblinded study with unbalanced control for quality of CPR.
108 108 Summary of findings table: 1 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) 47/813 (5.8%) 75/840 (8.9%) Difference 3.15% (0.64 to 5.66) NNT 31.8 OR 1.60 (1.09 to 2.33) 2470 (1)** Low1 Unblinded study with unbalanced control for quality of CPR.
109 109 Summary of findings table: 1 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) 47/813 (5.8%) 75/840 (8.9%) Difference 3.15% (0.64 to 5.66) NNT 31.8 OR 1.60 (1.09 to 2.33) 2470 (1)** Low1 Unblinded study with unbalanced control for quality of CPR.
110 110 Summary of findings table: 1 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 1 Neurologically intact survival (survival to hospital discharge with modified Rankin 3) Critical (9) 47/813 (5.8%) 75/840 (8.9%) Difference 3.15% (0.64 to 5.66) NNT 31.8 OR 1.60 (1.09 to 2.33) 2470 (1)** Low1 Unblinded study with unbalanced control for quality of CPR.
111 111 Summary of findings table: 2 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 2 Survival to hospital discharge Critical (8) 94/920 (10.2%) 123/943 (13%) Difference 2.83% (-0.08 to 5.73) NNT 35.4 OR 1.32 (0.99 to 1.75) 2680 (2)*** Low1 Unblinded studies with unbalanced control for quality of CPR.
112 112 Summary of findings table: 2 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 2 Survival to hospital discharge Critical (8) 94/920 (10.2%) 123/943 (13%) Difference 2.83% (-0.08 to 5.73) NNT 35.4 OR 1.32 (0.99 to 1.75) 2680 (2)*** Low1 Unblinded studies with unbalanced control for quality of CPR.
113 113 Summary of findings table: 2 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 2 Survival to hospital discharge Critical (8) 94/920 (10.2%) 123/943 (13%) Difference 2.83% (-0.08 to 5.73) NNT 35.4 OR 1.32 (0.99 to 1.75) 2680 (2)*** Low1 Unblinded studies with unbalanced control for quality of CPR.
114 114 Summary of findings table: 2 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 2 Survival to hospital discharge Critical (8) 94/920 (10.2%) 123/943 (13%) Difference 2.83% (-0.08 to 5.73) NNT 35.4 OR 1.32 (0.99 to 1.75) 2680 (2)*** Low1 Unblinded studies with unbalanced control for quality of CPR.
115 115 Summary of findings table: 2 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 2 Survival to hospital discharge Critical (8) 94/920 (10.2%) 123/943 (13%) Difference 2.83% (-0.08 to 5.73) NNT 35.4 OR 1.32 (0.99 to 1.75) 2680 (2)*** Low1 Unblinded studies with unbalanced control for quality of CPR.
116 116 Summary of findings table: 2 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 2 Survival to hospital discharge Critical (8) 94/920 (10.2%) 123/943 (13%) Difference 2.83% (-0.08 to 5.73) NNT 35.4 OR 1.32 (0.99 to 1.75) 2680 (2)*** Low1 Unblinded studies with unbalanced control for quality of CPR.
117 117 Summary of findings table: 2 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 2 Survival to hospital discharge Critical (8) 94/920 (10.2%) 123/943 (13%) Difference 2.83% (-0.08 to 5.73) NNT 35.4 OR 1.32 (0.99 to 1.75) 2680 (2)*** Low1 Unblinded studies with unbalanced control for quality of CPR.
118 118 Summary of findings table: 2 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 2 Survival to hospital discharge Critical (8) 94/920 (10.2%) 123/943 (13%) Difference 2.83% (-0.08 to 5.73) NNT 35.4 OR 1.32 (0.99 to 1.75) 2680 (2)*** Low1 Unblinded studies with unbalanced control for quality of CPR.
119 119 Summary of findings table: 2 Topic title: Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) Patient or population: Patients in cardiac arrest Settings: OOHCA Intervention: Use of Impedance Threshold Device in addition to Active Compression Decompression CPR Comparison: Use of Standard CPR Outcomes Illustrative comparative risks* (95% CI) Assumed risk Comparison Corresponding risk Intervention Relative effector (95% CI) No of Participants (studies) Quality of the evidence (GRADE) Comments Outcome 2 Survival to hospital discharge Critical (8) 94/920 (10.2%) 123/943 (13%) Difference 2.83% (-0.08 to 5.73) NNT 35.4 OR 1.32 (0.99 to 1.75) 2680 (2)*** Low1 Unblinded studies with unbalanced control for quality of CPR.
120 120 So what might a 2015 COS statement look like?
121 121 Consensus on Science statements Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) One RCT enrolling over 2000 OOHCAs [Aufderheide 2011, 301]reported improved neurologically intact survival when the unblinded use of an Impedance Threshold Device and Active Compression Decompression CPR was compared with manual standard CPR. Two RCTs enrolling over 2000 OOHCAs [Aufderheide 2011, 301; Wolcke 2003, 2201] were unable to demonstrate any improvements in survival to hospital discharge when the unblinded use of an Impedance Threshold Device and Active Compression Decompression CPR was compared with manual standard CPR.
122 122 What about a Treatment Recommendation?
123 123 GRADE Strength of Recommendation Strong: the desirable effects of an intervention clearly outweigh the undesirable effects, or clearly do not. Weak: the trade-offs are less certain either because of low quality evidence or because evidence suggests that desirable and undesirable effects are closely balanced.
124 124 So what might a 2015 TR look like?
125 Draft Treatment Recommendations Impedance Threshold Device + Active Compression Decompression CPR (I) vs Standard CPR (C) There is insufficient evidence to recommend the routine use of the combination of an Impedance Threshold Device and manual active compression decompression cardiopulmonary resuscitation instead of standard CPR (weak recommendation, low quality of evidence).



 Strong or weak (strength) By considering:")
 Rate")

126 Grade down Grade up 126 RCT start high, obs. data start low P I C O Outcome Outcome Outcome Outcome Systematic review Critical Critical Important Not Summary of findings & estimate of effect for each outcome High Moderate Low Very low 1. Risk of bias 2. Inconsistency 3. Indirectness 4. Imprecision 5. Publication bias 1. Large effect 2. Dose response 3. Confounders Guideline development Formulate recommendations: For or against (direction) Strong or weak (strength) By considering: Quality of evidence Balance benefits/harms Values and preferences Revise if necessary by considering: Resource use (cost) Rate overall quality of evidence across outcomes based on lowest quality of critical outcomes We recommend using We suggest using We recommend against using We suggest against using
127 Journals Journal of Clinical Epidemiology (2011-2) 12 articles (more to come in series) extensive review, major reference for GRADE methodology BMJ Series (2008) 7 articles initial concepts of GRADE and justification documents Multiple other publications 127
128 128 Online resources Provides numerous webinars, videos, Powerpoint s, and PDFs on the topic of GRADE. General website for all things GRADE Pro: video at site provides 10 minute quick review Con: lacking an executive summary or user guides as have been created for other User Guides to the Medical Literature Software and PDF website Pro: provides both software and PDF tools Con: unknown usability at this point Online tool available to reviewers. Pro: thorough and compreshensive Con: difficult to navigate through

129 ster.ca/ 129
How might GRADE work for ILCOR? Summary of specific components of GRADE using example worksheet
 1 How might GRADE work for ILCOR? Summary of specific components of GRADE using example worksheet Associate Professor Peter Morley Director Medical Education Royal Melbourne Hospital University of Melbourne
1 How might GRADE work for ILCOR? Summary of specific components of GRADE using example worksheet Associate Professor Peter Morley Director Medical Education Royal Melbourne Hospital University of Melbourne
ANZCOR Guideline 6 Compressions
 ANZCOR Guideline 6 Compressions Who does this guideline apply to? Summary This guideline applies to all persons who are unresponsive and not breathing normally. Who is the audience for this guideline?
