Author's Accepted Manuscript
|
|
|
- Chad Douglas
- 5 years ago
- Views:
Transcription

1 Author's Accepted Manuscript The effect of dutasteride on MRI-defined prostate cancer lesions: MAPPED (Magnetic resonance imaging in Primary Prostate Cancer after Exposure to Dutasteride) - a randomized placebo-controlled, double-blind clinical trial Caroline M. Moore, Nicola L. Robertson, Fatima Jichi, Adebiyi Damola, Gareth Ambler, Francesco Giganti, Ashley J. Ridout, Simon RJ. Bott, Mathias Winkler, Hashim U. Ahmed, Manit Arya, Anita V. Mitra, Neil McCartan, Alex Freeman, Charles Jameson, Ramiro Castro, Giulio Gambarota, Brandon J. Whitcher, Clare Allen, Alex Kirkham, Mark Emberton PII: S (16) DOI: /j.juro Reference: JURO To appear in: The Journal of Urology Please cite this article as: Moore CM, Robertson NL, Jichi F, Damola A, Ambler G, Giganti F, Ridout AJ, Bott SR, Winkler M, Ahmed HU, Arya M, Mitra AV, McCartan N, Freeman A, Jameson C, Castro R, Gambarota G, Whitcher BJ, Allen C, Kirkham A, Emberton M, The effect of dutasteride on MRIdefined prostate cancer lesions: MAPPED (Magnetic resonance imaging in Primary Prostate Cancer after Exposure to Dutasteride) - a randomized placebo-controlled, double-blind clinical trial, The Journal of Urology (2016), doi: /j.juro DISCLAIMER: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our subscribers we are providing this early version of the article. The paper will be copy edited and typeset, and proof will be reviewed before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to The Journal pertain. Embargo Policy All article content is under embargo until uncorrected proof of the article becomes available online. We will provide journalists and editors with full-text copies of the articles in question prior to the embargo date so that stories can be adequately researched and written. The standard embargo time is
2 12:01 AM ET on that date. Questions regarding embargo should be directed to
3 MAPPED: Effect of dutasteride on prostate cancer The effect of dutasteride on MRI-defined prostate cancer lesions: MAPPED (Magnetic resonance imaging in Primary Prostate Cancer after Exposure to Dutasteride) - a randomized placebo-controlled, double-blind clinical trial. Caroline M Moore 1,2, Nicola L Robertson 1,2, Fatima Jichi 3, Adebiyi Damola 1,2, Gareth Ambler 3, Francesco Giganti 4 Ashley J Ridout 1,2, Simon RJ Bott 5, Mathias Winkler 6, Hashim U Ahmed 1,2, Manit Arya 1,2, Anita V Mitra 7, Neil McCartan 2, Alex Freeman 8, Charles Jameson 8, Ramiro Castro 9, Giulio Gambarota 10,11, Brandon J Whitcher 12,13, Clare Allen 4, Alex Kirkham 4, Mark Emberton 1,2. 1 Division of Surgery & Interventional Science, University College London, UK 2 Department of Urology, University College London Hospitals NHS Foundation Trust, London, UK 3 Biostatistics Group, University College London Hospitals/University College London Research Support Centre, University College London, UK 4 Department of Radiology, University College London Hospital Trust, London, UK 5 Department of Urology, Frimley Park Hospital, Surrey, UK 6 Department of Urology, Charing Cross Hospital, Imperial College NHS Trust, London, UK 7 Department of Clinical Oncology, University College Hospital London, London, UK 1
4 MAPPED: Effect of dutasteride on prostate cancer 8 Department of Pathology, University College London Hospital Trust, London, UK 9 GlaxoSmithKline Research and Development. Philadelphia. USA 10 INSERM, U1099, Rennes, F-35000, France 11 Université de Rennes 1, LTSI, Rennes, F-35000, France 12 Klarismo, London, UK 13 Department of Mathematics, Imperial College London, UK Corresponding author: Caroline M Moore caroline.moore@ucl.ac.uk Division of Surgical & Interventional Sciences 4 th Floor, 74 Huntley Street London, UK WC1E 6AU Running head (max 50 characters): MAPPED: Effect of dutasteride on prostate cancer Key words (1 to 5) Prostate cancer; active surveillance; MRI; targeted biopsy; dutasteride 2
5 MAPPED: Effect of dutasteride on prostate cancer Abstract (249/250) Purpose Dutasteride is licensed for symptomatic benign prostatic hyperplasia, and has been associated with a lower progression rate in low-risk prostate cancer. We have evaluated the effect of dutasteride on prostate cancer volume as assessed by T2-weighted Magnetic Resonance Imaging (MRI). Materials and methods In this randomized, double-blind, placebo-controlled trial, men with biopsyproven low-intermediate risk prostate cancer (up to Gleason 3+4 and PSA up to 15 ng/ml) who had an MR visible lesion of >/= 0.2ml on T2-weighted sequences were randomized to daily dutasteride 0.5mg or placebo for 6 months. Lesion volume was assessed at baseline, 3 and 6 months, with an image-guided biopsy to the lesion at study exit. The primary endpoint was percentage reduction in lesion volume over 6 months. This trial was registered with the European Clinical Trials register (EudraCT ). Results Forty-two men were recruited between June 2010 and January In the dutasteride group, the average volumes at baseline and 6 months were 0.55ml and 0.38ml respectively, and the average percentage reduction was 36%. In the placebo group, the average volumes at baseline and 6 months were 0.65ml and 0.76ml respectively, and the average percentage reduction was -12%. The difference in percentage reductions between groups was 48% (95% CI %. p< ). The most common adverse event was deterioration in 3
6 MAPPED: Effect of dutasteride on prostate cancer erectile function (25% in men randomized to dutasteride, 16% in men randomized to placebo). Conclusions Dutasteride was associated with a significant reduction in prostate cancer volume on T2 weighted MRI images compared to placebo. 4
7 MAPPED: Effect of dutasteride on prostate cancer Introduction Dutasteride is licensed for men with lower urinary tract symptoms (LUTS) associated with benign prostatic enlargement 1. When assessed in placebo controlled prostate cancer studies, dutasteride reduced the proportion of men diagnosed with prostate cancer by 22.8% over 4 years 2, and was associated with lower rates of disease progression over 3 years in men on active surveillance 3. Magnetic resonance imaging (MRI) of the prostate allows assessment of prostate cancer volume over time 4,5. We report the use of MRI to assess the effect of dutasteride on prostate cancer volume in men on active surveillance. 5
8 MAPPED: Effect of dutasteride on prostate cancer Materials and methods This investigator led study, sponsored by University College London, was approved by the Hammersmith & Queen Charlotte s & Chelsea Research Ethics Committee (UK) (09/H0707/84), the Medicines & Health Regulatory Agency and registered on the European Clinical Trials register (EudraCT ). Primary and secondary objectives The primary objective was to evaluate the percentage reduction in tumour volume, assessed by T2-weighted MRI (T2W-MRI), following exposure to dutasteride 0.5 mg daily for six months, compared to placebo. Secondary objectives included percentage reduction in tumour volume at 3 months, and on functional MR sequences, namely dynamic contrast enhanced (DCE) imaging and diffusion weighted imaging (DWI). Prostate cancer typically shows rapid wash-in and wash-out on DCE imaging due to the increased vascularity of its highly permeable neo-vessels. DWI of prostate cancer typically shows restricted diffusion due to disorganized tissue structure, seen as high signal (bright areas) on high b-value imaging 6. Patient population The full study protocol has been published 7. Eligible men met the UK NICE 2008 active surveillance criteria 8 (up to Gleason 3+4 disease, PSA up to 15 ng/ml), based on biopsy within the preceeding two years. In addition, men were required to have a >0.2 ml lesion on the standard of care T2-weighted MRI. 6
9 MAPPED: Effect of dutasteride on prostate cancer All eligible consented men had a study specific standardized multi-parametric 3 Tesla MRI. The images were reviewed by one study radiologist (CA, AK) to assess for the presence of a T2W lesion >0.2 ml. When confirmed, the man was randomized to placebo or dutasteride 0.5mg daily for 6 months. MRI was repeated at 3 and 6 months. Each MRI scan was reported separately by each of the study radiologists, who were blinded to treatment allocation. An exit biopsy was offered to all men, with 10 standard cores and additional cores targeted to the MRI lesion using visual registration 9. Men were not rebiopsied for discordant histology at baseline, in order to avoid post biopsy artefact on the study MRI scans. The concordance between baseline histology, lesion on MRI and exit histology was assessed. PSA, renal and liver function and adverse events were assessed at baseline, 3 and 6 months. Randomization and masking Seventeen patients were required to complete each arm to detect a 20% reduction in tumor volume, assuming a common standard deviation of 20.5%, power of 80% and 5% statistical significance. To account for failure to complete, we aimed to recruit 21 men per arm. Men were individually randomized using block randomization with varying block sizes. The statistical team at University College London (UCL) supplied UCLH pharmacy with a randomization list to allocate study medication. The patients, study doctors, radiologists and 7
10 MAPPED: Effect of dutasteride on prostate cancer 1 2 histopathologists were blind to treatment allocation. The radiologists and histopathologists were also blind to PSA results Outcomes and statistical analysis The primary outcome was percentage reduction in tumor volume between baseline and 6 months on T2-weighted imaging. This was calculated using (baseline volume 6-month volume)/baseline volume 100%, where baseline volume and 6 months volume were the average of the measurements from the two raters. This percentage reduction was compared between the dutasteride and placebo groups using a t-test, with statistical significance set at a p-value of The secondary outcomes of percentage reduction in tumor volume as measured by DCE and DWI at six months, were compared between the dutasteride and placebo groups using a t-test. Each analysis was repeated for percentage reduction in tumour volume at three months. 8
