Diving and Altitude Medicine
|
|
|
- Bennett Mitchell
- 5 years ago
- Views:
Transcription


1 Diving and Altitude Medicine David Regis, MD CAPT MC (UMO/DMO/SMO) USN
2 Background Estimated to be 1.5 to 3.5 million certified divers in the U.S. ( K new/year) >100 million people visit > 2,500m ( 8,000 ft) annually Many travel the world to prime destinations Each carries risks of both travel and environment. Pressure (Direct and Indirect Effects) Temperature
3 Trip of a Lifetime Mentality Usually large investment in time, money and training Pressure to make the dives/summit Overestimations of abilities Incorrect assumptions WRT fitness etc. Competition within group Leader/dive master reluctant to split group. Fear of being left behind Climbing/Trekking commercial outfits: Published itinerary s are average schedules Not meant to prevent AMS Inflexible schedule = left behind Flexible schedule = acclimatize within a day and can continue Underestimating the first case of AMS by the trip leader


4 We are all saturation divers at 1 atm


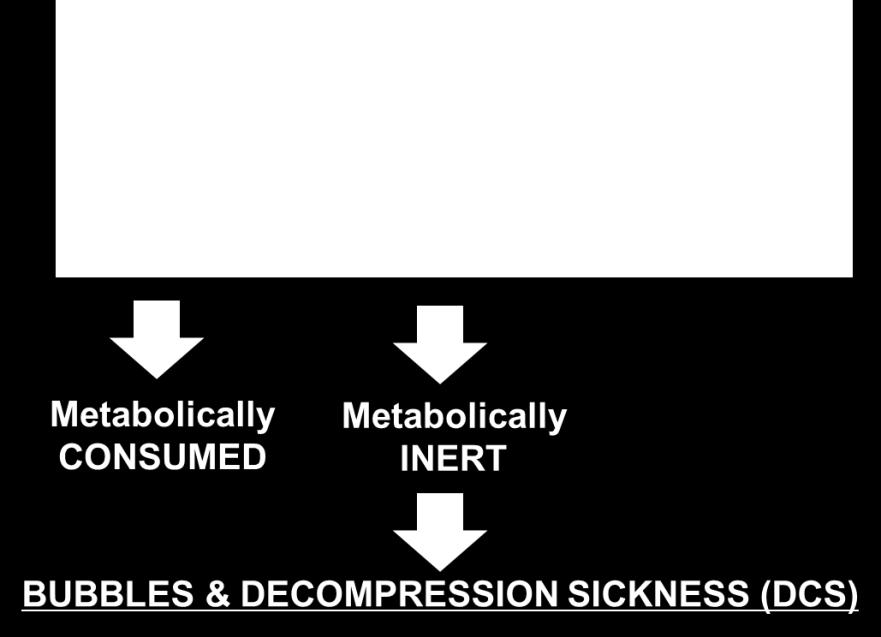
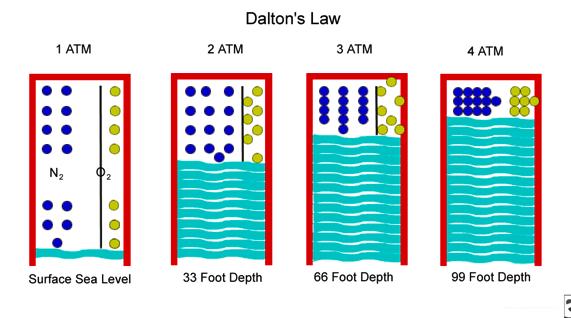
5 Dalton s Law : P O2 + P N2 =P AIR + = Metabolically CONSUMED Metabolically INERT BUBBLES & DECOMPRESSION SICKNESS (DCS)