ANZCOR Guideline 6 Compressions Who does this guideline apply to? Summary This guideline applies to all persons who are unresponsive and not breathing normally. Who is the audience for this guideline?
Academic Grant CPR process monitors provided by Zoll. conflict of interest to declare
 Comparison of Bystander Fatigue and CPR Quality when Using Ui Continuous Chest Compressions Versus 30:2 Compressions to Ventilations: A Randomized Cross over over Trial CAEP Niagara Falls 2012 CAEP St
Comparison of Bystander Fatigue and CPR Quality when Using Ui Continuous Chest Compressions Versus 30:2 Compressions to Ventilations: A Randomized Cross over over Trial CAEP Niagara Falls 2012 CAEP St
2015 Guidelines Summary HeartSine samaritan PAD Automated External Defibrillators
 2015 Guidelines Summary HeartSine samaritan PAD Automated External Defibrillators This document provides a summary of the 2015 guidelines and how the HeartSine samaritan PAD range of products complies
2015 Guidelines Summary HeartSine samaritan PAD Automated External Defibrillators This document provides a summary of the 2015 guidelines and how the HeartSine samaritan PAD range of products complies
CPR Quality During OHCA Transport
 CPR Quality During OHCA Transport Sheldon Cheskes, MD CCFP(EM) FCFP Medical Director, Sunnybrook Centre for Prehospital Medicine Associate Professor, Division of Emergency Medicine, University of Toronto
CPR Quality During OHCA Transport Sheldon Cheskes, MD CCFP(EM) FCFP Medical Director, Sunnybrook Centre for Prehospital Medicine Associate Professor, Division of Emergency Medicine, University of Toronto
Enhancing 4 th chain: Mechanical chest compression during transportation
 How to Implement New Resuscitation Guidelines Enhancing 4 th chain: Mechanical chest compression during transportation 한림대의료원강동성심병원응급의학과조영석 Contents The Present of Mechanical CPR Device Barriers of High
How to Implement New Resuscitation Guidelines Enhancing 4 th chain: Mechanical chest compression during transportation 한림대의료원강동성심병원응급의학과조영석 Contents The Present of Mechanical CPR Device Barriers of High
On-Scene Resuscitation. Brent Myers, MD MPH Director Medical Director Wake County EMS, Raleigh, NC
 L MODULE 7 On-Scene Resuscitation Brent Myers, MD MPH Director Medical Director Wake County EMS, Raleigh, NC Plan For Discussion: Rationale for EMS Providers On-Scene Resuscitation Choreography Check lists
L MODULE 7 On-Scene Resuscitation Brent Myers, MD MPH Director Medical Director Wake County EMS, Raleigh, NC Plan For Discussion: Rationale for EMS Providers On-Scene Resuscitation Choreography Check lists
Termination of Resuscitation in the Prehospital Setting
 Resuscitation Outcomes Consortium Termination of Resuscitation in the Prehospital Setting Mr. Ian R Drennan ACP BScHK PhD(c) Rescu, Li Ka Shing Knowledge Institute, St. Michael s Hospital Institute of
Resuscitation Outcomes Consortium Termination of Resuscitation in the Prehospital Setting Mr. Ian R Drennan ACP BScHK PhD(c) Rescu, Li Ka Shing Knowledge Institute, St. Michael s Hospital Institute of
U.S. Lifeguard Standards: A Lifeguarding Practice Research Synopsis Mike Espino
 U.S. Lifeguard Standards: A Lifeguarding Practice Research Synopsis Mike Espino Mike is the Aquatics Safety and Risk Specialist for the YMCA of the USA. Previous to joining the YMCA of the USA, he was
U.S. Lifeguard Standards: A Lifeguarding Practice Research Synopsis Mike Espino Mike is the Aquatics Safety and Risk Specialist for the YMCA of the USA. Previous to joining the YMCA of the USA, he was
Hot Topics in Telephone CPR
 Hot Topics in Telephone CPR Bentley J. Bobrow, MD, FACEP Professor, Emergency Medicine Maricopa Medical Center University of Arizona College of Medicine-Phoenix Disclosure PI Arizona HeartRescue Project
Hot Topics in Telephone CPR Bentley J. Bobrow, MD, FACEP Professor, Emergency Medicine Maricopa Medical Center University of Arizona College of Medicine-Phoenix Disclosure PI Arizona HeartRescue Project
EMD CPR. The First First Responder. R. Darrell Nelson, MD, FACEP. Emergency Medicine Wake Forest University Baptist Health
 EMD CPR The First First Responder R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Baptist Health The First, First Responder Objectives 1. Why does EMD matter? 2. Review Role of EMD
EMD CPR The First First Responder R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Baptist Health The First, First Responder Objectives 1. Why does EMD matter? 2. Review Role of EMD
EMD CPR. The First First Responder. R. Darrell Nelson, MD, FACEP
 EMD CPR The First First Responder R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Baptist Health Medical Director, Davie and Stokes County EMS Assistant Medical Director, Forsyth
EMD CPR The First First Responder R. Darrell Nelson, MD, FACEP Emergency Medicine Wake Forest University Baptist Health Medical Director, Davie and Stokes County EMS Assistant Medical Director, Forsyth
What is the Role of Chest Compression Depth during Out-of-Hospital CPR?