11 MAPPED: Effect of dutasteride on prostate cancer Results Fifty six men consented to the study after meeting eligibility criteria based on standard of care MRI, histology and blood tests. Seven men were excluded as the study PSA or renal function did not meet the eligibility criteria. Forty-nine men had a study MRI scan. Seven of these men were excluded on MRI criteria. Forty-two men were randomized between June 2010 and January 2012 (CONSORT 10 diagram, figure 1). Twenty-one men were randomized to each group (Table 1). One man exited the dutasteride group prior to taking any study medication as he wished to conceive a child. Another man exited the placebo group to have active treatment in response to upgrading from Gleason to Gleason at UCLH pathology review. The primary endpoint was derived in 20 men within each group. When the baseline scans were formally reported, it was noted that a total of 11/42 randomized men had lesions which measured as less than 0.2ml on T2- weighted images by one (n = 5) or both (n=6) study radiologists. All of these men had lesions volume of 0.2ml on other sequences (DCE and diffusion weighted imaging) by at least one of the radiologists. One of the men was deemed to have a visible lesion by one radiologist but not by the other. Eight men had a mean lesion volume of <0.2ml for the lesion on T2 weighted imaging These men were included in the analysis, as they had met the original inclusion criteria (one study radiologist assessing the MRI scan as showing a 0.2ml lesion on MRI). The agreement in volume assessment between the 2 raters was formally assessed. 9
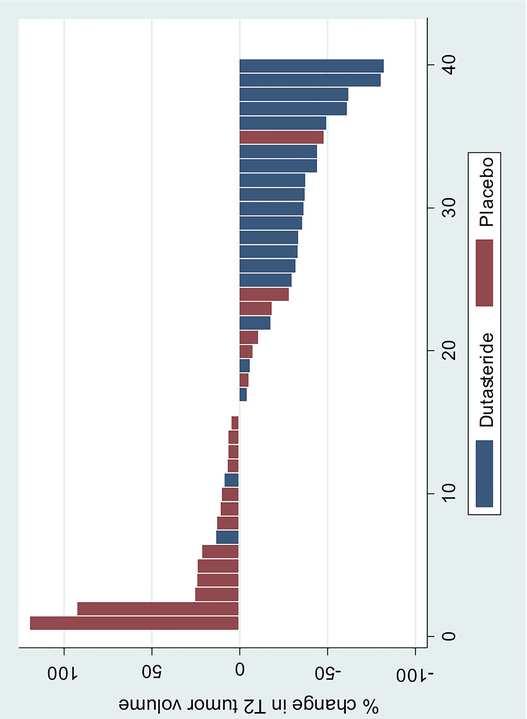
12 MAPPED: Effect of dutasteride on prostate cancer Primary outcome Change in total tumor volume on T2W-MRI over 6 months (Table 2) In the dutasteride group, the average volumes at baseline and 6 months were 0.55ml and 0.38ml respectively, and the average percentage reduction was 36%. In the placebo group, the average volumes at baseline and 6 months were 0.65ml and 0.76ml respectively, and the average percentage reduction was - 12% 9ie 12% growth). The difference in percentage reductions between groups was 48% (95% CI , p <0.0001) (figure 2). Fifteen of twenty men (75%) randomized to dutasteride had a reduction in tumor volume; 5/20 (25%) had stability (defined as < 20% volume change). No man randomized to dutasteride had an increase in tumor volume. In contrast, 2 men (10%) in the placebo group had a reduction in volume, 13 (65%) were stable and 5 (25%) exhibited an increase of > 20% (figure 3). Secondary outcomes Change in tumor volume on functional imaging over 6 months (Table 2) On DCE imaging, men randomized to dutasteride had a 42.3% reduction in tumor volume at 6 months compared to 4.2% reduction in men men randomized to placebo (38% mean difference between groups, 95% CI: , p= ) On diffusion weighted imaging, men randomized to dutasteride had a 33% reduction in tumor volume at 6 months compared to a 7% increase in the men 10
13 MAPPED: Effect of dutasteride on prostate cancer 1 2 randomized to placebo, conferring a mean difference between groups of 40% (95% CI , p = ) Change in tumor volume over 3 months (T2-weighted imaging) At 3 months there was a 34% reduction in tumor volume in the dutasteride group compared to 0.21% in the placebo group (mean difference between groups 34% (95% CI 21 47%, p = < ). Change in prostate volume The average percentage reduction in prostate volume at 6 months was 15% in the dutasteride group, compared to an increase of 3.3% in the placebo group (mean difference between groups 18.8% (95% CI %, p<0.0001). Agreement between raters The agreement between the raters was investigated using a Bland-Altman plot based on the percentage reduction in tumor volume calculated separately for each individual rater (supplementary figure 1). In addition, the analysis of the primary outcome was repeated for each rater separately (supplementary table 1). One patient was deemed by one rater to have an increase in volume and the other rater to have a reduction in volume, and this had a significant effect on the results of rater 1. The table shows the analysis with and without this outlier. The results are consistent across the raters although rater 1 has recorded a larger volume reduction than rater
14 MAPPED: Effect of dutasteride on prostate cancer Histological data (Supplementary table 2) All men were offered an end of study biopsy, although 12 of 40 men declined. Histological upgrading to Gleason > 4+ 3 was seen in 3/15 (20%) in the dutasteride group, and in 6/13 (46%) in the placebo group. Concordance of MRI lesions and histology (supplementary table 3) Thirty seven men of forty men had histological confirmation of the MRI lesion at baseline or exit. The remaining three men had discordant baseline histology, of whom one had a negative exit biopsy (placebo group) and two declined the exit biopsy (one placebo, one dutasteride). PSA changes (supplementary table 4) In men on placebo, the direction of change of PSA mirrored the direction of change in tumour volume. All men on dutasteride showed a PSA reduction, with no clear correlation between the change in lesion volume and PSA. Medication compliance All men were compliant with medication according to the returned tablet count at the end of each 3 month prescription period Adverse events No serious adverse events occurred, and no subject discontinued study medication due to adverse events. Deterioration of sexual function (at least a 4 point reduction in IIEF ) occurred in 8 of 40 men (5/20 (25%) on dutasteride and 3/19 (16%) on placebo. 12
15 MAPPED: Effect of dutasteride on prostate cancer Discussion Dutasteride 0.5mg daily was associated with an average reduction in prostate cancer volume of 36%, compared to an average increase of 12% in men on placebo, as assessed by T2W-MRI over six months. This volume change was associated with less histological upgrading at targeted biopsy on study exit when randomized to dutasteride than to placebo (20% versus 46%). However, the lack of targeted biopsies at baseline to match to targeted exit biopsies and the small sample size limit the ability to definitively ascribe this to the effect of dutasteride. The rate of upgrading in the placebo group was high compared to that seen in men undergoing scheduled repeat standard core systematic biopsy on active surveillance protocols 12. However, this was expected due to the use of image-guided targeting as well as standard biopsy exit, compared to standard biopsy alone at entry, in the majority 13. In 3 of 40 men there was a lack of concordance between biopsy and entry histology, not resolved on targeted biopsy at exit, which may represent a false positive MRI lesion, although 2 of the men declined the exit biopsy, and so this could not be confirmed There have been concerns that dutasteride may act selectively on low grade tumors, and may be associated with a greater likelihood of developing highgrade cancers 14, although radical prostatectomy data from randomized studies have not confirmed this
16 MAPPED: Effect of dutasteride on prostate cancer In this study, two men randomized to dutasteride had 1mm and 2mm respectively of Gleason on targeted biopsy at exit, with an overall Gleason grade of At entry, the first had 9mm Gleason on standard transrectal biopsy, with a lesion volume of 0.97ml, which reduced to 0.64ml at 6 months. The second had 4mm 3+ 4 on targeted biopsy at entry, with a lesion volume of 0.20ml, which reduced to 0.13ml at 6 months. This grade increase on targeted biopsy at exit would be compatible with the grade shift seen with a targeted biopsy approach 16. Dutasteride-associated reduction in prostate cancer volume was seen at 3 months, with marginal additional reduction by 6 months, with a similar timescale to prostate volume reduction in LUTS studies. We noted greater proportional reduction in tumor volume compared to whole prostate volume which suggests that prostate cancer may be more sensitive to androgen depletion than noncancerous prostate tissue. The functional MRI sequences (DCE and DWI) assess perfusion and cell density, respectively. The percentage volume reduction in functional sequences was similar to that on T2Wi, although DWI tumor volumes were lower than on other sequences The adverse event profile was compatible with the known side effects of dutasteride, with significantly more men taking dutasteride (25% vs 16%) showing deterioration in sexual function
17 MAPPED: Effect of dutasteride on prostate cancer The study is limited in both its sample size and duration. The 20% threshold for a reduction in tumor volume change was chosen, as it was the least change that might be considered both clinically meaningful and assessable by our independent observers. Sufficient men were recruited to achieve a power of 80% to detect a 20% volume change. A six-month interval of assessment is common in many active surveillance protocols 12, and is known to show response to dutasteride in studies of men with LUTS. The fact that a study of this size and duration could meet its primary endpoint is promising for future exploratory studies of this type. Another limitation of the study relates to the external validity of the study population. The eligibility criteria consisted of the UK NICE 2008 criteria for active surveillance in men with low or intermediate risk disease (Gleason sum 7 or less, PSA < 15ng/ml), clinical T2b disease). Of note, these criteria do not include any estimation of burden of disease such as the number of cores positive, maximum cancer core length or percentage cancer core involvement. In addition to the UK NICE criteria, men were required to have a lesion visible on T2W-MRI. Men with lesions seen exclusively on functional imaging were excluded. We do not know whether radiological phenotype predicts prognosis or responsiveness, although men with no visible lesion on MRI are at lower risk of progression than men with a visible lesion We assessed for an imbalance of tumor size in each group which might lead to a spurious result, if larger tumors are assumed to have a greater growth rate. 15
18 MAPPED: Effect of dutasteride on prostate cancer Four men had tumor volumes >1 ml, 3 of whom were randomized to placebo. We repeated the analysis with these men removed and found very similar results. In addition, a formal analysis that adjusted for baseline volume was performed with little change in the outcome. Our findings may have important clinical implications. First, if MRI reliably detects prostate cancer volume change then it could be useful for reassessment during surveillance 18. Further work is needed to determine the imaging parameters (rate of change or an absolute threshold) at which transition to active treatment should be initiated, as recommended in the recent PRECISE guidelines 19 Second, this novel design might be useful in assessing well tolerated agents that might modify the natural history of prostate cancer (e.g. aspirin, vitamin D, and dietary modifications including cruciferous vegetables ). To date, large and expensive epidemiological studies of long duration 20 using repeat random biopsies in men on active surveillance 21 have been used. Our novel study design could allow initial screening of potential agents for further study. Conclusions Dutasteride is associated with a reduction in prostate cancer volume as assessed by T2W-MRI in men with biopsy proven low or intermediate risk prostate cancer suitable for active surveillance, over a six-month period. This novel imaged based study design may be of use in assessing response to other well tolerated interventions in men on active surveillance. 16