6 Boyle s Law

7 DIVING
8 Introduction 3-9/100,000 diving deaths per year Drowning most common cause (60%) Pre-disposing risk factors/mitigators Fitness Age Concurrent illness (acute or chronic) Sex? Training All risks directly related to effects of pressure
9 Risk Factors/Mitigators Fitness Being physically fit reduces risk of Decompression Sickness (DCS) Age May be more directly related to BMI Some related to above plus acquisition of chronic illnesses Dive certification usually not allowed until 12 yrs
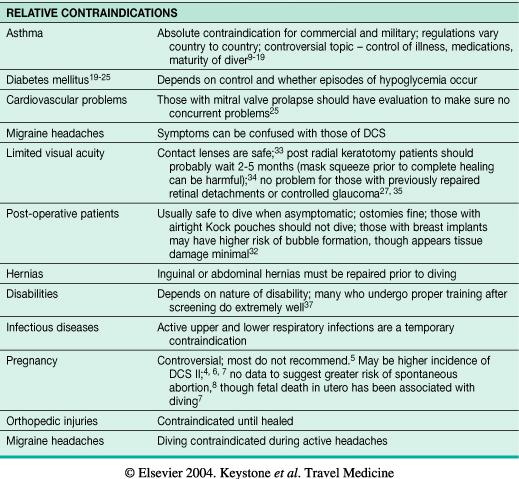
10 Risk Factors/Mitigators Concurrent illness/conditions Short/long term meds may preclude from diving Dehydration; Alcohol; obesity; cold PFO controversial: 20% of population; 40% DCS cases Women No clear relationship with DCS: Risk 0-3x vs Men Menses DOES NOT increase risk of shark attack Pregnancy contraindicated
11
12
13



14 Training (or lack there of)

15 DIVING PROBLEMS
16 Barotrauma (Dysbarism) Otic Sinus Dental GI Mask Pulmonary (POIS = POPS)


17 Otic Barotrauma Squeeze On descent Reverse Squeeze On Ascent Other related issues Alternobaric Vertigo Usually on ascent Brief, self limited Caloric Vertigo Colder water Brief, self limited


18 Sinus/Tooth (Barodontalgia) Squeeze -Anatomy -Allergies/Illness -Medications -Bad dentition -Filling defect -May need DDS/DMD

 -Not clearing properly -Will")
19 GI Distention/Mask Squeeze -Swallowing Air on Descent -Vigorous/Freq Clearing -Burping/distention Ascent -Ill fitting mask (too tight) -Not clearing properly -Will resolve on own

20 Pulmonary Over-Inflation/Pressure Syndrome (POIS/POPS) Due to pulmonary barotrauma Breath-holding or too rapid ascent Expanding gas bubbles into blood stream Risk greatest near the surface 4 important entities: Arterial Gas Embolism 2 nd most common cause of death in divers Usually occurs within 10 minutes of surfacing Pneumomediastinum Pneumothorax Subcutaneous emphysema Tx: Oxygen, Recompression NEEDS F/U TO R/O Underlying cause

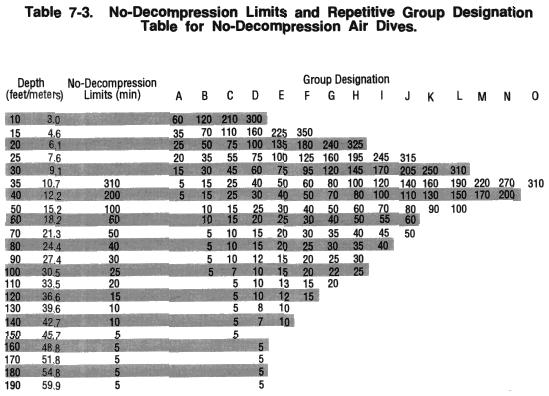
21 Decompression Sickness Due To Rapid Decrease in Pressure Tissues/Blood Supersaturated Bubble Formation Not all w/bubbles get DCS Vessel occlusion Tissue trapping Inflammatory Cascade USN Dive Manual Revision 6
:e50079: Decompression")

22 Decompression Sickness PLoS One. 2012;7(11):e50079: Decompression Illness: Clinical Aspects of 5278 Consecutive Cases Treated in a Single Hyperbaric Unit


23 Decompression Sickness Caisson s Disease Categorized into Type I and Type II but argument for more of a spectrum of Illness No dive is without DCS risk but generally < 1-2% range for recreational if follow training/tables.