 Resuscitation Outcomes Consortium What is the Role of Chest Compression Depth during Out-of-Hospital CPR? Ian Stiell for The ROC Investigators Co-Authors Ian Stiell University of Ottawa Siobhan Everson-Stewart
Resuscitation Outcomes Consortium What is the Role of Chest Compression Depth during Out-of-Hospital CPR? Ian Stiell for The ROC Investigators Co-Authors Ian Stiell University of Ottawa Siobhan Everson-Stewart
Abstract. Keywords. Kyoko Tsukigase 1, Hideharu Tanaka 1,2, Hiroshi Takyu 2
 World Journal of Cardiovascular Diseases, 2017, 7, 185-194 http://www.scirp.org/journal/wjcd ISSN Online: 2164-5337 ISSN Print: 2164-5329 Mismatch between Sites of Incidence of Out-of-Hospital Cardiac
World Journal of Cardiovascular Diseases, 2017, 7, 185-194 http://www.scirp.org/journal/wjcd ISSN Online: 2164-5337 ISSN Print: 2164-5329 Mismatch between Sites of Incidence of Out-of-Hospital Cardiac
High Quality CPR: Demonstration and Analysis. Conflict of Interest (COI)
") High Quality CPR: Demonstration and Analysis Ankur Doshi, MD, Emergency Medicine, University of Pittsburgh Mark Pinchalk, MS, EMT-P, Patient Care Coordinator, Pittsburgh EMS Robin Roberts, Sr. Account
High Quality CPR: Demonstration and Analysis Ankur Doshi, MD, Emergency Medicine, University of Pittsburgh Mark Pinchalk, MS, EMT-P, Patient Care Coordinator, Pittsburgh EMS Robin Roberts, Sr. Account
SUPPLEMENTARY APPENDIX. Ary Serpa Neto MD MSc, Fabienne D Simonis MD, Carmen SV Barbas MD PhD, Michelle Biehl MD, Rogier M Determann MD PhD, Jonathan
 1 LUNG PROTECTIVE VENTILATION WITH LOW TIDAL VOLUMES AND THE OCCURRENCE OF PULMONARY COMPLICATIONS IN PATIENTS WITHOUT ARDS: a systematic review and individual patient data metaanalysis SUPPLEMENTARY APPENDIX
1 LUNG PROTECTIVE VENTILATION WITH LOW TIDAL VOLUMES AND THE OCCURRENCE OF PULMONARY COMPLICATIONS IN PATIENTS WITHOUT ARDS: a systematic review and individual patient data metaanalysis SUPPLEMENTARY APPENDIX
Evidence Summary Recommendations for Pediatric Prehospital Protocols
 Evidence Summary Recommendations for Pediatric Prehospital Protocols Emergency Medical Services for Children State Partnership Purpose To provide summaries of existing evidence to address clinically-relevant
Evidence Summary Recommendations for Pediatric Prehospital Protocols Emergency Medical Services for Children State Partnership Purpose To provide summaries of existing evidence to address clinically-relevant
 Introduction Welcome to COMPREHENSIVE BASIC LIFE SUPPORT Course. BLS is the foundation for saving lives after cardiac arrest. You will learn the skills of highquality cardiopulmonary resuscitation (CPR)
Introduction Welcome to COMPREHENSIVE BASIC LIFE SUPPORT Course. BLS is the foundation for saving lives after cardiac arrest. You will learn the skills of highquality cardiopulmonary resuscitation (CPR)
Resuscitation Council of Southern Africa
 Resuscitation Council of Southern Africa 72 Sophia Street, Fairland, 2170, Johannesburg, South Africa Tel: 011-478-3989 Fax: 011-678-5087 www.resuscitationcouncil.co.za 30 November 2009 PLEA TO THE SOUTH
Resuscitation Council of Southern Africa 72 Sophia Street, Fairland, 2170, Johannesburg, South Africa Tel: 011-478-3989 Fax: 011-678-5087 www.resuscitationcouncil.co.za 30 November 2009 PLEA TO THE SOUTH
Triage Using Telemedicine: Advancements in Prehospital Stroke Care
 Triage Using Telemedicine: Advancements in Prehospital Stroke Care Prasanthi Govindarajan MD, MAS Associate Professor of Emergency Medicine Stanford University Medical Center Disclosures American Heart/Stroke
Triage Using Telemedicine: Advancements in Prehospital Stroke Care Prasanthi Govindarajan MD, MAS Associate Professor of Emergency Medicine Stanford University Medical Center Disclosures American Heart/Stroke
1/9/2015. Red Flags in Prehospital Airway Management. H. Wang, MD 1. Red Flags in Prehospital Airway Management. Disclosures. The Current Standard
 Red Flags in Prehospital Airway Henry E. Wang, MD, MS Professor and Vice Chair for Research Department of Emergency Medicine University of Alabama at Birmingham Disclosures NIH Grant Support UH2-HL125163
Red Flags in Prehospital Airway Henry E. Wang, MD, MS Professor and Vice Chair for Research Department of Emergency Medicine University of Alabama at Birmingham Disclosures NIH Grant Support UH2-HL125163
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY REFERENCE NO. 474
 SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY REFERENCE NO. 474 PURPOSE: To establish the requirements and responsibilities of an S-SV approved EMT / Public Safety Automatic External Defibrillation
SIERRA-SACRAMENTO VALLEY EMS AGENCY PROGRAM POLICY REFERENCE NO. 474 PURPOSE: To establish the requirements and responsibilities of an S-SV approved EMT / Public Safety Automatic External Defibrillation
Ain't Nobody Got Time for That Epi, Fool: ACLS in the 20-Teens Comes of Age Disclosures Updated Syllabus
 Ain't Nobody Got Time for That Epi, Fool: ACLS in the 20-Teens Comes of Age JASON PERSOFF, MD, SFHM UNIVERSITY OF COLORADO HOSPITAL MEDICINE GROUP Disclosures Nothing to disclose Will present topics that
Ain't Nobody Got Time for That Epi, Fool: ACLS in the 20-Teens Comes of Age JASON PERSOFF, MD, SFHM UNIVERSITY OF COLORADO HOSPITAL MEDICINE GROUP Disclosures Nothing to disclose Will present topics that
Avalanche Victim Resuscitation Checklist
 Avalanche Victim Resuscitation Checklist Changing process for saving lives ICAR MEDCOM: Kottmann A, Blancher M, Boyd J, Spichiger T, Brugger H Dr A. Kottmann Avalanche Time Hazard Life or death Stressfull
Avalanche Victim Resuscitation Checklist Changing process for saving lives ICAR MEDCOM: Kottmann A, Blancher M, Boyd J, Spichiger T, Brugger H Dr A. Kottmann Avalanche Time Hazard Life or death Stressfull
European EMS Championship Rules
 Telegrafvej 5 DK-2750 Ballerup EMS2018@regionh.dk Follow us on Twitter: @European_EMS #EMS2018 Date: 5 September 2017 European EMS Championship Rules Location Tivoli Hotel & Congress Center, Copenhagen,
Telegrafvej 5 DK-2750 Ballerup EMS2018@regionh.dk Follow us on Twitter: @European_EMS #EMS2018 Date: 5 September 2017 European EMS Championship Rules Location Tivoli Hotel & Congress Center, Copenhagen,
Pediatric Hospice Patients
 Page 1 APPROVED: EMS Medical Director EMS Administrator 1. Purpose 1.1 To establish procedures for prehospital personnel to recognize and follow modified Do Not Resuscitate (DNR) directives and other specific
Page 1 APPROVED: EMS Medical Director EMS Administrator 1. Purpose 1.1 To establish procedures for prehospital personnel to recognize and follow modified Do Not Resuscitate (DNR) directives and other specific
McHENRY WESTERN LAKE COUNTY EMS SYSTEM FALL 2014 CONTINUING EDUCATION MANDATORY FOR ALL PRIMARY AND PROBATIONARY ALS SYSTEM PROVIDERS.
 McHENRY WESTERN LAKE COUNTY EMS SYSTEM FALL 2014 CONTINUING EDUCATION MANDATORY FOR ALL PRIMARY AND PROBATIONARY ALS SYSTEM PROVIDERS ResQPOD In a cardiac arrest blood flow to the organs stop. Key to survival
McHENRY WESTERN LAKE COUNTY EMS SYSTEM FALL 2014 CONTINUING EDUCATION MANDATORY FOR ALL PRIMARY AND PROBATIONARY ALS SYSTEM PROVIDERS ResQPOD In a cardiac arrest blood flow to the organs stop. Key to survival
UTSW/BioTel EMS System Training Bulletin June 1, 2015 EMS TB Adult CPR Update: Change to Continuous Chest Compressions (CCC)
") UTSW/BioTel EMS System Training Bulletin June 1, 2015 EMS TB 15-005 Adult CPR Update: Change to Continuous Chest Compressions (CCC) 06/01/2015 FINAL-BioTel 1 Purpose To set forth updated ADULT CPR practice
UTSW/BioTel EMS System Training Bulletin June 1, 2015 EMS TB 15-005 Adult CPR Update: Change to Continuous Chest Compressions (CCC) 06/01/2015 FINAL-BioTel 1 Purpose To set forth updated ADULT CPR practice
COCHRANE CORNER. The development of an updated prehospital search filter for the Cochrane Library: Prehospital Search Filter Version 2.