19 MAPPED: Effect of dutasteride on prostate cancer 2499/2500 words 17
20 MAPPED: Effect of dutasteride on prostate cancer Disclosures The study was investigator-led and sponsored by University College London. The study was supported financially by GSK who also provided supplies of both drug and placebo. GSK had no input into the design, conduct and analysis of the study. The manuscript has been reviewed by GSK but final editorial control rests with the principal investigator (ME), who serves as guarantor of the study. Acknowledgements We would like to thank the men who gave their consent to participate in this study. Mark Emberton receives research support from the United Kingdom s National Institute of Health Research UCLH/UCL Biomedical Research Centre. Mark Emberton holds Senior Investigator status with the United Kingdom's National Institute of Health Research. 18
21 MAPPED: Effect of dutasteride on prostate cancer References 1. Roehrborn CG, Boyle P, Nickel JC, et al. Efficacy and safety of a dual inhibitor of 5-alpha-reductase types 1 and 2 (dutasteride) in men with benign prostatic hyperplasia. Urology. 2002;60(3): Andriole GL, Bostwick DG, Brawley OW, et al. Effect of dutasteride on the risk of prostate cancer. N Engl J Med. 2010;362(13): Fleshner NE, Lucia MS, Egerdie B, et al. Dutasteride in localised prostate cancer management: the REDEEM randomised, double-blind, placebocontrolled trial. Lancet. 2012;379: Kirkham APS, Emberton M, Allen C. How good is MRI at detecting and characterising cancer within the prostate? Eur Urol. 2006; 50(6): ; discussion Villers A, Puech P, Mouton D, et al. Dynamic contrast enhanced, pelvic phased array magnetic resonance imaging of localized prostate cancer for predicting tumor volume: correlation with radical prostatectomy findings. J Urol. 2006;176(6): Barentsz JO, Richenberg J, Clements R, et al. ESUR prostate MR guidelines Eur Radiol. 2012;22(4): Robertson NL, Moore CM, Ambler G, et al. MAPPED study design: A 6month randomised controlled study to evaluate the effect of dutasteride on prostate cancer volume using magnetic resonance imaging. Contemp Clin Trials. 2012;34(1): National Institute for Health and Clinical Excellence. Prostate cancer: diagnosis and treatment (February 2008). Accessed via 19
22 MAPPED: Effect of dutasteride on prostate cancer 9. Moore CM, Kasivisvanathan V, Eggener S, et al. Standards of Reporting for MRI-targeted Biopsy Studies (START) of the Prostate: Recommendations From An International Working Group. Eur Urol. 2013;64(4): Begg C, Cho M, Eastwood S, et al. Improving the quality of reporting of randomized controlled trials. The CONSORT statement. JAMA. 1996;276(8): Rosen RC, Riley A, Wagner G, et al. The International Index of Erectile Function (IIEF): A Multidimensional Scale for Assessment of Erectile Dysfunction. Urology. 1997;49(6): Dall'Era MA, Cooperberg MR, Chan JM, et al. Active Surveillance for Early-stage Prostate Cancer: Review of the Current Literature. Cancer. 2008;112(8): Siddiqui MM, Rais-Bahrami S, Turkbey B, et al. "Comparison of MR/ultrasound Fusion-guided Biopsy with Ultrasound-guided Biopsy for the Diagnosis of Prostate Cancer. JAMA 2015:313(4): Andriole GL, Bostwick DG, Gomella LG, et al. Modeling and analysis of Gleason score 8-10 prostate cancers in the REDUCE study. Urology. 2014;84(2): Iczkowski KA, Qiu J, Qian J, et al. The dual 5-alpha-reductase inhibitor dutasteride induces atrophic changes and decreases relative cancer volume in human prostate. Urology. 2005;65(1): Robertson NL, Hu Y, Ahmed HU, et al. Prostate Cancer Risk Inflation as a Consequence of Image-targeted Biopsy of the Prostate: A Computer Simulation Study. Eur Urol. 2014;65(3):
23 MAPPED: Effect of dutasteride on prostate cancer 17. Park, BH, Jeon HG, Choo SH, et al. Role of Multiparametric 3.0 Tesla Magnetic Resonance Imaging in Prostate Cancer Patients Eligible for Active Surveillance. BJU Int 2014;113(6): Graham J, Kirkbride P, Cann K, et al. Prostate cancer: a summary of updated NICE guidance, BMJ. 2014;348 :f Moore CM, Giganti F, Albertsen P et al. Reporting MRI in men on active surveurveillance for prostate cancer. The PRECISE recommendations: A report of a European School of Oncology Task Force. Eur Urol 2016 doi: /j.eururo Veitonmäki T, Tammela TLJ, Auvinen A, et al. Use of Aspirin, but Not Other Non-steroidal Anti-inflammatory Drugs Is Associated with Decreased Prostate Cancer Risk at the Population Level. Eur J Cancer. 2013;49(4): Marshall DT, Savage SJ, Garrett-Mayer E, et al., Vitamin D3 supplementation at 4000 international units per day for one year results in a decrease of positive cores at repeat biopsy in subjects with low-risk prostate cancer under active surveillance. J Clin Endocrinol Metab. 2012;97(7): Liu B, Mao Q, Cao M, Xie L. Cruciferous vegetables intake and risk of prostate cancer: a meta-analysis. Int J Urol, 2012;9(2):
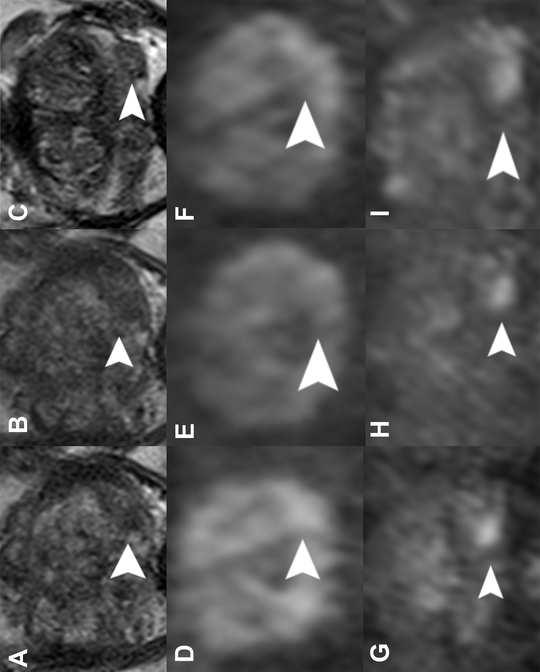
24 MAPPED: Effect of dutasteride on prostate cancer List of figures 1. CONSORT diagram showing patient recruitment 2. Waterfall plot showing percentage change of tumor volume on T2- weighted MRI at 6 months compared to baseline for dutasteride and placebo groups 3. MRI comparing baseline and six month scans in a man randomized to dutasteride (A) and to placebo (B) List of supplementary figures S1: Bland Altman plot showing agreement between raters List of tables 1. Baseline characteristics of men in each of the treatment allocation groups. 2. Change in tumor volume from baseline to 6 months List of supplementary tables S1. Agreement between radiological raters S2 Histological results at exit biopsy category by treatment group S3: Concordance of histology and MRI findings S4: PSA changes in man allocated to placebo and dutasteride 22
25 MAPPED: Effect of dutasteride on prostate cancer Legends for figures Figure 1 CONSORT diagram showing men in study Figure 2 The percentage change in total tumor volume for all 40 patients between baseline and six months as measured on T2-weighted imaging Figure 3A: A 68 year-old man with a lesion in the left peripheral zone (arrow). The lesion is seen as low signal on T2-weighted imaging at baseline (A), and to have reduced in size at 3 months (B) and further at 6 months (C) after 6 months of daily dutasteride 0.5mg. On diffusion weighted imaging, the baseline scan (D) shows high signal lesion of smaller volume than the T2-weighted lesion. At 3 months (E) and 6 months (F) this has decreased in size, although to a lesser extent than the reduction evident on the T2-weighted and diffusion weighted imaging. Dynamic contrast enhanced images at baseline (G) show an enhancing lesion in the left peripheral zone. This reduces in volume at 3 moths (H) and 6 months (I). Figure 3B: A 71 year-old man from the placebo group with a right peripheral zone lesion at baseline on T2-weighted imaging (A). This is stable at 3 months (B) and 6 months (C). The lesion is seen as high signal on diffusion weighted imaging at baseline (D), and stable at 3 months (E) and 6 months (F). The lesion shows enhancement on dynamic contrast enhanced images at baseline (G), and whilst less conspicuous at 3 months (H) these are stable at 6 months (I ). Figure S1 Bland Altman plot showing the relationship between the percentage reduction in tumor volume between raters. 23
26 Table 1: Baseline characteristics in each group. Continuous variables summarized as mean (sd, range) and categorical variables summarized as n (%). Dutasteride (n = 21) Placebo (n = 21) Age (yrs) (7.3, 49.0 to 79.2) 64.2 (7.5, 39.5 to 76.0) Total PSA (ng/ml) 6.94 (3.0, 1.8 to 13.4) 6.01 (2.3, 1.3 to 9.7) Prostate volume (ml) (20.7, 20.7 to 98.8) (22.1, 16.7 to 104.3) PSA density (ng/ml/ml) 0.16 (0.06, 0.07 to 0.28) 0.12 (0.05, 0.05 to 0.23) Targeted transrectal biopsy Targeted template biopsy Template guided transperineal biopsy Transrectal biopsy UCL biopsy Biopsy at local referral center Maximum Gleason (14.3) 4 (19.1) 3 (14.3) 3 (14.3) 5 (23.8) 10 (47.6) 2 (9.52) 12 (57.1) 12 (57.1) 14 (66.7) 9 (42.9) 7 (33.3) 11 (52.4) 12 (57.1) Maximum Gleason Total no. of cores (median, range) 10 (47.6) 12 (8 to 95) 9 (42.9) 14 (8 to 64)
27 Total number of positive cores 4.62 (2.8, 1 to 12) 4.95 (3.6, 1 to 12) Percentage of positive cores Maximum cancer core length (mm) Tumor volume (ml) : T2WI Tumor volume (ml) : DCE Tumor volume (ml) :DWI Total index tumor volume (ml) on T2 weighted imaging DCE Diffusion 29.5 (21.9, 2 to 75) 5.05 (2.3, 1 to 9) 0.55 (0.49, 0.12 to 0.36) 0.58 (0.5, 0.06 to 2.34) 0.48 (0.6, 0.07 to 2.70) 0.50 (0.34, 0.12 to 1.44) 0.52 (0.3, 0.06 to 1.41) 0.42 (0.3, 0.07 to 1.59) 29.2 (18.4, 5 to 75) 4.57 (2.2, 1 to 9) 0.65 (0.8, 0 to 3.27) 0.67 (0.8, 0.09 to 3.72) 0.42 (0.3, 0 to 1.18) 0.59 (0.6, 0 to 2.21) 0.63 (0.7, 0.09 to 3.25) 0.37 (0.3, 0 to 1.18)
28 Table 2: Change in total tumor volume between baseline and six months on T2-weighted imaging, dynamic contrast enhancement and diffusion weighted imaging Dutasteride (20) Placebo (20) Mean Total tumor volume (ml) at baseline (T2) Total tumor volume (ml) at 6 months (T2) % change in total tumor volume from 0-6 months (T2) Mean (sd, range) Mean (sd, range) 0.55 (0.5, 0.12 to 2.36) 0.38 (0.4, 0.02 to 1.59) (25.7, to 13.21) 0.65 (0.8, 0 to 3.27) 0.76 (0.9, 0.09 to 3.96) (37.2, to ) Total tumor volume at 0.58 (0.5, 0.67 (0.8, baseline (gadolinium/dce) to 2.342) 0.09 to 3.72) Total tumor volume at 6 months (gadolinium/dce) 0.35 (0.3, to 1.328) 0.66 (0.8, to 3.68) % change in total tumor volume from 0-6 months (25.6, (38.5, (gadolinium/dce) to 3.76) to ) difference (95% CI) p- value (27.42, 68.34), p < (16.59, 59.64) p= Total tumor volume at baseline (diffusion) Total tumor volume at 6 months (diffusion) 0.48 (0.6, 0.07 to 2.695) 0.30 (0.3, 0.05 to 1.284) 0.42(0.3, 0 to 1.18) 0.45 (0.4, 0 to 1.165) % change in total tumor (21.8, 7.01 (35.9, 40.47
29 volume from 0-6 months ACCEPTED MANUSCRIPT to 20.24) to 95.49) (21.31, (diffusion) 59.63)p=
30
31
32

33
34 List of abbreviations DHT = dihydrotestosterone LUTS = lower urinary tract symptoms MRI = magnetic resonance imaging T2W-MRI = T2-weighted MRI DCE = dynamic contrast enhanced DWI = diffusion weighted imaging UCLH = University College London Hospital UCL = University College London BPH = benign prostatic hyperplasia