24 Decompression Sickness DCS Type I Affects bones/joints manifesting as pain = The Bends Skin/lymphatics manifesting as Cutis Marmorata Skin marbling Itching
25 Decompression Sickness DCS Type II Life/Limb Threatening Emergency Neurologic Peripheral and CNS symptoms Cardiopulmonary ( Chokes ) Overwhelming Lung/CV congestion Usually from deep dive blow-up Vestibular ( Staggers ) Most common with Heliox Diving

26 DCS Treatment High flow O 2 Rest Hydrate Treat Symptoms Pain control Steroids not recom. For serious DCS pt likely unstable RECOMPRESSION TX

27 Nitrogen Tissue Saturation
 Tissue Metabolism (Low Oxygen Tension) Utilizes concentration gradient Used to Treat & Prevent DCS CAPT Albert R. Behnke Jr. USN (ret.")
28 Oxygen Window N 2 N 2 N 2 N 2 N 2 N 2 O 2 N 2 N 2 O 2 N 2 N 2 N 2 N 2 N 2 N 2 N 2 N 2 SURROUNDING BLOOD/TISSUE Oxygen N 2 O 2 N 2 O 2 N 2 N 2 O 2 O N 2 2 N 2 O 2 O 2 O 2 N 2 N 2 O 2 O 2 N 2 N 2 N 2 Lungs/Exhalation (Hi Oxygen Tension) Tissue Metabolism (Low Oxygen Tension) Utilizes concentration gradient Used to Treat & Prevent DCS CAPT Albert R. Behnke Jr. USN (ret.)
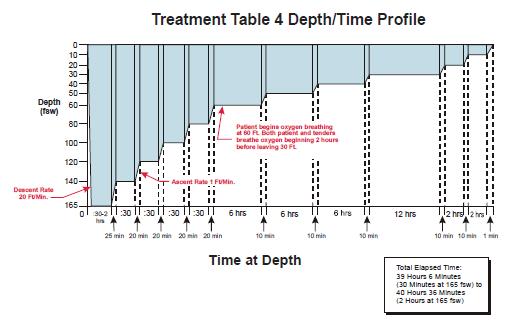
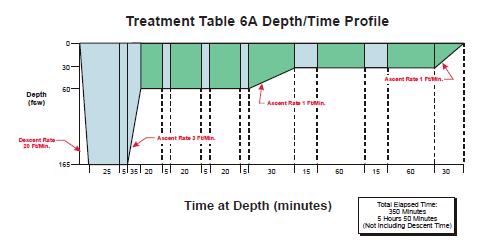
29 More Rapid Decompression Treatments with Oxygen

30 Gas Problems

31 Nitrogen Narcosis Rapture of the Deep Generally > 100 fsw Martini s Law Loosened inhibitions Agitation Tunnel Vision Tinnitus/Rushing Sound Poor Judgement Simple Tasks Become Difficult LOC Resolves with ascent or He