 ISSN 1447-4999 COCHRANE CORNER The development of an updated prehospital search filter for the Cochrane Library: Prehospital Search Filter Version 2.0 Stephen Burgess, Erin Smith, Sarah Piper, Frank Archer
ISSN 1447-4999 COCHRANE CORNER The development of an updated prehospital search filter for the Cochrane Library: Prehospital Search Filter Version 2.0 Stephen Burgess, Erin Smith, Sarah Piper, Frank Archer
CPR competition 2016 Rules. The ERC Congress on Education. Reykjavik, Iceland
 CPR competition 2016 Rules The ERC Congress on Education Reykjavik, Iceland Location Prague Congress Centre, Prague, Czech Republic Timing Preliminary round : Saturday 24 th September 2016 Final: Sunday
CPR competition 2016 Rules The ERC Congress on Education Reykjavik, Iceland Location Prague Congress Centre, Prague, Czech Republic Timing Preliminary round : Saturday 24 th September 2016 Final: Sunday
MRC Academy November 4, 2013 Kevin Sipprell MD EMS Medical Director Ridgeview Ambulance DISPATCH ASSISTED CPR
 MRC Academy November 4, 2013 Kevin Sipprell MD EMS Medical Director Ridgeview Ambulance DISPATCH ASSISTED CPR Objectives The importance of dispatch assistance Keys to success Perceived barriers to performing
MRC Academy November 4, 2013 Kevin Sipprell MD EMS Medical Director Ridgeview Ambulance DISPATCH ASSISTED CPR Objectives The importance of dispatch assistance Keys to success Perceived barriers to performing
2005 Top Ten Major Changes in Treatment Recommendations *
 2005 Top Ten Major Changes in Treatment Recommendations * This document reviews the top ten new treatment recommendations and guidelines for ASHI s basic life support training programs for professional
2005 Top Ten Major Changes in Treatment Recommendations * This document reviews the top ten new treatment recommendations and guidelines for ASHI s basic life support training programs for professional
Emergency Life Support (ELS) Course
 Course") V1 Approved by Resuscitation Committee - July 2018 Course Resuscitation Services UK Ltd Topics The ABCDE Approach Handout, Podcast & Scenario teaching/assessment Medical Emergency conditions Slide set
V1 Approved by Resuscitation Committee - July 2018 Course Resuscitation Services UK Ltd Topics The ABCDE Approach Handout, Podcast & Scenario teaching/assessment Medical Emergency conditions Slide set
Pan-Asian Resuscitation Outcomes Study (PAROS)
") Pan-Asian Resuscitation Outcomes Study (PAROS) Page 1 of 6 Case number Mode of Transportation #1 Patient brought in by 1 EMS 2 Non-EMS If Non-EMS, please specify 1 Private ambulance 2 Own/Private transport
Pan-Asian Resuscitation Outcomes Study (PAROS) Page 1 of 6 Case number Mode of Transportation #1 Patient brought in by 1 EMS 2 Non-EMS If Non-EMS, please specify 1 Private ambulance 2 Own/Private transport
MANAGEMENT OF COLLAPSED ADULT PATIENT
 MANAGEMENT OF COLLAPSED ADULT PATIENT Author Information Dr. Venugopalan P.P. Chief Emergency Medicine Dy Director, MIMS Academy Malabar Institute of Medical Sciences Ltd. P.O. Govindapuram, Calicut, Kerala
MANAGEMENT OF COLLAPSED ADULT PATIENT Author Information Dr. Venugopalan P.P. Chief Emergency Medicine Dy Director, MIMS Academy Malabar Institute of Medical Sciences Ltd. P.O. Govindapuram, Calicut, Kerala
Safety and Participation Policies 2017
 Safety and Participation Policies 2017 POLICY AND PROCEDURE CHANGES From the Australian Rugby Strategic Plan 2016-2020, under the Pillar Make Rugby a Game for All, Australian Rugby is committed to ensuring
Safety and Participation Policies 2017 POLICY AND PROCEDURE CHANGES From the Australian Rugby Strategic Plan 2016-2020, under the Pillar Make Rugby a Game for All, Australian Rugby is committed to ensuring
Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Cardiac Arrest General This protocol should be followed for all adult cardiac arrests. Medical cardiac arrest patients undergoing attempted resuscitation should not
Date: November 15, 2012 Page 1 of 5 Cardiac Arrest General This protocol should be followed for all adult cardiac arrests. Medical cardiac arrest patients undergoing attempted resuscitation should not
INITIATE APPROPRIATE RESUSCITATION PER POLICY/PROTOCOL
 PATIENT ASSESSMENT ASSURE PATIENT HAS A PATENT AIRWAY LOOK, LISTEN AND FEEL TO CONFIRM APNEA CHECK F PULSE F MINIMUM OF 60 SECONDS TO CONFIRM PULSELESS CHECK PUPILLARY RESPONSE DOES PATIENT MEET OBVIOUS
PATIENT ASSESSMENT ASSURE PATIENT HAS A PATENT AIRWAY LOOK, LISTEN AND FEEL TO CONFIRM APNEA CHECK F PULSE F MINIMUM OF 60 SECONDS TO CONFIRM PULSELESS CHECK PUPILLARY RESPONSE DOES PATIENT MEET OBVIOUS
Basic Life Support (BLS)
") Basic Life Support (BLS) Basic Life Support (BLS) is the foundation for saving lives after cardiac arrest. Participant will learn the skills of high-quality cardiopulmonary resuscitation (CPR) for victims
Basic Life Support (BLS) Basic Life Support (BLS) is the foundation for saving lives after cardiac arrest. Participant will learn the skills of high-quality cardiopulmonary resuscitation (CPR) for victims
Peter J. Kudenchuk, MD University of Washington
 Peter J. Kudenchuk, MD University of Washington CPR-The Science Behind the Hands A/Prof Marcus Ong Senior Consultant, Clinician Scientist & Director of Research Department of Emergency Medicine Singapore
Peter J. Kudenchuk, MD University of Washington CPR-The Science Behind the Hands A/Prof Marcus Ong Senior Consultant, Clinician Scientist & Director of Research Department of Emergency Medicine Singapore
Supplementary Online Content
 Supplementary Online Content McEvoy JP, Byerly M, Hamer RM, et al. Effectiveness of Paliperidone Palmitate vs Haloperidol Decanoate for Maintenance Treatment of Schizophrenia: a Randomized Clinical Trial.
Supplementary Online Content McEvoy JP, Byerly M, Hamer RM, et al. Effectiveness of Paliperidone Palmitate vs Haloperidol Decanoate for Maintenance Treatment of Schizophrenia: a Randomized Clinical Trial.