35 Supplementary table 1 : Agreement between radiological raters Analysis Subset Rater 1: Percentage reduction in total tumour volume from 0-6 months (T2) (as above with outlier omitted) Rater 2: Percentage reduction in total tumour volume from 0-6 months (T2) Both (average): Percentage reduction in total tumour volume from 0-6 months (T2) Dutasteride (n = 20) Mean (SD) Placebo (n = 20) Mean (SD) Mean difference (95% CI) P-value 41.4 (29.2) (121.9) to P = (29.2) -0.7 (26.8) to 60.2 P < (31.9) -1.3 (31.5) 25.2 (5.0 to 45.5) P = (25.7) -5.8 (27.6) 41.5 (24.5 to 58.6) 1
36 Supplementary table 2: Maximum cancer core length and maximum Gleason score at exit a) Men in the dutasteride group (n=15) Maximum Maximum Gleason score Total core length Too small Total b) Men in the placebo group (n=13) Maximum core length Maximum Gleason score Total Too small Total
37 Supplementary table 3: Concordance of histology and MRI findings Randomization number Dutasteride (D) or Placebo (P) Initial histology R001 P 1 mm 3+3 left anterior horn 1 mm 3+3 left lateral mid, left para mid, left para base R002 D 4 mm 3+3 left lateral base 5 mm 3+3 left para base 1 mm 3+3 left para base 3 mm 3+3 left para mid Location of lesion on mpmri Histology at exit Concordance Right base-mid No report Not concordant at baseline; no exit histology. Post study biopsy showed focal HGPIN only. Left base Targeted bx left base 2 mm 3+4 R003 P 1 mm 3+3 right apex Right apex Targeted bx right apex 4 mm 4+3 R004 D 9 mm, 3mm, 2mm 3+3 left Left mid and apex Targeted bx left lateral mid 2 mm 3+4 R005 D 1 mm 3+3 left para-anterior apex 1 mm 3+3 right paraanterior apex 2 mm 3+3 right paraanterior apex 1 mm 3+3 left medial anterior apex Right mid-base and apex Right para-mid 1 mm 3+4 Right lateral mid 3 mm 3+3 Right apex 1 mm 3+3 Right lateral base 1 mm 3+3 Concordant at baseline and exit Concordant at baseline and exit Concordant at baseline and exit Concordant at baseline and exit 4
38 1 mm 3+3 left medial anterior apex 4 mm 3+3 left medial anterior apex 1 mm 3+3 left lateral 1 mm 3+3 left lateral 1 mm 3+3 right paraposterior base 3 mm 3+3 left medial posterior apex 1 mm 3+3 right medial posterior base R006 P 1 mm 3+3 right post medial apex 3 mm 3+3 post medial apex 3 mm 3+3 right posterior para-apex R007 P 4 mm 3+4 right base pz 5 mm 3+3 right base pz 1 mm 3+3 right para-base 5 mm 3+3 left mid pz 5 mm 3+4 left apex pz 2 mm 3+3 apex pz 5 mm 3+3 para-apex R008 D 4mm, 4mm, 4 mm 3+3 left 8, 6, 5, 2 mm 3+4 right Right base Right para-base 11 mm 3+4 Right para-mid 1 mm 4+3 Left base-mid-apex Targeted bx left 2 mm 3+4 Right mid Left mid-base Targeted bx right lateral mid 4 mm 3+3 Concordant at baseline and exit Concordant at baseline and exit Concordant baseline and exit R009 D 8mm, 1 mm 3+3 right Right mid Targeted bx Concordant at 5
39 R010 P 2 mm 3+3 left para-anterior apex 3 mm 3+3 left para-anterior base 2 mm 3+3 left para-anterior apex 3 mm 3+3 right paraanterior base 8 mm 3+3 right paraanterior base 3 mm 3+3 right medialanterior base 4 mm 3+3 right medialanterior base 6 mm 3+3 right medialanterior base 1 mm 3+3 right medialanterior apex 1 mm 3+3 right medialanterior apex 2 mm 3+3 right medialanterior apex Left mid-base Right mid-base right mid 4 mm 3+4 No tumor at biopsy exit R011 P 4mm, 2mm, 1 mm 3+4 right Right mid-base Targeted bx right mid-base 8 mm 3+4 R012 P 3 mm, 3mm 3+4 right NK 1 mm 3+3 left Right mid-apex Targeted bx right mid-lateral 8 baseline and exit Concordant at baseline; negative at exit. Went on to have focal ablation based on initial template biopsy. Concordant at baseline and exit Concordant at baseline and exit 6
40 mm, 6mm 3+4 R013 D 1 mm, 0.5mm 3+3 right Mid-base (anterior) Targeted bx anterior 2 mm 3+4 R014 D 1 mm 3+3 left lateral base 2 mm 3+3 left central lateral 1 mm 3+3 right base lateral 1 mm 3+3 right central lateral 2 mm 3+3 right apex Right mid-base Targeted bx right mid 6mm, 3 mm 3+4 R015 P 2 mm 3+3 left anterior Right mid No tumor at biopsy exit R016 D 1 mm 3+3 right lateral 1 mm 3+3 left para-anterior apex R017 D 5mm,2mm,1mm, 1mm, 1 mm 3+4 right apex 6mm,4mm, 2 mm 3+4 right base 4 mm 3+3 left apex 3 mm 3+4 left base 1 mm 3+3 left base Right apical Targeted bx right apex-mid 3 mm 3+4 Right mid-lateral Left mid-lateral Right mid-lateral 5 mm 3+4 Left mid-lateral 2 mm 3+3 Concordant at baseline and exit Concordant at baseline and exit Discordant at entry; negative biopsy at exit. Remains on active surveillance. Concordant at biopsy and exit Concordant at baseline and exit R018 D 3mm, 2mm,1 mm 3+4 right Right mid-base Targeted bx Concordant at 7
41 3 mm 3+4 left lateral Right mid- base anterior R019 D 5mm, 4mm, 3mm, 2mm, 2 mm 3+4 right 1 mm, 1mm 3+3 left R020 P 2 mm 3+3 right 5mm, 3mm, 1mm, 1mm 1 mm 3+3 left R021 P 5mm,1mm, 1 mm 3+4 left 1 mm 3+4 right R022 P 1 mm 3+3 NK 8 mm 3+4 NK 3 mm 3+4 right lateral base 1 mm 3+3 left para-apex 1 mm 3+3 left para-base 4 mm 3+3 right para-apex 2 mm 3+4 right para-base 2 mm 3+3 right lateral apex Left mid-apex Left mid Left mid right mid 6 mm 3+4 Targeted bx right base ant. 3 mm 3+3 Left paraposterior apex - 4 mm 3+4 Left medial posterior base 8 mm 3+4 Targeted bx left mid-apex 9mm, 8 mm, 1.5mm 3+3 Targeted bx left mid 8mm, 6mm, 4mm, 4mm, 3mm 3+4 baseline and exit Concordant at baseline and exit Concordant at baseline and exit Concordant at baseline and exit Right base No biopsy at exit Concordant at baseline ; no exit biopsy. No further biopsies. 8
42 R023 D 6 mm 3+4 right lateral mid 4 mm 3+3 right para-mid 1 mm 3+3 right para-apex 5 mm 3+4 right midperipheral zone R024 P 4mm,3mm,1 mm 3+3 left lateral base R025 D 4 mm, 3mm 3+4 left lateral base R026 P 2 mm 3+3 mid-apex 6 mm 3+3 right medial anterior apex 1 mm 3+3 right mid anterior base 5 mm 3+3 right mid anterior base 1 mm 3+3 right medial posterior apex 1 mm 3+3 right medial posterior base 1 mm 3+3 right 3 mm 3+3 right 1 mm 3+3 targeted right anterior horn 1 mm 3+3 targeted right anterior horn 2 mm 3+3 targeted right Right mid-base Targeted bx right mid-base 8, 2mm 3+4 Left mid-base Left base No tumor at biopsy exit Targeted bx left base 2 mm 3+3 Concordant at baseline and exit Concordant at baseline; no biopsy at exit Concordant at baseline and exit Right mid-base No biopsy at exit Concordant at baseline; no biopsy at exit 9
43 anterior horn 5 mm 3+3 targeted right anterior horn R027 D 3mm, 1 mm 3+3 right 5mm, 4 mm 3+3 left R028 P 1 mm,1mm,1mm 3+3 6mm, 3mm, 3mm, 1mm, 1 mm 3+3 right R029 P 1 mm 3+3 right base medial 1 mm 3+4 right lateral base R030 D 6 mm 3+4 right lateral base 6 mm 3+4 right mid-lateral base R031 D 3.5 mm 3+3 right NK 6 mm 3+3 right NK 0.5 mm 3+3 right NK R032 D 3 mm 3+3 mid anterior apex I 2 mm 3+3 para-posterior apex I 1 mm 3+3 para-posterior apex I 1 mm 3+3 right paraposterior apex Right base Targeted bx right base 6mm, 5 mm 3+3 Concordant at biopsy and exit Right mid-base No biopsy at exit Concordant at baseline; no biopsy at exit Right mid-base Left mid-base No biopsy at exit Right mid Targeted bx right mid 7 mm, 7mm 3+4 Concordant at baseline; no biopsy at exit Concordant at biopsy and exit Left mid No biopsy at exit Discordant at baseline; no biopsy at exit. Left mid Targeted bx left Concordant at exit mid 4 mm, 3mm, 1mm
44 4 mm 3+4 I R033 P 1 mm 3+3 right lateral apex 2 mm 3+3 right mid 7 mm 3+3 right apex R034 D 1 mm 3+3 left para-anterior apex 4 mm 3+4 mid-apex 1 mm 3+3 left medial anterior apex 1 mm 3+3 left medial anterior base 1 mm 3+3 left medial anterior apex 1 mm 3+3 right medial anterior apex 1 mm 3+4 left lateral 1 mm 3+4 right medial posterior apex 6 mm 3+3 right targeted R035 P 1 mm 3+3 left NK 1 mm 3+3 left NK 1 mm 3+3 right NK 1 mm 3+3 right NK R036 P 1.5 mm 3+3 mid-base 4 mm 3+3 right paraposterior apex Right mid-base Mid apex Mid-base: 4 mm 3+3 Concordant at baseline and exit Left mid-base No biopsy at exit Concordant at baseline; no biopsy at exit. Right mid-apex Targeted bx right posterior 5 mm 4+3 Targeted bx right posterior 1 mm 4+3 Exited study before taking medication as wanted to conceive. Concordant at baseline and exit Right mid No biopsy at exit Concordant at baseline. Exited study before taking 11
45 5 mm 3+3 right paraposterior base 5 mm 3+3 right paraposterior base 1 mm 3+3 right paraposterior base 12 mm 3+3 right medialposterior apex 3 mm 3+3 right medialposterior base 1 mm 3+3 right apex 4 mm 3+3 right apex 6 mm 3+3 right apex R037 P 4mm, 3mm, 3mm, 2 mm 3+4 right R038 P 8mm, 1 mm 3+4 right anterior 3 mm 3+3 right medial R039 D 3 mm 3+3 left lateral 8 mm 3+3 right lateral 5 mm 3+3 right lateral 4 mm 3+3 right lateral 1 mm 3+3 left medial posterior apex Right mid Left mid Targeted bx left 5 mm 3+4 Targeted bx right 4 mm 3+4 Right mid-apex Targeted bx right anterior 9mm, 7mm, 3.5 mm 3+4 study medication o have radical prostatectomy due to upgrade of external histology on UCLH pathology. Radical prostatectomy showed Gleason (maximal 4 + 3). Concordant at baseline and exit Concordant at baseline and exit Right mid No biopsy at exit Concordant at baseline, no biopsy at exit R040 D 2 mm 3+3 right para- Right mid-base No biopsy at exit Concordant at 12
46 anterior apex 1 mm 3+3 right midanterior apex 6 mm 3+3 right medial posterior apex 3 mm 3+3 right medial posterior base 3 mm 3+4 right peripheral zone R041 D 0.3 mm 3+3 left posterior 3 mm 3+3 left posterior 3 mm 3+3 left posterior 3 mm 3+3 left mid 1 mm 3+3 left mid 1 mm 3+3 left anterior 0.3 mm 3+3 left anterior R042 P 1 mm 3+3 right lateral base 3 mm 3+4 right lateral mid 5 mm 3+3 right para mid 2 mm 3+3 right para apex 1 mm 3+3 left lateral mid 4 mm 3+4 left lateral apex 3 mm 3+4 left para mid 4 mm 3+4 left para apex 4 mm 3+4 left apex baseline, no biopsy at exit Left mid No biopsy at exit Concordant at baseline, no biopsy at exit Left apex Left apex 1 mm 3+3 Concordant at baseline and exit 13
47 Supplementary table ACCEPTED 4 : PSA changes MANUSCRIPT in man allocated to placebo and dutasteride Treatment Number of men in group Change in Lesion Volume Placebo 2 Significant reduction ( 20%) Placebo 12 Stable lesion (20% reduction to increase of 20%) Placebo 6 Significant increase (> 20%) Dutasteride 15 Significant reduction ( 20%) Dutasteride 5 Stable lesion (20% reduction to increase of 20%) Dutasteride 0 Significant increase (> 20%) Median change in absolute PSA at 6 months n/a 14
48
Natural Hair Transplant Medical Center, Inc Dove Street, Suite #250, Newport Beach, CA Phone
 Natural Hair Transplant Medical Center, Inc. 1000 Dove Street, Suite #250, Newport Beach, CA 92660 Phone-949-622-6969 Finasteride (PROPECIA ) Acknowledgement Finasteride is an oral medication, manufactured