32 Hypoxia/Hyperoxia Issue with Nitrox Diving and Rebreathers Hypoxia Similar to Narcosis Hyperoxia VENTID-C Visual Ear Nausea/Vomitting Twitching/tingling Irritability Dizziness Convulsions
33 Carbon Dioxide/Monoxide Poisoning Usually from bad air source Compressor intakes near exhausts CO 2 also from overbreathing equipment Hyperventilation CO 2 Scrubber Failure (Rebreathers) Increased RR Irritability Sweating/N/V Drowsiness HA Difficulty Concentrating Seizures (CO 2 ) LOC
34 Flying After Diving Most commercial flights pressurized to 8000 feet USN Dive Manual has recommendations Each certifying organization has their own as well In general as follows: No decompression diving: 12 hours Decompression Diving: 24 hours or longer Multiple days of multiple dives: 24 hours
35 Returning To Diving After... Otic BT: When healed and can clear. Eye surgery (Lasek): 1 month w/opth approv Pulmonary BT (known cause): 1 month + w/u 6 months for traumatic PTX with neg w/u +PPD/LTBI post Tx and neg w/u Abd Surgery: After 3 months and neg w/u Successful DCS Tx post 1 Tx Type I: 2d-1 week - Type II: 30+ days NOTE: These are for guidelines only. Consult a DMO on case by case basis. US Navy Manual of the Medical Department (MANMED) Ch
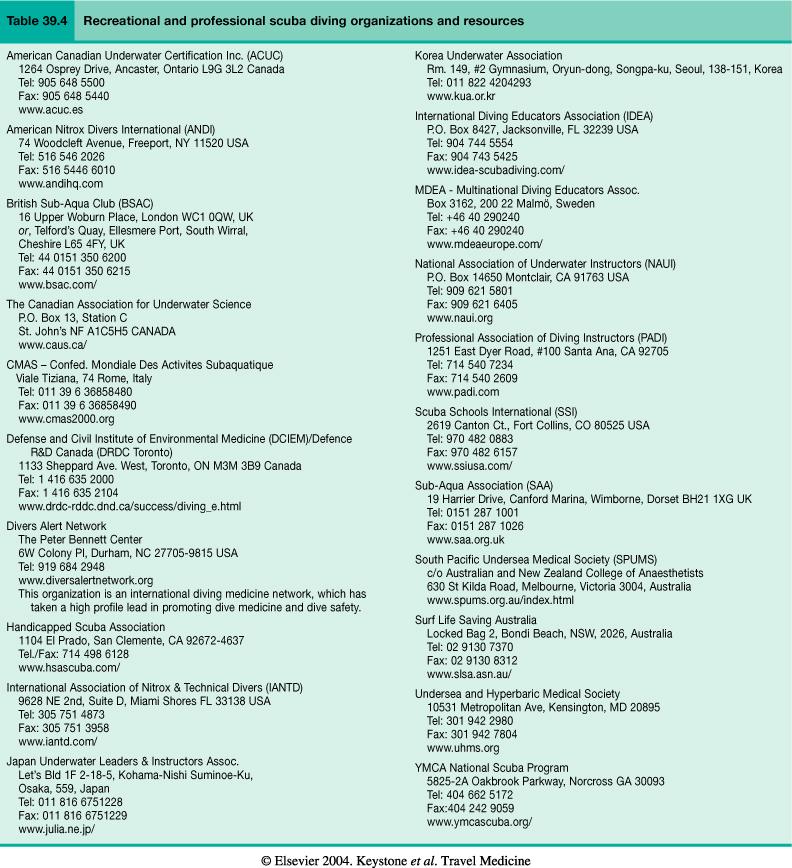
36 Diving Key Points The hazards of diving and the sophistication of advising travelers are underappreciated by the travel medicine community Many with underlying chronic illnesses or with disabilities may dive Barotrauma results from the uncontrolled expansion of gas within body compartments Decompression sickness results from too rapid a return to atmospheric pressure Consider doing a detailed neuro exam on any traveling diver Encourage refresher courses for infrequent divers. There are many organizations and resources for diving travelers and travel medicine physicians
37

38 Problems with Altitude

39 Problems with Altitude
40 High Altitude Definitions Over 1500m (4900 ft) Moderate altitude is m (6600 to 11,500 ft) Mild tissue hypoxia from low arterial PO2 and altitude sickness is common Very high altitude is m (18,000 ft) Arterial oxygen saturation is not maintained HAPE and HACE most common in this range Extreme altitude is over 5500m (18,000 ft) Successful long-term acclimatization is impossible
: 247")
41 Journal of Travel Medicine 2013; Volume 20 (Issue 4):