Exposure-adjusted fatality rates for cycling and walking in European countries
 Epidemiology, Biostatistics and Prevention Institute Exposure-adjusted fatality rates for cycling and walking in European countries Alberto Castro Sonja Kahlmeier Thomas Götschi University of Zurich, Epidemiology
Epidemiology, Biostatistics and Prevention Institute Exposure-adjusted fatality rates for cycling and walking in European countries Alberto Castro Sonja Kahlmeier Thomas Götschi University of Zurich, Epidemiology
Alpine Trauma Registry
 Alpine Trauma Registry Giacomo Strapazzon MD PhD EURAC Institute of Mountain Emergency Medicine, Italy CNSAS Italian Alpine and Cave Rescue Team, Italy ICAR-CISA General Assembly Bol, Croatia 2013 OBJECTIVE
Alpine Trauma Registry Giacomo Strapazzon MD PhD EURAC Institute of Mountain Emergency Medicine, Italy CNSAS Italian Alpine and Cave Rescue Team, Italy ICAR-CISA General Assembly Bol, Croatia 2013 OBJECTIVE
7.0 DEVIATION and EXCEPTION of a PREVIOUSLY APPROVED PROTOCOL
 7.0 DEVIATION and EXCEPTION of a PREVIOUSLY APPROVED PROTOCOL 7.1 OBJECTIVE To describe the policies and procedures for reviewing a modification or a deviation/exception to a previously approved protocol.
7.0 DEVIATION and EXCEPTION of a PREVIOUSLY APPROVED PROTOCOL 7.1 OBJECTIVE To describe the policies and procedures for reviewing a modification or a deviation/exception to a previously approved protocol.
Lima 2019 Pan American Games Internal Nomination Process: Triathlon
 Lima 2019 Pan American Games Internal Nomination Process: Triathlon A. Introduction This document outlines the qualification and nomination procedures (the Nomination Process ) of Triathlon Canada for
Lima 2019 Pan American Games Internal Nomination Process: Triathlon A. Introduction This document outlines the qualification and nomination procedures (the Nomination Process ) of Triathlon Canada for
Chi è il bystander laico? Come modificare l algoritmo BLS in base al soccorritore. Federico Semeraro Ospedale Maggiore, Bologna
 Chi è il bystander laico? Come modificare l algoritmo BLS in base al soccorritore Federico Semeraro Ospedale Maggiore, Bologna President Italian Resuscitation Council Educational Committee (SEC) BLS co-chair
Chi è il bystander laico? Come modificare l algoritmo BLS in base al soccorritore Federico Semeraro Ospedale Maggiore, Bologna President Italian Resuscitation Council Educational Committee (SEC) BLS co-chair
12/03/2013. Conflict of interest. ERC 2010 Guidelines. Waar is nog winst te behalen in het reanimatieonderwijs?
 Conflict of interest Waar is nog winst te behalen in het reanimatieonderwijs? Unrestricted research grant from the Laerdal Foundation Nicolas MPOTOS Emergency Department, Ghent University Hospital, Belgium
Conflict of interest Waar is nog winst te behalen in het reanimatieonderwijs? Unrestricted research grant from the Laerdal Foundation Nicolas MPOTOS Emergency Department, Ghent University Hospital, Belgium
The Positive Effect of Negative Pressure
 The Positive Effect of Negative Pressure (Future Direction in Resuscitative Care) Brent Parquette, NRP Lucas County EMS, Toledo, OH Toledo, Ohio Lucas County EMS (Toledo, OH) Primary service area: 340
The Positive Effect of Negative Pressure (Future Direction in Resuscitative Care) Brent Parquette, NRP Lucas County EMS, Toledo, OH Toledo, Ohio Lucas County EMS (Toledo, OH) Primary service area: 340
High-Functioning EMS CPR Teams. Sally A Taylor - Paramedic Atlantic Partners EMS
 High-Functioning EMS CPR Teams Cardiac Arrest Management Sally A Taylor - Paramedic Atlantic Partners EMS Insanity: Doing the same thing over and over and expecting a different result. John Dryden The
High-Functioning EMS CPR Teams Cardiac Arrest Management Sally A Taylor - Paramedic Atlantic Partners EMS Insanity: Doing the same thing over and over and expecting a different result. John Dryden The
Neonatal tidal volume targeted ventilation
 Neonatal tidal volume targeted ventilation Colin Morley Retired Professor of Neonatal Medicine, Royal Women s Hospital, Melbourne, Australia. Honorary Visiting Fellow, Dept Obstetrics and Gynaecology,
Neonatal tidal volume targeted ventilation Colin Morley Retired Professor of Neonatal Medicine, Royal Women s Hospital, Melbourne, Australia. Honorary Visiting Fellow, Dept Obstetrics and Gynaecology,
University of Iowa External/Central IRB Reliance Process Standard Operating Procedure (SOP)
") University of Iowa External/Central IRB Reliance Process Standard Operating Procedure (SOP) I. OVERVIEW The purpose of this Standard Operating Procedure is to define a process for all University of Iowa
University of Iowa External/Central IRB Reliance Process Standard Operating Procedure (SOP) I. OVERVIEW The purpose of this Standard Operating Procedure is to define a process for all University of Iowa
Matthew Thomas 1*, Sarah Voss 2, Jonathan Benger 3,4, Kim Kirby 2 and Jerry P. Nolan 5
 Thomas et al. BMC Emergency Medicine (2019) 19:16 https://doi.org/10.1186/s12873-018-0214-1 RESEARCH ARTICLE Open Access Cluster randomised comparison of the effectiveness of 100% oxygen versus titrated
Thomas et al. BMC Emergency Medicine (2019) 19:16 https://doi.org/10.1186/s12873-018-0214-1 RESEARCH ARTICLE Open Access Cluster randomised comparison of the effectiveness of 100% oxygen versus titrated
Pearls for ED Airway Management 12/26/2013
 Red Flags in Prehospital Airway Management Henry E. Wang, MD, MS Associate Professor and Vice Chair for Research Department of Emergency Medicine University of Alabama at Birmingham The Current Standard
Red Flags in Prehospital Airway Management Henry E. Wang, MD, MS Associate Professor and Vice Chair for Research Department of Emergency Medicine University of Alabama at Birmingham The Current Standard
CPR: Are You a Machine or Do You Need One?