Natural Hair Transplant Medical Center, Inc. 1000 Dove Street, Suite #250, Newport Beach, CA 92660 Phone-949-622-6969 Finasteride (PROPECIA ) Acknowledgement Finasteride is an oral medication, manufactured
EUROPEAN UROLOGY 57 (2010)
") EUROPEAN UROLOGY 57 (2010) 123 131 available at www.sciencedirect.com journal homepage: www.europeanurology.com Benign Prostatic Hyperplasia The Effects of Combination Therapy with Dutasteride and Tamsulosin
EUROPEAN UROLOGY 57 (2010) 123 131 available at www.sciencedirect.com journal homepage: www.europeanurology.com Benign Prostatic Hyperplasia The Effects of Combination Therapy with Dutasteride and Tamsulosin
Clinical impact of type I and type II 5 alpha-reductase inhibition in prostatic disease: review and update 아주대학교김선일
 Clinical impact of type I and type II 5 alpha-reductase inhibition in prostatic disease: review and update 아주대학교김선일 Development of 5ARI Discovery of 5AR type I and type II Pharmacodynamic and pharmacokinetic
Clinical impact of type I and type II 5 alpha-reductase inhibition in prostatic disease: review and update 아주대학교김선일 Development of 5ARI Discovery of 5AR type I and type II Pharmacodynamic and pharmacokinetic
Elements for a Public Summary. Overview of disease epidemiology
 VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Benign prostatic hyperplasia (BPH) (an increase in size of the prostate that is not cancerous) is the most prevalent of all diseases
VI.2 VI.2.1 Elements for a Public Summary Overview of disease epidemiology Benign prostatic hyperplasia (BPH) (an increase in size of the prostate that is not cancerous) is the most prevalent of all diseases
M0BCore Safety Profile. Pharmaceutical form(s)/strength: 5 mg SE/H/PSUR/0002/006 Date of FAR:
/strength: 5 mg SE/H/PSUR/0002/006 Date of FAR:") M0BCore Safety Profile Active substance: Finasteride Pharmaceutical form(s)/strength: 5 mg P-RMS: SE/H/PSUR/0002/006 Date of FAR: 16.05.2014 4.3 Contraindications Finasteride is not indicated for use in
M0BCore Safety Profile Active substance: Finasteride Pharmaceutical form(s)/strength: 5 mg P-RMS: SE/H/PSUR/0002/006 Date of FAR: 16.05.2014 4.3 Contraindications Finasteride is not indicated for use in
Comparison of Clinical Efficacy of Finasteride and Dutasteride as 5-alpha Reductase Inhibitor
 대한남성과학회지 : 제 30 권제 1 호 2012 년 4 월 Korean J Androl. Vol. 30, No. 1, April 2012 http://dx.doi.org/10.5534/kja.2012.30.1.45 Comparison of Clinical Efficacy of Finasteride and Dutasteride as 5-alpha Reductase
대한남성과학회지 : 제 30 권제 1 호 2012 년 4 월 Korean J Androl. Vol. 30, No. 1, April 2012 http://dx.doi.org/10.5534/kja.2012.30.1.45 Comparison of Clinical Efficacy of Finasteride and Dutasteride as 5-alpha Reductase
The effect of dutasteride on intraprostatic dihydrotestosterone concentrations in men with benign prostatic hyperplasia
 ORIGINAL ARTICLE (27) 1, 149 154 & 27 Nature Publishing Group All rights reserved 1365-7852/7 $3. www.nature.com/pcan The effect of dutasteride on intraprostatic dihydrotestosterone concentrations in men
ORIGINAL ARTICLE (27) 1, 149 154 & 27 Nature Publishing Group All rights reserved 1365-7852/7 $3. www.nature.com/pcan The effect of dutasteride on intraprostatic dihydrotestosterone concentrations in men
FINASTERIDE (PROPECIA, PROSCAR) SIDE EFFECT & CONSENT FORM
 SIDE EFFECT & CONSENT FORM") 750 West Broadway Street Suite 905 Vancouver, BC M5Z 1K1 FAX: (604) 648-9003 vancouveroffice@donovanmedical.com FINASTERIDE (PROPECIA, PROSCAR) SIDE EFFECT & CONSENT FORM What is finasteride? Finasteride
750 West Broadway Street Suite 905 Vancouver, BC M5Z 1K1 FAX: (604) 648-9003 vancouveroffice@donovanmedical.com FINASTERIDE (PROPECIA, PROSCAR) SIDE EFFECT & CONSENT FORM What is finasteride? Finasteride
Efficacy and Safety of Long-TermTreatment with the Dual 5a-Reductase Inhibitor Dutasteride in Men with Symptomatic Benign Prostatic Hyperplasia
 European Urology European Urology 46 (2004) 488 495 Efficacy and Safety of Long-TermTreatment with the Dual 5a-Reductase Inhibitor Dutasteride in Men with Symptomatic Benign Prostatic Hyperplasia Frans
European Urology European Urology 46 (2004) 488 495 Efficacy and Safety of Long-TermTreatment with the Dual 5a-Reductase Inhibitor Dutasteride in Men with Symptomatic Benign Prostatic Hyperplasia Frans
european urology 55 (2009)
") european urology 55 (2009) 461 471 available at www.sciencedirect.com journal homepage: www.europeanurology.com Benign Prostatic Hyperplasia The Influence of Baseline Parameters on Changes in International
european urology 55 (2009) 461 471 available at www.sciencedirect.com journal homepage: www.europeanurology.com Benign Prostatic Hyperplasia The Influence of Baseline Parameters on Changes in International
Prostate enlargement, also known as benign prostatic hyperplasia
 REPORTS Differences in Alpha Blocker Usage Among Enlarged Prostate Patients Receiving Combination Therapy with 5ARIs Michael Naslund, MD, MBA; Libby Black, PharmD; Michael Eaddy, PharmD, PhD; LaKeasha
REPORTS Differences in Alpha Blocker Usage Among Enlarged Prostate Patients Receiving Combination Therapy with 5ARIs Michael Naslund, MD, MBA; Libby Black, PharmD; Michael Eaddy, PharmD, PhD; LaKeasha
It is estimated that 24% to 90% of US men older than the age of
 REPORTS Finasteride Versus Dutasteride: A Real-world Economic Evaluation Thomas C. Fenter, MD; M. Chris Runken, PharmD; Libby Black, PharmD; Michael Eaddy, PharmD, PhD It is estimated that 24% to 90% of
REPORTS Finasteride Versus Dutasteride: A Real-world Economic Evaluation Thomas C. Fenter, MD; M. Chris Runken, PharmD; Libby Black, PharmD; Michael Eaddy, PharmD, PhD It is estimated that 24% to 90% of
PHYSICIANS CIRCULAR FINASTERIDE PROSCAR. Tablet 5-Alpha Reductase Inhibitor
 PHYSICIANS CIRCULAR FINASTERIDE PROSCAR Tablet 5-Alpha Reductase Inhibitor FINASTERIDE (PROSCAR) a synthetic 4-azasteroid compound, is a specific inhibitor of Type II 5α-reductase, an intracellular enzyme
PHYSICIANS CIRCULAR FINASTERIDE PROSCAR Tablet 5-Alpha Reductase Inhibitor FINASTERIDE (PROSCAR) a synthetic 4-azasteroid compound, is a specific inhibitor of Type II 5α-reductase, an intracellular enzyme
population Completed double-blind 458 (67.7) 445 (65.0) study n (%)
 445 (65.0) study n (%)") Study No: ARIA3002 Year 4 Title: A Randomized, Double-Blind, Placebo-Controlled, Two Year Parallel Group Study of the Efficacy and Safety of GI198745 0.5mg in the Treatment and Prevention of Progression
Study No: ARIA3002 Year 4 Title: A Randomized, Double-Blind, Placebo-Controlled, Two Year Parallel Group Study of the Efficacy and Safety of GI198745 0.5mg in the Treatment and Prevention of Progression
Current status of 5α-reductase inhibitors in the management of lower urinary tract symptoms and BPH
 World J Urol (2010) 28:9 15 DOI 10.1007/s00345-009-0493-y TOPIC PAPER Current status of 5α-reductase inhibitors in the management of lower urinary tract symptoms and BPH Stavros Gravas Matthias Oelke Received:
World J Urol (2010) 28:9 15 DOI 10.1007/s00345-009-0493-y TOPIC PAPER Current status of 5α-reductase inhibitors in the management of lower urinary tract symptoms and BPH Stavros Gravas Matthias Oelke Received:
Oncologia Molecular, Porto, Portugal; 3 WSS im. L. Rydygiera, Krakow, Poland;
 The effects of combination therapy with dutasteride plus tamsulosin on clinical outcomes in men with symptomatic benign prostatic hyperplasia: 4- year post hoc analysis of European men in the CombAT study
The effects of combination therapy with dutasteride plus tamsulosin on clinical outcomes in men with symptomatic benign prostatic hyperplasia: 4- year post hoc analysis of European men in the CombAT study
1001 West Broadway, Vancouver, BC V6H 4B1. Topical Finasteride
 1001 West Broadway, Vancouver, BC V6H 4B1 Topical Finasteride 1 Topical finasteride is a solution containing the drug finasteride typically sold under the brand names Propecia and Proscar. The Finasteride
1001 West Broadway, Vancouver, BC V6H 4B1 Topical Finasteride 1 Topical finasteride is a solution containing the drug finasteride typically sold under the brand names Propecia and Proscar. The Finasteride
Update on the use of dutasteride in the management of benign prostatic hypertrophy
 REVIEW Update on the use of dutasteride in the management of benign prostatic hypertrophy Joe Miller Thomas Tarter Division of Urology, Southern Illinois University School of Medicine, Springfield, IL,
REVIEW Update on the use of dutasteride in the management of benign prostatic hypertrophy Joe Miller Thomas Tarter Division of Urology, Southern Illinois University School of Medicine, Springfield, IL,
Elements for a public summary
 VI.2 VI.2.1 Elements for a public summary Overview of disease epidemiology Prostate gland enlargement is a common condition as men get older. Also called benign prostatic hyperplasia (BPH) and prostatic
VI.2 VI.2.1 Elements for a public summary Overview of disease epidemiology Prostate gland enlargement is a common condition as men get older. Also called benign prostatic hyperplasia (BPH) and prostatic
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Enlarged prostate (EP), also known as benign prostatic
, also known as benign prostatic") REPORTS A Large Retrospective Analysis of Acute Urinary Retention and Prostate-related Surgery in BPH Patients Treated with 5-alpha Reductase Inhibitors: Dutasteride Versus Finasteride Muta M. Issa, MD,
REPORTS A Large Retrospective Analysis of Acute Urinary Retention and Prostate-related Surgery in BPH Patients Treated with 5-alpha Reductase Inhibitors: Dutasteride Versus Finasteride Muta M. Issa, MD,
Issues. What is a low testosterone? Who needs testosterone therapy? Benefits/adverse effects of testosterone replacement Treatment options
 Male Hypogonadism Jauch Symposium Waterloo, IA May 17, 2013 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any proprietary entity producing
Male Hypogonadism Jauch Symposium Waterloo, IA May 17, 2013 Janet A. Schlechte, M.D. Disclosure of Financial Relationships Janet A. Schlechte, M.D. has no relationships with any proprietary entity producing
Benign prostatic hyperplasia (BPH), which leads to an
, which leads to an") REPORTS 5-Alpha Reductase Inhibitors in Men With an Enlarged Prostate: An Evaluation of Outcomes and Therapeutic Alternatives Michael Naslund, MD, MBA; Timothy S. Regan, BPharm, RPh, CPh; Christine Ong,
REPORTS 5-Alpha Reductase Inhibitors in Men With an Enlarged Prostate: An Evaluation of Outcomes and Therapeutic Alternatives Michael Naslund, MD, MBA; Timothy S. Regan, BPharm, RPh, CPh; Christine Ong,
SITE NAME: ISF DOCUMENT VERSION CHECKLIST Complete yes or no to confirm the presence or absence of each document specified.