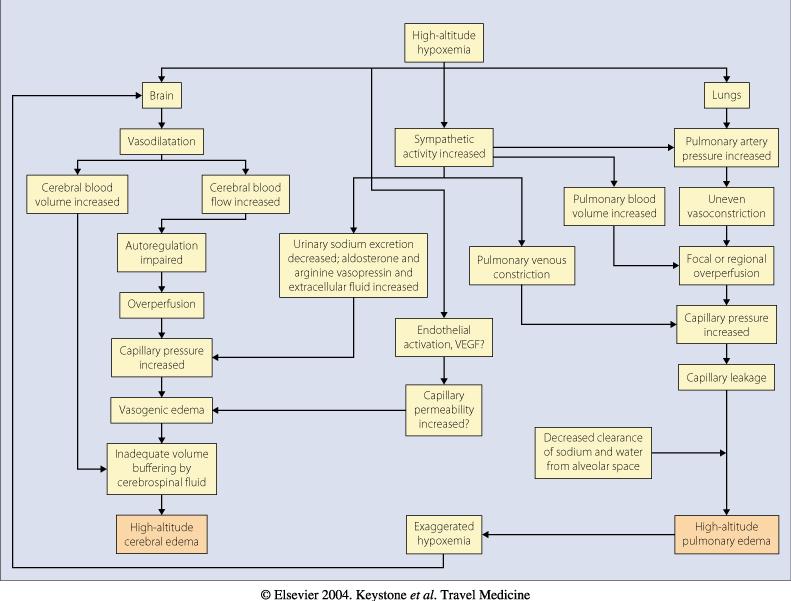
42 Boyle & Dalton... Again! 1 ATM 0.5 ATM 0.25 ATM 0.16 ATM
43
44 Temperature and other issues Decreases up to 12 F (6.5 C) per 3300ft (1000m). Effects of hypothermia can be additive HAPE Frostbite UV exposure increases 4%/1000ft (300m) Sunburn UV keratoconjunctivitis Cataracts Dry air predisposes to dehydration/dry airways
45 Demographics Persons Activities N High altitude Everyone Skiing/Air Travel Millions m Touring (5,000-11,500) Trekking Mountaineering Very High altitude m (11,500-18,000) Healthy adults Skiing Trekking Mountaineering Many thousands Extreme altitude 5500 m Extreme athletes Mountaineering Few thousands > 18,000 feet
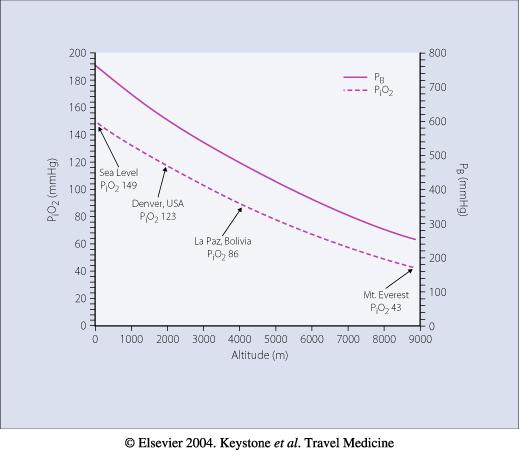
46 Acclimatization is Key! If you could immediately dissaparate to the summit of Everest (P i O 2 43) LOC w/in 2 minutes. Normal Physiologic Changes: Hyperventilation (Resp Alkalosis) SOB w/exercise ( VO 2 max 10%/1000m > 1500m) Increased urination (Bicarb excretion) Increased Cerebral Blood Flow (HA?) Increased Hgb Changed breathing pattern at night (Cheyne-Stokes) Awakening frequently at night/headache (up to 80%)

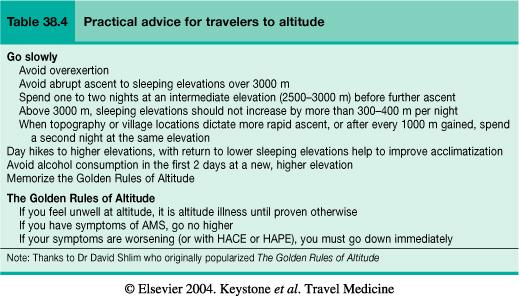
47 Acclimatization 8,000 to 10,000 ft for most This line can move up the 400m/day (1300ft/d)* If you get too far above the line it only gets worse, no acclimatization possible Avoid heavy excersion Don t ascend when symptomatic * Am J Respir Crit Care Med 2012; 185: The Acclimatization Line Sick Well




48 Transition Line

49 HIGH ALTITUDE SYNDROMES
 Pulmonary High altitude pulmonary edema (HAPE) Pathophysiology of hypoxia in otherwise healthy")
50 High Altitude Syndromes Cerebral and pulmonary syndromes that develop in non-acclimatized persons Cerebral Acute mountain sickness (AMS) High altitude cerebral edema (HACE) Pulmonary High altitude pulmonary edema (HAPE) Pathophysiology of hypoxia in otherwise healthy persons