 CPR: Are You a Machine or Do You Need One? Outline Mechanical CPR update Are you a machine? Measuring performance ED/hospital challenges When mechanical CPR could make a difference New Guidelines The evidence
CPR: Are You a Machine or Do You Need One? Outline Mechanical CPR update Are you a machine? Measuring performance ED/hospital challenges When mechanical CPR could make a difference New Guidelines The evidence
The Effect of a Seven Week Exercise Program on Golf Swing Performance and Musculoskeletal Screening Scores
 The Effect of a Seven Week Exercise Program on Golf Swing Performance and Musculoskeletal Screening Scores 2017 Mico Hannes Olivier Bachelor of Sport Science Faculty of Health Sciences and Medicine Bond
The Effect of a Seven Week Exercise Program on Golf Swing Performance and Musculoskeletal Screening Scores 2017 Mico Hannes Olivier Bachelor of Sport Science Faculty of Health Sciences and Medicine Bond
Training Presentation. TFD-EMS Ver. 1 09/15
 Training Presentation TFD-EMS Ver. 1 09/15 Agenda ResQCPR System: Definition and Labeling IPR Therapy Physiology of Conventional CPR ResQPOD ITD 16 and Instructions for Use ResQPUMP ACD-CPR Device and
Training Presentation TFD-EMS Ver. 1 09/15 Agenda ResQCPR System: Definition and Labeling IPR Therapy Physiology of Conventional CPR ResQPOD ITD 16 and Instructions for Use ResQPUMP ACD-CPR Device and
1. Review and approval of the consent document is a responsibility that FDA assigns to the IRB with jurisdiction
 Medical College of Wisconsin/Froedtert Hospital Guidance on Negotiating Consent Document Language For Clinical Trial Sponsors 1. Review and approval of the consent document is a responsibility that FDA
Medical College of Wisconsin/Froedtert Hospital Guidance on Negotiating Consent Document Language For Clinical Trial Sponsors 1. Review and approval of the consent document is a responsibility that FDA
Training BULLETIN A Training and Education Update for PADI Members Worldwide
 Training BULLETIN A Training and Education Update for PADI Members Worldwide FIRST QUARTER 2011 Product No. 01220 In This Issue... Dive Theory Online Link to Divemaster 2 Referral Form Notice 2 EANx RDP
Training BULLETIN A Training and Education Update for PADI Members Worldwide FIRST QUARTER 2011 Product No. 01220 In This Issue... Dive Theory Online Link to Divemaster 2 Referral Form Notice 2 EANx RDP
SECOND EUROPEAN CONSENSUS CONFERENCE ON HYPERBARIC MEDICINE THE TREATMENT OF DECOMPRESSION ACCIDENTS IN RECREATIONAL DIVING
 SECOND EUROPEAN CONSENSUS CONFERENCE ON HYPERBARIC MEDICINE THE TREATMENT OF DECOMPRESSION ACCIDENTS IN RECREATIONAL DIVING MARSEILLE, May 8-10, 1996 RECOMMENDATIONS OF THE JURY* QUESTION 1 : Is there
SECOND EUROPEAN CONSENSUS CONFERENCE ON HYPERBARIC MEDICINE THE TREATMENT OF DECOMPRESSION ACCIDENTS IN RECREATIONAL DIVING MARSEILLE, May 8-10, 1996 RECOMMENDATIONS OF THE JURY* QUESTION 1 : Is there
Stroke Outcomes in Australia - five years of AROC data- Tara Stevermuer AROC Data Manager
 Stroke Outcomes in Australia - five years of AROC data- Tara Stevermuer AROC Data Manager Background on Overview AROC FIM & AN-SNAP Rehabilitation outcome measures Profile of stroke rehabilitation episodes
Stroke Outcomes in Australia - five years of AROC data- Tara Stevermuer AROC Data Manager Background on Overview AROC FIM & AN-SNAP Rehabilitation outcome measures Profile of stroke rehabilitation episodes
Update on chest compressions
 Update on chest compressions Georg M Schmölzer Centre for the Studies of Asphyxia and Resuscitation, Royal Alexandra Hospital, Edmonton, Canada; Dept. of Pediatrics, University of Alberta, Edmonton, Canada
Update on chest compressions Georg M Schmölzer Centre for the Studies of Asphyxia and Resuscitation, Royal Alexandra Hospital, Edmonton, Canada; Dept. of Pediatrics, University of Alberta, Edmonton, Canada
2016 EFR CPR & AED Instructor Guide Errata Revision to 12/11 EFR CPR & AED English Instructor Guide (product #79215, English, Vision 1.
 2016 EFR CPR & AED Instructor Guide Errata Revision to 12/11 EFR CPR & AED English Instructor Guide (product #79215, English, Vision 1.0) Cover and inside cover, bottom of page, change version and copyright
2016 EFR CPR & AED Instructor Guide Errata Revision to 12/11 EFR CPR & AED English Instructor Guide (product #79215, English, Vision 1.0) Cover and inside cover, bottom of page, change version and copyright
Ventilating the Sick Lung Mike Dougherty RRT-NPS
 Ventilating the Sick Lung 2018 Mike Dougherty RRT-NPS Goals and Objectives Discuss some Core Principles of Ventilation relevant to mechanical ventilation moving forward. Compare and Contrast High MAP strategies
Ventilating the Sick Lung 2018 Mike Dougherty RRT-NPS Goals and Objectives Discuss some Core Principles of Ventilation relevant to mechanical ventilation moving forward. Compare and Contrast High MAP strategies
UNIVERSITY OF TENNESSEE GRADUATE SCHOOL OF MEDICINE INSTITUTIONAL REVIEW BOARD CONTINUING REVIEW AND REAPPROVAL OF RESEARCH
 UNIVERSITY OF TENNESSEE GRADUATE SCHOOL OF MEDICINE INSTITUTIONAL REVIEW BOARD CONTINUING REVIEW AND REAPPROVAL OF RESEARCH I. PURPOSE This document outlines the required elements of University of Tennessee
UNIVERSITY OF TENNESSEE GRADUATE SCHOOL OF MEDICINE INSTITUTIONAL REVIEW BOARD CONTINUING REVIEW AND REAPPROVAL OF RESEARCH I. PURPOSE This document outlines the required elements of University of Tennessee
Issue in IRB Approvals:
 Issue in IRB Approvals: What are the obligations of investigators and the IRB in maintaining IRB approval? What are the consequences of a lapse in IRB approval? How does the IRB evaluate lapses in approval?
Issue in IRB Approvals: What are the obligations of investigators and the IRB in maintaining IRB approval? What are the consequences of a lapse in IRB approval? How does the IRB evaluate lapses in approval?