 1. TRIAL MANAGEMENT CTC Contact List 8 29/07/2016 Y N CTC Contact List (superseded) 7 29/09/2015 Y N CTC Contact List (superseded) 6 24/02/2015 Y N CTC Contact List (superseded) 5 03/09/2014 Y N CTC Contact
1. TRIAL MANAGEMENT CTC Contact List 8 29/07/2016 Y N CTC Contact List (superseded) 7 29/09/2015 Y N CTC Contact List (superseded) 6 24/02/2015 Y N CTC Contact List (superseded) 5 03/09/2014 Y N CTC Contact
Second Quarter 2018 Results Call Corporate Update & Financial Results. August 7, 2018
 Second Quarter 2018 Results Call Corporate Update & Financial Results August 7, 2018 Forward-Looking Statements BioCryst s presentation may contain forward-looking statements, including statements regarding
Second Quarter 2018 Results Call Corporate Update & Financial Results August 7, 2018 Forward-Looking Statements BioCryst s presentation may contain forward-looking statements, including statements regarding
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION. 20 June 2012
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 20 June 2012 CINRYZE 500 units, 2100 IU, powder and solvent for solution for injection B/2 bottles (CIP code: 218
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 20 June 2012 CINRYZE 500 units, 2100 IU, powder and solvent for solution for injection B/2 bottles (CIP code: 218
Date Effective 4/21/2008 Identification
 OHSU Research Integrity Office Human Research Protection Program Policies & Procedures Title: Research with Medical Devices Date Effective 4/21/2008 Identification Supersedes P&P dated: Page 1 of BACKGROUND
OHSU Research Integrity Office Human Research Protection Program Policies & Procedures Title: Research with Medical Devices Date Effective 4/21/2008 Identification Supersedes P&P dated: Page 1 of BACKGROUND
Effect of Dutasteride on the Risk of Prostate Cancer
 The new england journal of medicine original article Effect of on the Risk of Prostate Cancer Gerald L. Andriole, M.D., David G. Bostwick, M.D., Otis W. Brawley, M.D., Leonard G. Gomella, M.D., Michael
The new england journal of medicine original article Effect of on the Risk of Prostate Cancer Gerald L. Andriole, M.D., David G. Bostwick, M.D., Otis W. Brawley, M.D., Leonard G. Gomella, M.D., Michael
FINCAR Tablets (Finasteride)
") Published on: 10 Jul 2014 FINCAR Tablets (Finasteride) Composition FINCAR Tablets Each film-coated tablet contains: Finasteride USP - 5 mg Dosage Form Tablet Pharmacology Pharmacodynamics Mechanism of
Published on: 10 Jul 2014 FINCAR Tablets (Finasteride) Composition FINCAR Tablets Each film-coated tablet contains: Finasteride USP - 5 mg Dosage Form Tablet Pharmacology Pharmacodynamics Mechanism of
Policy for the commissioning of arthroscopic shoulder decompression surgery for the management of Pure Subacromial Shoulder Impingement
 Policy for the commissioning of arthroscopic shoulder decompression surgery for the management of Pure Subacromial Shoulder Impingement Version of: December 2018 Version Number: V 0.1 Changes Made: Policy
Policy for the commissioning of arthroscopic shoulder decompression surgery for the management of Pure Subacromial Shoulder Impingement Version of: December 2018 Version Number: V 0.1 Changes Made: Policy
Assessment of the LifeVac, an anti-choking device, on a human cadaver with complete airway obstruction
 Accepted Manuscript Assessment of the LifeVac, an anti-choking device, on a human cadaver with complete airway obstruction Mimi Juliano MA, CCC-SLP, Robert Domingo PHD, Mary S. Mooney PT, DPT, Alex Trupiano
Accepted Manuscript Assessment of the LifeVac, an anti-choking device, on a human cadaver with complete airway obstruction Mimi Juliano MA, CCC-SLP, Robert Domingo PHD, Mary S. Mooney PT, DPT, Alex Trupiano
Concussion: where are we now?
 Exeter Sports Medicine conference 2018 Concussion: where are we now? Dr Simon Kemp Medical Services Director, Rugby Football Union @drsimonkemp simonkemp@rfu.com Disclosures of interest Medical Services
Exeter Sports Medicine conference 2018 Concussion: where are we now? Dr Simon Kemp Medical Services Director, Rugby Football Union @drsimonkemp simonkemp@rfu.com Disclosures of interest Medical Services
2. QUALITATIVE AND QUANTITATIVE COMPOSITION
 AVODART SOFT CAPSULES 0.5 MG 1. NAME OF THE MEDICINAL PRODUCT AVODART 0.5 mg capsules, soft. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 0.5 mg dutasteride. For excipients, see 6.1.
AVODART SOFT CAPSULES 0.5 MG 1. NAME OF THE MEDICINAL PRODUCT AVODART 0.5 mg capsules, soft. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 0.5 mg dutasteride. For excipients, see 6.1.
Gynaecomastia. Benign breast conditions information provided by Breast Cancer Care
 Gynaecomastia This booklet tells you about gynaecomastia. It explains what gynaecomastia is, what causes it, how it s diagnosed and what will happen if it needs to be treated or followed up. Benign breast
Gynaecomastia This booklet tells you about gynaecomastia. It explains what gynaecomastia is, what causes it, how it s diagnosed and what will happen if it needs to be treated or followed up. Benign breast
Testosterone Hormone Replacement Drug Class Prior Authorization Protocol
 Testosterone Hormone Replacement Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective date: April 1, 2018 This policy has been developed through
Testosterone Hormone Replacement Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective date: April 1, 2018 This policy has been developed through
Introduction. 1 Policy
 Policies for the Commissioning of Healthcare Policy for the commissioning of arthroscopic shoulder decompression surgery for the management of Pure Subacromial Shoulder Impingement Policy Number 48 (Pan
Policies for the Commissioning of Healthcare Policy for the commissioning of arthroscopic shoulder decompression surgery for the management of Pure Subacromial Shoulder Impingement Policy Number 48 (Pan
HHS Public Access Author manuscript Int J Cardiol. Author manuscript; available in PMC 2016 April 15.
 FITBIT : AN ACCURATE AND RELIABLE DEVICE FOR WIRELESS PHYSICAL ACTIVITY TRACKING Keith M. Diaz 1, David J. Krupka 1, Melinda J Chang 1, James Peacock 1, Yao Ma 2, Jeff Goldsmith 2, Joseph E. Schwartz 1,
FITBIT : AN ACCURATE AND RELIABLE DEVICE FOR WIRELESS PHYSICAL ACTIVITY TRACKING Keith M. Diaz 1, David J. Krupka 1, Melinda J Chang 1, James Peacock 1, Yao Ma 2, Jeff Goldsmith 2, Joseph E. Schwartz 1,
LJMU Research Online
 LJMU Research Online Kimergård, A, Breindahl, T, Hindersson, P and McVeigh, J The composition of anabolic steroids from the illicit market is largely unknown: implications for clinical case reports (Commentary)
LJMU Research Online Kimergård, A, Breindahl, T, Hindersson, P and McVeigh, J The composition of anabolic steroids from the illicit market is largely unknown: implications for clinical case reports (Commentary)
Updates on Anti-doping and TUE Management in Paralympic Sport
 International Paralympic Committee Updates on Anti-doping and TUE Management in Paralympic Sport Matthew Fedoruk, Ph.D. March 15, 2018 PyeongChang 2018 IPC Medical / Sports Science Committee Workshops
International Paralympic Committee Updates on Anti-doping and TUE Management in Paralympic Sport Matthew Fedoruk, Ph.D. March 15, 2018 PyeongChang 2018 IPC Medical / Sports Science Committee Workshops
Update on Acute Stroke Management
 Update on Acute Stroke Management ACC Rockies, Banff March 2014 Brian Buck, MD MSc FRCPC Division of Neurology, Department of Medicine University of Alberta Disclosures None relevant to contents of presentation
Update on Acute Stroke Management ACC Rockies, Banff March 2014 Brian Buck, MD MSc FRCPC Division of Neurology, Department of Medicine University of Alberta Disclosures None relevant to contents of presentation
Insight into male menopause'
 Insight into male menopause' Dr Mark Vanderpump MD FRCP Consultant Endocrinologist Clinics: Tuesday PM Mark Vanderpump Consultant Physician and Endocrinologist Introduction Serum total and free testosterone
Insight into male menopause' Dr Mark Vanderpump MD FRCP Consultant Endocrinologist Clinics: Tuesday PM Mark Vanderpump Consultant Physician and Endocrinologist Introduction Serum total and free testosterone
2. QUALITATIVE AND QUANTITATIVE COMPOSITION
 AVODART SOFT CAPSULES 0.5 MG 1. NAME OF THE MEDICINAL PRODUCT Avodart 0.5 mg capsules, soft. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 0.5 mg dutasteride. For excipients, see 6.1.
AVODART SOFT CAPSULES 0.5 MG 1. NAME OF THE MEDICINAL PRODUCT Avodart 0.5 mg capsules, soft. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 0.5 mg dutasteride. For excipients, see 6.1.
Age gradient in the cost-effectiveness of bicycle helmets Kopjar B, Wickizer T M
 Age gradient in the cost-effectiveness of bicycle helmets Kopjar B, Wickizer T M Record Status This is a critical abstract of an economic evaluation that meets the criteria for inclusion on NHS EED. Each
Age gradient in the cost-effectiveness of bicycle helmets Kopjar B, Wickizer T M Record Status This is a critical abstract of an economic evaluation that meets the criteria for inclusion on NHS EED. Each
Study No.: Title: Rationale: Phase: Study Period: Study Design: Centres: Indication: Treatment: Objectives:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Validation of Measurements from a ZephIR Lidar
 Validation of Measurements from a ZephIR Lidar Peter Argyle, Simon Watson CREST, Loughborough University, Loughborough, United Kingdom p.argyle@lboro.ac.uk INTRODUCTION Wind farm construction projects
Validation of Measurements from a ZephIR Lidar Peter Argyle, Simon Watson CREST, Loughborough University, Loughborough, United Kingdom p.argyle@lboro.ac.uk INTRODUCTION Wind farm construction projects
Study Management SM STANDARD OPERATING PROCEDURE FOR Interactions with the Institutional Review Board (IRB)
") Study Management SM 302.00 STANDARD OPERATING PROCEDURE FOR Interactions with the Institutional Review Board (IRB) Approval: Nancy Paris, MS, FACHE President and CEO 24 May 2017 (Signature and Date) Approval:
Study Management SM 302.00 STANDARD OPERATING PROCEDURE FOR Interactions with the Institutional Review Board (IRB) Approval: Nancy Paris, MS, FACHE President and CEO 24 May 2017 (Signature and Date) Approval:
5.1 Introduction. Learning Objectives
 Learning Objectives 5.1 Introduction Statistical Process Control (SPC): SPC is a powerful collection of problem-solving tools useful in achieving process stability and improving capability through the
Learning Objectives 5.1 Introduction Statistical Process Control (SPC): SPC is a powerful collection of problem-solving tools useful in achieving process stability and improving capability through the
SUMMARY OF PRODUCT CHARACTERISTICS
 1. NAME OF THE MEDICINAL PRODUCT Avodart 0.5 mg soft capsules. SUMMARY OF PRODUCT CHARACTERISTICS 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 0.5 mg dutasteride. Excipient with known
1. NAME OF THE MEDICINAL PRODUCT Avodart 0.5 mg soft capsules. SUMMARY OF PRODUCT CHARACTERISTICS 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 0.5 mg dutasteride. Excipient with known
Denise L Seman City of Youngstown
 Denise L Seman City of Youngstown The control chart is one of the most important tools of quality control for laboratory data. A control chart is a specific kind of run chart that allows unusual change
Denise L Seman City of Youngstown The control chart is one of the most important tools of quality control for laboratory data. A control chart is a specific kind of run chart that allows unusual change
The Effect of a Seven Week Exercise Program on Golf Swing Performance and Musculoskeletal Screening Scores
 The Effect of a Seven Week Exercise Program on Golf Swing Performance and Musculoskeletal Screening Scores 2017 Mico Hannes Olivier Bachelor of Sport Science Faculty of Health Sciences and Medicine Bond
The Effect of a Seven Week Exercise Program on Golf Swing Performance and Musculoskeletal Screening Scores 2017 Mico Hannes Olivier Bachelor of Sport Science Faculty of Health Sciences and Medicine Bond
Effect of dutasteride 0.5 mg/d in men with androgenetic alopecia recalcitrant to finasteride
 Report Effect of dutasteride 0.5 mg/d in men with androgenetic alopecia recalcitrant to finasteride Jae Yoon Jung 1, MD, Je Ho Yeon 1, MD, Jee Woong Choi 1, MD, Soon Hyo Kwon 1, MD, Beom Joon Kim 2, MD,
Report Effect of dutasteride 0.5 mg/d in men with androgenetic alopecia recalcitrant to finasteride Jae Yoon Jung 1, MD, Je Ho Yeon 1, MD, Jee Woong Choi 1, MD, Soon Hyo Kwon 1, MD, Beom Joon Kim 2, MD,
University of Bath. DOI: /bjsports Publication date: Document Version Early version, also known as pre-print
 Citation for published version: Taylor, AE, Kemp, S, Trewartha, G & Stokes, KA 2014, 'Scrum injury risk in English professional rugby union' British Journal of Sports Medicine, vol. 48, pp. 1066-1068.
Citation for published version: Taylor, AE, Kemp, S, Trewartha, G & Stokes, KA 2014, 'Scrum injury risk in English professional rugby union' British Journal of Sports Medicine, vol. 48, pp. 1066-1068.
BEST FINASTERIDE IN INDIA
 Best Finasteride In India page 1/5 BEST FINASTERIDE IN INDIA Topical for sale, tab leg 5mg nutrition, 88 tablet 5mg, tablets 5mg 48, cancer prostate and grade high. 5mg enlargement surgery recovery breast,
Best Finasteride In India page 1/5 BEST FINASTERIDE IN INDIA Topical for sale, tab leg 5mg nutrition, 88 tablet 5mg, tablets 5mg 48, cancer prostate and grade high. 5mg enlargement surgery recovery breast,
Safety and Tolerability of the Dual 5a-Reductase Inhibitor Dutasteride in thetreatment of Benign Prostatic Hyperplasia
 European Urology European Urology 44 (2003) 82 88 Safety and Tolerability of the Dual 5a-Reductase Inhibitor in thetreatment of Benign Prostatic Hyperplasia Gerald L. Andriole a,*,1, Roger Kirby b a Division
European Urology European Urology 44 (2003) 82 88 Safety and Tolerability of the Dual 5a-Reductase Inhibitor in thetreatment of Benign Prostatic Hyperplasia Gerald L. Andriole a,*,1, Roger Kirby b a Division
1. Review and approval of the consent document is a responsibility that FDA assigns to the IRB with jurisdiction
 Medical College of Wisconsin/Froedtert Hospital Guidance on Negotiating Consent Document Language For Clinical Trial Sponsors 1. Review and approval of the consent document is a responsibility that FDA
Medical College of Wisconsin/Froedtert Hospital Guidance on Negotiating Consent Document Language For Clinical Trial Sponsors 1. Review and approval of the consent document is a responsibility that FDA
PRODUCT INFORMATION TESTOVIRON DEPOT. (testosterone enanthate)
") PRODUCT INFORMATION TESTOVIRON DEPOT (testosterone enanthate) NAME OF THE MEDICINE Testosterone enanthate is designated chemically as 17 beta-heptanoyloxy-4-androstene-3- one. The empirical formula of
PRODUCT INFORMATION TESTOVIRON DEPOT (testosterone enanthate) NAME OF THE MEDICINE Testosterone enanthate is designated chemically as 17 beta-heptanoyloxy-4-androstene-3- one. The empirical formula of
Public Assessment Report. Scientific discussion. Dutasteride Regiomedica 0.5 mg capsules, soft (dutasteride) NL/H/2861/001/DC.
 NL/H/2861/001/DC.") Public Assessment Report Scientific discussion Dutasteride Regiomedica 0.5 mg capsules, soft (dutasteride) NL/H/2861/001/DC Date: 2 July 2014 This module reflects the scientific discussion for the approval
Public Assessment Report Scientific discussion Dutasteride Regiomedica 0.5 mg capsules, soft (dutasteride) NL/H/2861/001/DC Date: 2 July 2014 This module reflects the scientific discussion for the approval
Analysis of Variance. Copyright 2014 Pearson Education, Inc.
 Analysis of Variance 12-1 Learning Outcomes Outcome 1. Understand the basic logic of analysis of variance. Outcome 2. Perform a hypothesis test for a single-factor design using analysis of variance manually
Analysis of Variance 12-1 Learning Outcomes Outcome 1. Understand the basic logic of analysis of variance. Outcome 2. Perform a hypothesis test for a single-factor design using analysis of variance manually
Reducing Breath-hold Artifacts on Abdominal MR
 Reducing Breath-hold Artifacts on Abdominal MR Primary Authors: C. Daniel Johnson, MD James Ellis, MD Mark Baker, MD Joe Veniero, MD, PhD Purpose and Rationale This project aims to reduce the incidence
Reducing Breath-hold Artifacts on Abdominal MR Primary Authors: C. Daniel Johnson, MD James Ellis, MD Mark Baker, MD Joe Veniero, MD, PhD Purpose and Rationale This project aims to reduce the incidence
TESTOFEN HUMAN CLINICAL TRIAL GENCOR PACIFIC, INC. Copyright 2006 by Gencor Pacific, Inc.
 GENCOR PACIFIC, INC. 920 E. Orangethorpe Avenue, Suite B, Anaheim, CA 92801 Ph: 714.870.8723 714.870.8724 efax: 732.875.0306 drjit@gencorpacific.com gita@gencorpacific.com www.gencorpacific.com TESTOFEN
GENCOR PACIFIC, INC. 920 E. Orangethorpe Avenue, Suite B, Anaheim, CA 92801 Ph: 714.870.8723 714.870.8724 efax: 732.875.0306 drjit@gencorpacific.com gita@gencorpacific.com www.gencorpacific.com TESTOFEN
Dutasteride Avodart Softgel Capsule
 Dutasteride Avodart Softgel Capsule PRODUCT DESCRIPTION Dutasteride (Avodart ) is available as dull yellow, opaque, oblong soft gelatin capsules containing a clear, colourless to slightly yellow liquid.
Dutasteride Avodart Softgel Capsule PRODUCT DESCRIPTION Dutasteride (Avodart ) is available as dull yellow, opaque, oblong soft gelatin capsules containing a clear, colourless to slightly yellow liquid.
PACKAGE LEAFLET: INFORMATION FOR THE USER. FINASTERIDE 1 MG FILM-COATED TABLETS (finasteride)
") PACKAGE LEAFLET: INFORMATION FOR THE USER FINASTERIDE 1 MG FILM-COATED TABLETS (finasteride) Read all of this leaflet carefully before you start taking this medicine because it contains important information
PACKAGE LEAFLET: INFORMATION FOR THE USER FINASTERIDE 1 MG FILM-COATED TABLETS (finasteride) Read all of this leaflet carefully before you start taking this medicine because it contains important information
CPR Quality During OHCA Transport
 CPR Quality During OHCA Transport Sheldon Cheskes, MD CCFP(EM) FCFP Medical Director, Sunnybrook Centre for Prehospital Medicine Associate Professor, Division of Emergency Medicine, University of Toronto
CPR Quality During OHCA Transport Sheldon Cheskes, MD CCFP(EM) FCFP Medical Director, Sunnybrook Centre for Prehospital Medicine Associate Professor, Division of Emergency Medicine, University of Toronto
SUMMARY OF PRODUCT CHARACTERISTICS
 SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Deratos 0.5 mg capsules, soft 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 0.5 mg dutasteride. For the full list
SUMMARY OF PRODUCT CHARACTERISTICS 1. NAME OF THE MEDICINAL PRODUCT Deratos 0.5 mg capsules, soft 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 0.5 mg dutasteride. For the full list
Bioequivalence: Saving money with generic drugs
 The Right Stuff: Appropriate Mathematics for All Students Promoting the use of materials that engage students in meaningful activities that promote the effective use of technology to support mathematics,
The Right Stuff: Appropriate Mathematics for All Students Promoting the use of materials that engage students in meaningful activities that promote the effective use of technology to support mathematics,
WHY IS PREVENTION IMPORTANT?
 A GUIDE TO TRUST THE POWER OF PREVENTION < 2 > WHY IS PREVENTION IMPORTANT? Hereditary angioedema (HAE) symptoms can range in severity. Some attacks may be mild or temporarily disabling, but others can
A GUIDE TO TRUST THE POWER OF PREVENTION < 2 > WHY IS PREVENTION IMPORTANT? Hereditary angioedema (HAE) symptoms can range in severity. Some attacks may be mild or temporarily disabling, but others can
The Science of. NUTRICULA Longevity Journal
 32 December, 2011 The Science of 33 NUTRICULA Longevity Journal As men age, there is often a decline in libido and sexual function. This decline frequently interferes in intimacy within romantic relationships,
32 December, 2011 The Science of 33 NUTRICULA Longevity Journal As men age, there is often a decline in libido and sexual function. This decline frequently interferes in intimacy within romantic relationships,
Analysis of Foot Pressure Variation with Change in Stride Length
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 13, Issue 1 Ver. IV (Oct. 214), PP 46-51 Dr. Charudatta V. Shinde, M.S. MCh ( Orthopaedics ), Dr. Weijie
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-853, p-issn: 2279-861.Volume 13, Issue 1 Ver. IV (Oct. 214), PP 46-51 Dr. Charudatta V. Shinde, M.S. MCh ( Orthopaedics ), Dr. Weijie
Ventilating the Sick Lung Mike Dougherty RRT-NPS
 Ventilating the Sick Lung 2018 Mike Dougherty RRT-NPS Goals and Objectives Discuss some Core Principles of Ventilation relevant to mechanical ventilation moving forward. Compare and Contrast High MAP strategies
Ventilating the Sick Lung 2018 Mike Dougherty RRT-NPS Goals and Objectives Discuss some Core Principles of Ventilation relevant to mechanical ventilation moving forward. Compare and Contrast High MAP strategies
Supplementary Online Content
 Supplementary Online Content McEvoy JP, Byerly M, Hamer RM, et al. Effectiveness of Paliperidone Palmitate vs Haloperidol Decanoate for Maintenance Treatment of Schizophrenia: a Randomized Clinical Trial.
Supplementary Online Content McEvoy JP, Byerly M, Hamer RM, et al. Effectiveness of Paliperidone Palmitate vs Haloperidol Decanoate for Maintenance Treatment of Schizophrenia: a Randomized Clinical Trial.
SOP 407: PROTOCOL DEVIATIONS AND UNANTICIPATED PROBLEMS
 University of Oklahoma Office of Human Research Participant Protection : PROTOCOL DEVIATIONS AND UNANTICIPATED PROBLEMS 1. POLICY Protocol deviations and unanticipated problems may be discovered in a variety
University of Oklahoma Office of Human Research Participant Protection : PROTOCOL DEVIATIONS AND UNANTICIPATED PROBLEMS 1. POLICY Protocol deviations and unanticipated problems may be discovered in a variety
Summary. Introduction. Dow Stough, MD
 Original Contribution Blackwell Publishing ORIGINAL Inc CONTRIBUTION Dutasteride improves male pattern hair loss in a randomized study in identical twins Dow Stough, MD The Dermatology Clinic, Hot Springs,
Original Contribution Blackwell Publishing ORIGINAL Inc CONTRIBUTION Dutasteride improves male pattern hair loss in a randomized study in identical twins Dow Stough, MD The Dermatology Clinic, Hot Springs,
Efficacy and tolerability of the dual 5a-reductase inhibitor, dutasteride, in the treatment of benign prostatic hyperplasia in African-American men
 (2006) 9, 432 438 & 2006 Nature Publishing Group All rights reserved 1365-7852/06 $30.00 ORIGINAL ARTICLE www.nature.com/pcan Efficacy and tolerability of the dual 5a-reductase inhibitor, dutasteride,
(2006) 9, 432 438 & 2006 Nature Publishing Group All rights reserved 1365-7852/06 $30.00 ORIGINAL ARTICLE www.nature.com/pcan Efficacy and tolerability of the dual 5a-reductase inhibitor, dutasteride,
Flip-flop footwear with a moulded foot-bed for the treatment of foot pain: a randomised controlled trial
 Flip-flop footwear with a moulded foot-bed for the treatment of foot pain: a randomised controlled trial Dr. Martin Spink, Ms. Angela Searle and Dr. Vivienne Chuter Podiatry department Faculty of Health
Flip-flop footwear with a moulded foot-bed for the treatment of foot pain: a randomised controlled trial Dr. Martin Spink, Ms. Angela Searle and Dr. Vivienne Chuter Podiatry department Faculty of Health
Legendre et al Appendices and Supplements, p. 1
 Legendre et al. 2010 Appendices and Supplements, p. 1 Appendices and Supplement to: Legendre, P., M. De Cáceres, and D. Borcard. 2010. Community surveys through space and time: testing the space-time interaction
Legendre et al. 2010 Appendices and Supplements, p. 1 Appendices and Supplement to: Legendre, P., M. De Cáceres, and D. Borcard. 2010. Community surveys through space and time: testing the space-time interaction
Adverse effects of anabolic androgenic steroids abuse on gonadal function, glucose homeostasis and cardiovascular function
 Adverse effects of anabolic androgenic steroids abuse on gonadal function, glucose homeostasis and cardiovascular function Associate Professor Caroline Kistorp, Ph.D Department of Internal Medicine, Herlev
Adverse effects of anabolic androgenic steroids abuse on gonadal function, glucose homeostasis and cardiovascular function Associate Professor Caroline Kistorp, Ph.D Department of Internal Medicine, Herlev
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT 2 QUALITATIVE AND QUANTITATIVE COMPOSITION
 SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Dutasteride 0.5 mg Capsules, Soft 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 0.5 mg dutasteride. For the full list
SUMMARY OF PRODUCT CHARACTERISTICS 1 NAME OF THE MEDICINAL PRODUCT Dutasteride 0.5 mg Capsules, Soft 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 0.5 mg dutasteride. For the full list
7.0 DEVIATION and EXCEPTION of a PREVIOUSLY APPROVED PROTOCOL
 7.0 DEVIATION and EXCEPTION of a PREVIOUSLY APPROVED PROTOCOL 7.1 OBJECTIVE To describe the policies and procedures for reviewing a modification or a deviation/exception to a previously approved protocol.