SOP 407: PROTOCOL DEVIATIONS AND UNANTICIPATED PROBLEMS
 University of Oklahoma Office of Human Research Participant Protection : PROTOCOL DEVIATIONS AND UNANTICIPATED PROBLEMS 1. POLICY Protocol deviations and unanticipated problems may be discovered in a variety
University of Oklahoma Office of Human Research Participant Protection : PROTOCOL DEVIATIONS AND UNANTICIPATED PROBLEMS 1. POLICY Protocol deviations and unanticipated problems may be discovered in a variety
Lima 2019 Pan American Games Internal Nomination Process: Triathlon
 Lima 2019 Pan American Games Internal Nomination Process: Triathlon A. Introduction This document outlines the qualification and nomination procedures (the Nomination Process ) of Triathlon Canada for
Lima 2019 Pan American Games Internal Nomination Process: Triathlon A. Introduction This document outlines the qualification and nomination procedures (the Nomination Process ) of Triathlon Canada for
EMERGENCY USE 03/02/2016
 DUKE UNIVERSITY HEALTH SYSTEM Human Research Protection Program EMERGENCY USE 03/02/2016 Emergency Exemption for an Investigational Drug or Biologic or Unapproved Device Emergency use of an investigational
DUKE UNIVERSITY HEALTH SYSTEM Human Research Protection Program EMERGENCY USE 03/02/2016 Emergency Exemption for an Investigational Drug or Biologic or Unapproved Device Emergency use of an investigational
TECHNICAL NOTE THROUGH KERBSIDE LANE UTILISATION AT SIGNALISED INTERSECTIONS
 TECHNICAL NOTE THROUGH KERBSIDE LANE UTILISATION AT SIGNALISED INTERSECTIONS Authors: Randhir Karma NDip: Eng (Civil) B. Tech Eng (Civil) M Eng (Hons) (Transportation) Auckland Traffic Service Group Manager
TECHNICAL NOTE THROUGH KERBSIDE LANE UTILISATION AT SIGNALISED INTERSECTIONS Authors: Randhir Karma NDip: Eng (Civil) B. Tech Eng (Civil) M Eng (Hons) (Transportation) Auckland Traffic Service Group Manager
bls guidelines B42EFDD89A9AB6A33D869587D2D61D4E Bls Guidelines 1 / 6
 Bls Guidelines 1 / 6 2 / 6 3 / 6 Bls Guidelines Welcome to the Basic Life Support (BLS) algorithms and training by United Medical Education. Here we will discuss basic life saving interventions for patients
Bls Guidelines 1 / 6 2 / 6 3 / 6 Bls Guidelines Welcome to the Basic Life Support (BLS) algorithms and training by United Medical Education. Here we will discuss basic life saving interventions for patients
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and
 This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution
This article appeared in a journal published by Elsevier. The attached copy is furnished to the author for internal non-commercial research and education use, including for instruction at the authors institution
Corrected FIM effectiveness as an index independent of FIM score on admission
 7 Japanese Journal of Comprehensive Rehabilitation Science (2014) Original Article Corrected FIM effectiveness as an index independent of FIM score on admission Makoto Tokunaga, MD, PhD, 1 Ryoji Nakanishi,
7 Japanese Journal of Comprehensive Rehabilitation Science (2014) Original Article Corrected FIM effectiveness as an index independent of FIM score on admission Makoto Tokunaga, MD, PhD, 1 Ryoji Nakanishi,
Guidelines 2005 for Basic Life Support
 Guidelines 2005 for Basic Life Support Anthony J Handley MD FRCP Chief Medical Adviser RLSS UK Honorary Medical Adviser ILSE Honorary Secretary, Medical Committee ILS Honorary Consultant Physician & Cardiologist,
Guidelines 2005 for Basic Life Support Anthony J Handley MD FRCP Chief Medical Adviser RLSS UK Honorary Medical Adviser ILSE Honorary Secretary, Medical Committee ILS Honorary Consultant Physician & Cardiologist,
Basic Life Support Adult
 1/2.4.1 Version 4, 03/2016 Basic Life Support Adult Collapse If physically unable to ventilate perform compression only CPR Unresponsive and breathing abnormally or gasping 112 / 999 Shout for help 112
1/2.4.1 Version 4, 03/2016 Basic Life Support Adult Collapse If physically unable to ventilate perform compression only CPR Unresponsive and breathing abnormally or gasping 112 / 999 Shout for help 112
THE SYSTEM FOR HIGH-QUALITY CPR
 AutoPulse THE SYSTEM FOR HIGH-QUALITY CPR RESUSCITATION ON THE MOVE Since we had the AutoPulse, we could carry the patient down three flights of stairs while continuing chest compressions. He survived,
AutoPulse THE SYSTEM FOR HIGH-QUALITY CPR RESUSCITATION ON THE MOVE Since we had the AutoPulse, we could carry the patient down three flights of stairs while continuing chest compressions. He survived,
Update on Acute Stroke Management
 Update on Acute Stroke Management ACC Rockies, Banff March 2014 Brian Buck, MD MSc FRCPC Division of Neurology, Department of Medicine University of Alberta Disclosures None relevant to contents of presentation
Update on Acute Stroke Management ACC Rockies, Banff March 2014 Brian Buck, MD MSc FRCPC Division of Neurology, Department of Medicine University of Alberta Disclosures None relevant to contents of presentation
Key statistics from the National Cardiac Arrest Audit 2016/17
 Key statistics from the National Cardiac Arrest Audit 216/17 Supported by Resuscitation Council (UK) and Intensive Care National Audit & Research Centre (ICNARC) Data collection scope (NCAA Version 1.3)
Key statistics from the National Cardiac Arrest Audit 216/17 Supported by Resuscitation Council (UK) and Intensive Care National Audit & Research Centre (ICNARC) Data collection scope (NCAA Version 1.3)
United States Lifeguard Standards Coalition Evidence Review
 United States Lifeguard Standards Coalition Evidence Review On the following pages, you will find a primary question (and in some cases ancillary questions), reviewed by the United States Lifeguard Standards
United States Lifeguard Standards Coalition Evidence Review On the following pages, you will find a primary question (and in some cases ancillary questions), reviewed by the United States Lifeguard Standards
Reading (6*%&-*/& 61%"5& $13 "/% &$$ "-(03*5). 1"$,"(& &TTFOUJBMT GPS )FBMUI 1SPGFTTJPOBMT
. 1$,(& &TTFOUJBMT GPS )FBMUI 1SPGFTTJPOBMT") Reading Introduction On October 15th, 2015 the Heart and Stroke Foundation of Canada (HSFC) released the 2015 Guidelines for Cardio Pulmonary Resuscitation (CPR) and Emergency Cardiac Care (ECC). HSFC
Reading Introduction On October 15th, 2015 the Heart and Stroke Foundation of Canada (HSFC) released the 2015 Guidelines for Cardio Pulmonary Resuscitation (CPR) and Emergency Cardiac Care (ECC). HSFC
2015 CPR and Resuscitation Guidelines Summary of Changes in Lifesaving Society Literature
 2015 CPR and Resuscitation Guidelines Summary of Changes in Lifesaving Society Literature October 2016 Introduction Every five years, the International Liaison Committee on Resuscitation (ILCOR) reviews
2015 CPR and Resuscitation Guidelines Summary of Changes in Lifesaving Society Literature October 2016 Introduction Every five years, the International Liaison Committee on Resuscitation (ILCOR) reviews
CPR & ECC COURSE MATRIX
 CPR & ECC COURSE MATRIX Course Content Audience Student Materials Instructor Materials Course Completion Card Type Estimated Time (Based on 6:1 Student to Instructor Ratio) Courses for Healthcare Professionals
CPR & ECC COURSE MATRIX Course Content Audience Student Materials Instructor Materials Course Completion Card Type Estimated Time (Based on 6:1 Student to Instructor Ratio) Courses for Healthcare Professionals
Promoting Physical Activity Using Walking Poles in Senior Citizens of Southern Vermont's Deerfield Valley Region
 University of Vermont ScholarWorks @ UVM Family Medicine Clerkship Student Projects College of Medicine 2016 Promoting Physical Activity Using Walking Poles in Senior Citizens of Southern Vermont's Deerfield
University of Vermont ScholarWorks @ UVM Family Medicine Clerkship Student Projects College of Medicine 2016 Promoting Physical Activity Using Walking Poles in Senior Citizens of Southern Vermont's Deerfield
Systematic Review and Meta-analysis of Bicycle Helmet Efficacy to Mitigate Head, Face and Neck Injuries
 Systematic Review and Meta-analysis of Bicycle Helmet Efficacy to Mitigate Head, Face and Neck Injuries Prudence Creighton & Jake Olivier MATHEMATICS & THE UNIVERSITY OF NEW STATISTICS SOUTH WALES Creighton
Systematic Review and Meta-analysis of Bicycle Helmet Efficacy to Mitigate Head, Face and Neck Injuries Prudence Creighton & Jake Olivier MATHEMATICS & THE UNIVERSITY OF NEW STATISTICS SOUTH WALES Creighton
Clarification of first aid practices: Position Statement re Control of Bleeding and CPR and Rescue Breaths ASPA Medical Advisory Committee July 2013
 Clarification of first aid practices: Position Statement re Control of Bleeding and CPR and Rescue Breaths ASPA Medical Advisory Committee July 2013 Over the past couple of months some queries have been
Clarification of first aid practices: Position Statement re Control of Bleeding and CPR and Rescue Breaths ASPA Medical Advisory Committee July 2013 Over the past couple of months some queries have been
Guide to Compression-only Bystander CPR
 Guide to Compression-only Bystander CPR The Value of CPR During a cardiac arrest, CardioPulmonary Resuscitation (CPR) is important because it is the best treatment until the arrival of a Defibrillator,
Guide to Compression-only Bystander CPR The Value of CPR During a cardiac arrest, CardioPulmonary Resuscitation (CPR) is important because it is the best treatment until the arrival of a Defibrillator,
A Comparison of American Red Cross- and YMCA-Preferred Approach Methods Used to Rescue Near-Drowning Victims
 International Journal of Aquatic Research and Education Volume 1 Number 1 Article 4 2-1-2007 A Comparison of American Red Cross- and YMCA-Preferred Approach Methods Used to Rescue Near-Drowning Victims
International Journal of Aquatic Research and Education Volume 1 Number 1 Article 4 2-1-2007 A Comparison of American Red Cross- and YMCA-Preferred Approach Methods Used to Rescue Near-Drowning Victims
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
How does the paramedics work day look like? Have a look at our field research video.