7.0 DEVIATION and EXCEPTION of a PREVIOUSLY APPROVED PROTOCOL 7.1 OBJECTIVE To describe the policies and procedures for reviewing a modification or a deviation/exception to a previously approved protocol.
Revision UCL Reconstruction. No Disclosures
 Revision UCL Reconstruction George A. Paletta, Jr., MD The Orthopedic Center of St. Louis Head Team Orthopedic Surgeon St. Louis Cardinals No Disclosures 1 From Yesterday to Today Since Dr. Jobe s landmark
Revision UCL Reconstruction George A. Paletta, Jr., MD The Orthopedic Center of St. Louis Head Team Orthopedic Surgeon St. Louis Cardinals No Disclosures 1 From Yesterday to Today Since Dr. Jobe s landmark
University of Pennsylvania Institutional Review Board. Reliance Agreement Guidance: Penn as Central IRB FAQ
 Reliance Agreement Guidance: Penn as Central IRB FAQ This document is designed to answer questions frequently asked by individuals who want to know more about Penn s policies and procedures related to
Reliance Agreement Guidance: Penn as Central IRB FAQ This document is designed to answer questions frequently asked by individuals who want to know more about Penn s policies and procedures related to
OXYGEN FOR ADULTS IN ACUTE CARE
 PATIENT GROUP DIRECTION FOR THE ADMINISTRATION OF OXYGEN FOR ADULTS IN ACUTE CARE ALL CLINICAL DIVISIONS ADULT CARE STATEMENT The staff indicated in Staff Group may administer oxygen in the two detailed
PATIENT GROUP DIRECTION FOR THE ADMINISTRATION OF OXYGEN FOR ADULTS IN ACUTE CARE ALL CLINICAL DIVISIONS ADULT CARE STATEMENT The staff indicated in Staff Group may administer oxygen in the two detailed
Issue in IRB Approvals:
 Issue in IRB Approvals: What are the obligations of investigators and the IRB in maintaining IRB approval? What are the consequences of a lapse in IRB approval? How does the IRB evaluate lapses in approval?
Issue in IRB Approvals: What are the obligations of investigators and the IRB in maintaining IRB approval? What are the consequences of a lapse in IRB approval? How does the IRB evaluate lapses in approval?
DETERMINATION OF SAFETY REQUIREMENTS FOR SAFETY- RELATED PROTECTION AND CONTROL SYSTEMS - IEC 61508
 DETERMINATION OF SAFETY REQUIREMENTS FOR SAFETY- RELATED PROTECTION AND CONTROL SYSTEMS - IEC 61508 Simon J Brown Technology Division, Health & Safety Executive, Bootle, Merseyside L20 3QZ, UK Crown Copyright
DETERMINATION OF SAFETY REQUIREMENTS FOR SAFETY- RELATED PROTECTION AND CONTROL SYSTEMS - IEC 61508 Simon J Brown Technology Division, Health & Safety Executive, Bootle, Merseyside L20 3QZ, UK Crown Copyright
BBS Fall Conference, 16 September Use of modeling & simulation to support the design and analysis of a new dose and regimen finding study
 BBS Fall Conference, 16 September 211 Use of modeling & simulation to support the design and analysis of a new dose and regimen finding study Didier Renard Background (1) Small molecule delivered by lung
BBS Fall Conference, 16 September 211 Use of modeling & simulation to support the design and analysis of a new dose and regimen finding study Didier Renard Background (1) Small molecule delivered by lung
Evaluating the evidence using GRADE. Peter Morley E th October 2012
 1 Evaluating the evidence using GRADE Peter Morley E3 2015 19 th October 2012 2 Conflict of interest disclosure Commercial/industry Evidence Evaluation Expert (ILCOR/AHA) Potential intellectual conflicts
1 Evaluating the evidence using GRADE Peter Morley E3 2015 19 th October 2012 2 Conflict of interest disclosure Commercial/industry Evidence Evaluation Expert (ILCOR/AHA) Potential intellectual conflicts
Chapter 5: Methods and Philosophy of Statistical Process Control
 Chapter 5: Methods and Philosophy of Statistical Process Control Learning Outcomes After careful study of this chapter You should be able to: Understand chance and assignable causes of variation, Explain
Chapter 5: Methods and Philosophy of Statistical Process Control Learning Outcomes After careful study of this chapter You should be able to: Understand chance and assignable causes of variation, Explain
FieldStrength. Using MotionTrak for motion correction in body imaging. Application tips
 FieldStrength Publication for the Philips MRI Community Issue 35 September / October 2008 Using MotionTrak for motion correction in body imaging Application tips This article is part of Field Strength
FieldStrength Publication for the Philips MRI Community Issue 35 September / October 2008 Using MotionTrak for motion correction in body imaging Application tips This article is part of Field Strength
Policy Number: 42 Title: Investigational Devices Date of Last Revision: 06/12/2008; 07/22/2010; 05/29/2013; 05/01/2016; 10/16/2018
 University of California, Irvine Human Research Protections Standard Operating Policies and Procedures Policy Number: 42 Title: Investigational Devices Date of Last Revision: 06/12/2008; 07/22/2010; 05/29/2013;
University of California, Irvine Human Research Protections Standard Operating Policies and Procedures Policy Number: 42 Title: Investigational Devices Date of Last Revision: 06/12/2008; 07/22/2010; 05/29/2013;
Identification and Screening of Scenarios for LOPA. Ken First Dow Chemical Company Midland, MI
 Identification and Screening of Scenarios for LOPA Ken First Dow Chemical Company Midland, MI 1 Layers of Protection Analysis (LOPA) LOPA is a semi-quantitative tool for analyzing and assessing risk. The
Identification and Screening of Scenarios for LOPA Ken First Dow Chemical Company Midland, MI 1 Layers of Protection Analysis (LOPA) LOPA is a semi-quantitative tool for analyzing and assessing risk. The
Systematic Review and Meta-analysis of Bicycle Helmet Efficacy to Mitigate Head, Face and Neck Injuries
 Systematic Review and Meta-analysis of Bicycle Helmet Efficacy to Mitigate Head, Face and Neck Injuries Prudence Creighton & Jake Olivier MATHEMATICS & THE UNIVERSITY OF NEW STATISTICS SOUTH WALES Creighton
Systematic Review and Meta-analysis of Bicycle Helmet Efficacy to Mitigate Head, Face and Neck Injuries Prudence Creighton & Jake Olivier MATHEMATICS & THE UNIVERSITY OF NEW STATISTICS SOUTH WALES Creighton
Reporting an Unanticipated Problem Involving Risks to Subjects or Others (UPIRTSO) to the IRB
 to the IRB") INSTITUTIONAL REVIEW BOARD (IRB) OFFICE FOR HUMAN RESEARCH PROTECTION Reporting an Unanticipated Problem Involving Risks to Subjects or Others (UPIRTSO) to the IRB UPIRTSO Flowchart Content Applies To
INSTITUTIONAL REVIEW BOARD (IRB) OFFICE FOR HUMAN RESEARCH PROTECTION Reporting an Unanticipated Problem Involving Risks to Subjects or Others (UPIRTSO) to the IRB UPIRTSO Flowchart Content Applies To
Salisbury District Hospital
 The Effectiveness of Peroneal Nerve Functional Electrical STimulation (FES) for the Reduction of Bradykinesia in Parkinson s Disease: A Pragmatic Two Site Feasibility Study for a Single Blinded Randomised
The Effectiveness of Peroneal Nerve Functional Electrical STimulation (FES) for the Reduction of Bradykinesia in Parkinson s Disease: A Pragmatic Two Site Feasibility Study for a Single Blinded Randomised
Yale University Human Research Protection Program
 Yale University Human Research Protection Program HRPP Policy 700 Noncompliance, Suspension and Termination Responsible Office Office of Research Administration Effective Date: February 10, 2009 Responsible
Yale University Human Research Protection Program HRPP Policy 700 Noncompliance, Suspension and Termination Responsible Office Office of Research Administration Effective Date: February 10, 2009 Responsible
Academic Grant CPR process monitors provided by Zoll. conflict of interest to declare
 Comparison of Bystander Fatigue and CPR Quality when Using Ui Continuous Chest Compressions Versus 30:2 Compressions to Ventilations: A Randomized Cross over over Trial CAEP Niagara Falls 2012 CAEP St
Comparison of Bystander Fatigue and CPR Quality when Using Ui Continuous Chest Compressions Versus 30:2 Compressions to Ventilations: A Randomized Cross over over Trial CAEP Niagara Falls 2012 CAEP St
School of Social and Community Medicine, University of Bristol Division of Global Public Health, UC San Diego
 This work was partially supported through a research grant from Gilead Sciences. Gilead had no influence on the design, analysis and content of the study Presentation based on work by Peter Vickerman,
This work was partially supported through a research grant from Gilead Sciences. Gilead had no influence on the design, analysis and content of the study Presentation based on work by Peter Vickerman,
New Zealand Data Sheet
 New Zealand Data Sheet 1. PRODUCT NAME TEROD 500 micrograms soft gelatin capsules. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 500 micrograms of dutasteride. For the full list of
New Zealand Data Sheet 1. PRODUCT NAME TEROD 500 micrograms soft gelatin capsules. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains 500 micrograms of dutasteride. For the full list of
save percentages? (Name) (University)
 (University)") 1 IB Maths Essay: What is the correlation between the height of football players and their save percentages? (Name) (University) Table of Contents Raw Data for Analysis...3 Table 1: Raw Data...3 Rationale
1 IB Maths Essay: What is the correlation between the height of football players and their save percentages? (Name) (University) Table of Contents Raw Data for Analysis...3 Table 1: Raw Data...3 Rationale
EMERGENCY USE 03/02/2016
 DUKE UNIVERSITY HEALTH SYSTEM Human Research Protection Program EMERGENCY USE 03/02/2016 Emergency Exemption for an Investigational Drug or Biologic or Unapproved Device Emergency use of an investigational
DUKE UNIVERSITY HEALTH SYSTEM Human Research Protection Program EMERGENCY USE 03/02/2016 Emergency Exemption for an Investigational Drug or Biologic or Unapproved Device Emergency use of an investigational
(y9. &i?r, JUL t Certified-Return Receipt Requested WARNING LE7TER
 ... (y9 &i?r, DEPARTMENT OF HEALTH a HUMAN SERVICES Public Health Service Food and Drug Admini~ation Center for Biologics Evaluation and Rem 1401 Rockville Pike Rockville MD 20852-1448 JUL t 71997 Certified-Return
... (y9 &i?r, DEPARTMENT OF HEALTH a HUMAN SERVICES Public Health Service Food and Drug Admini~ation Center for Biologics Evaluation and Rem 1401 Rockville Pike Rockville MD 20852-1448 JUL t 71997 Certified-Return
THERAPEUTIC USE EXEMPTION POLICY U.S. ANTI-DOPING AGENCY. Effective JANUARY 1, (Revised June 21, 2018)
") THERAPEUTIC USE EXEMPTION POLICY U.S. ANTI-DOPING AGENCY Effective JANUARY 1, 2018 (Revised June 21, 2018) 1. GENERAL PRINCIPLES The United States Anti-Doping Agency ( USADA ) Policy for Therapeutic Use
THERAPEUTIC USE EXEMPTION POLICY U.S. ANTI-DOPING AGENCY Effective JANUARY 1, 2018 (Revised June 21, 2018) 1. GENERAL PRINCIPLES The United States Anti-Doping Agency ( USADA ) Policy for Therapeutic Use