 Adrinject Adripod Adrinject and Adripod are designed as a kit to assist paramedics in adrenaline administration during CPR procedures in pre-hospital contexts. Together two products will free up time,
Adrinject Adripod Adrinject and Adripod are designed as a kit to assist paramedics in adrenaline administration during CPR procedures in pre-hospital contexts. Together two products will free up time,
B-CARD NO PAUSE SHOULD BE YOUR CAUSE
 B-CARD NO PAUSE SHOULD BE YOUR CAUSE SIMEU Congress, 17-20 November, Symposium Georges Bousignac 1 Cardiac arrest: A new cutting edge treatment method by Dr. Boussignac No Pause Should Be Your Cause 2
B-CARD NO PAUSE SHOULD BE YOUR CAUSE SIMEU Congress, 17-20 November, Symposium Georges Bousignac 1 Cardiac arrest: A new cutting edge treatment method by Dr. Boussignac No Pause Should Be Your Cause 2
IRB APPLICATION CHECKLIST
 The application for IRB approval may appear daunting at first, but most questions are straightforward. For those that may require some interpretation or specialized knowledge, this guide (which is essentially
The application for IRB approval may appear daunting at first, but most questions are straightforward. For those that may require some interpretation or specialized knowledge, this guide (which is essentially
Evaluation System for Chest Compression Training Shinnosuke-kun
 NEW AREAS Evaluation System for Chest Compression Training Shinnosuke-kun Youta KOKUBO*, Ichinosuke MAEDA, Shingo HIBINO and Kouichirou MINAMI ----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
NEW AREAS Evaluation System for Chest Compression Training Shinnosuke-kun Youta KOKUBO*, Ichinosuke MAEDA, Shingo HIBINO and Kouichirou MINAMI ----------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
Current Status: Active PolicyStat ID: Origination: 04/2018 Effective: 04/2018 Approved: 04/2018 Last Revised: 04/2018 Expiration: 04/2021
 Current Status: Active PolicyStat ID: 4870880 Origination: 04/2018 Effective: 04/2018 Approved: 04/2018 Last Revised: 04/2018 Expiration: 04/2021 Owner: Policy Area: References: Suzanne Sharland-Hemmila:
Current Status: Active PolicyStat ID: 4870880 Origination: 04/2018 Effective: 04/2018 Approved: 04/2018 Last Revised: 04/2018 Expiration: 04/2021 Owner: Policy Area: References: Suzanne Sharland-Hemmila:
Outcomes of an Innovative Outpatient Monitor Service for Gynaecological Patients The Case Study of the Royal Free Hospital
 Outcomes of an Innovative Outpatient Monitor Service for Gynaecological Patients The Case Study of the Royal Free Hospital Dr Michela Tinelli November 2017 LSE Enterprise Limited London School of Economics
Outcomes of an Innovative Outpatient Monitor Service for Gynaecological Patients The Case Study of the Royal Free Hospital Dr Michela Tinelli November 2017 LSE Enterprise Limited London School of Economics
Basic Life Support in the Modern Era
 The ALS in BLS TheRoleof of Basic Life Support in the Modern Era Raymond L. Fowler, MD, FACEP Professor of Emergency Medicine, Surgery, and Allied Health The University of Texas Southwestern at Dallas
The ALS in BLS TheRoleof of Basic Life Support in the Modern Era Raymond L. Fowler, MD, FACEP Professor of Emergency Medicine, Surgery, and Allied Health The University of Texas Southwestern at Dallas
Even Better Support For Rescuers
 Even Better Support For Rescuers Beyond the AED Plus In 2002, ZOLL launched the AED Plus defibrillator with Real CPR Help real-time CPR Feedback to let rescuers know, for the first time ever, when they
Even Better Support For Rescuers Beyond the AED Plus In 2002, ZOLL launched the AED Plus defibrillator with Real CPR Help real-time CPR Feedback to let rescuers know, for the first time ever, when they
DECLARATION OF CONFLICT OF INTEREST
 DECLARATION OF CONFLICT OF INTEREST Data collection supported by unconditional grant of Physio- Control Place and use of the Automated External Defibrillator in the community R.W. Koster Academic Medical
DECLARATION OF CONFLICT OF INTEREST Data collection supported by unconditional grant of Physio- Control Place and use of the Automated External Defibrillator in the community R.W. Koster Academic Medical
IGEM/TD/2 Edition 2 with amendments July 2015 Communication 1779 Assessing the risks from high pressure Natural Gas pipelines
 Communication 1779 Assessing the risks from high pressure Natural Gas pipelines Founded 1863 Royal Charter 1929 Patron: Her Majesty the Queen Communication 1779 Assessing the risks from high pressure Natural
Communication 1779 Assessing the risks from high pressure Natural Gas pipelines Founded 1863 Royal Charter 1929 Patron: Her Majesty the Queen Communication 1779 Assessing the risks from high pressure Natural
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 20 June 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 20 June 2012 CINRYZE 500 units, 2100 IU, powder and solvent for solution for injection B/2 bottles (CIP code: 218
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 20 June 2012 CINRYZE 500 units, 2100 IU, powder and solvent for solution for injection B/2 bottles (CIP code: 218
PBR MODEL GOVERNANCE CHECKLIST: Some Considerations for Practicing Actuaries
 PBR MODEL GOVERNANCE CHECKLIST: Some Considerations for Practicing Actuaries 2016 American Academy of Actuaries. All rights reserved. May not be reproduced without express permission. PBR Boot Camp: Basic
PBR MODEL GOVERNANCE CHECKLIST: Some Considerations for Practicing Actuaries 2016 American Academy of Actuaries. All rights reserved. May not be reproduced without express permission. PBR Boot Camp: Basic
SOP 5.06 Full Committee Review: Initial IRB Review
 Office of Research Integrity - Human Subjects SOP #: ORI-HS(HS)- Page #: Page 1 of 5 Approved By: ORI-HS Executive Director *Signature on file Date: Date First Effective: 10/13/2016 Approved by: Biomedical
Office of Research Integrity - Human Subjects SOP #: ORI-HS(HS)- Page #: Page 1 of 5 Approved By: ORI-HS Executive Director *Signature on file Date: Date First Effective: 10/13/2016 Approved by: Biomedical