51 High Altitude Syndromes Lancet 359, Issue 9303, 26 January 2002 Pages
52 High Altitude Syndromes Rate of ascent (>1300 ft/day) Altitude Altitude reached and slept at Incidence of AMS at m is 10-40% 25-50% above 4000m Variable susceptibility Past history of AMS is best predictor Muted response & desaturation to hypoxia Slight decrease in risk after age 50 Physical fitness NOT protective But obesity/smoking may be a risk factor HTN, CAD and DM do not increase risk
53 Acute Mountain Sickness AMS & High-Altitude Cerebral Edema (HACE) Spectrum of disease Pathophysiology poorly understood Effects and response to hypoxia Cerebral vasodilation Impaired cerebral autoregulation Elevated capillary pressures Cytokine induced changes in BBB permiability Capillary leaks Edema Edema is what will cause herniation and death
54 AMS/HACE Occurs within 48 hrs of ascent to > 8000 ft After rapid ascent (1 day or less) Usually within hours of arrival but up to 3 days out Similar to hangover or afebrile viral illness HA that is throbbing /bilateral Anorexia, N/V Weakness, lightheadedness Often report reduced UOP (vs expected increase) Most resolve 1-2 days depending on situation Can worsen to ataxia, MS changes = HACE < 10% go on to HACE (40% mortality with limited medical care.)
55 AMS Worksheet "The Lake Louise Consensus on the Definition and Quantification of Altitude Illness" in Sutton JR, Coates G, Houston CS(Eds), Hypoxia and Mountain Medicine. Queen City Printers, Burlington, Vermont, TIME Altitude SYMPTOMS Headache + 1 other symptom = AMS 0 None 1 Mild 2 Mod 3 Severe GI 0- None 1- Nausea 2 - Mod N/V 3 - Severe
 usually sufficient Descend at first sign of HACE 0 2 if")
56 AMS/HACE Treatment No further ascent until asymptomatic Descend to lower altitude if no improvement with therapy m ( ft) usually sufficient Descend at first sign of HACE 0 2 if available
57 AMS/HACE Treatment Acetazolamide Speeds acclimatization Hastens resolution in 12-24hrs Dexamethasone Rapidly reverses symptoms 2-4 hrs Does not affect acclimatization Rebound Continue 1-2 days post descent or when MS clears No evidence for Coca leaf tea or garlic

58 AMS/HACE Treatment Gamow Bag, CERTEC, Pac Manually inflated Pressurize to mmhg above 1/3 descent Similar efficacy to O2 1 hour to effect
59 AMS/HACE Prevention Preacclimatization Acclimatization!!! Effects for AMS will last for > 1wk; 1-2d for HAPE Acetazolamide Will not mask AMS Appears 125 mg BID as effective as 250mg or 500mg QD Journal of Travel Medicine 2012; Volume 19 (Issue 5):
60
61 Acetazolamide Sulfa allergy a concern Serious allergic reactions are rare Although at increased risk, individuals with Sulfa allergy are less likely to react to Diamox than PCN allergic patients Travelers with any allergic history should test their tolerance prior to departure References: Strom BL et al. Absence of cross-reactivity between sulfonamide antibiotics and sulfonamide nonantibiotics. N Engl J Med. 2003; 349(17): Editorial: Ray WA. N Engl J Med. 2003; 349(17):
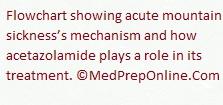
62 High Altitude Pulmonary Edema (HAPE) Incidence 0.01%-15% Genetic predisposition Pulmonary artery hypertension Exaggerated hypoxic pulmonary vasoconstriction Male Pre-existing medical conditions Pulmonary HTN Restricted pulmonary vascular bed Non-cardiogenic hydrostatic pulmonary edema
63 HAPE Occurs 2-4 days after ascent Worse at night Decreased exercise performance Dry cough Insidious onset that can quickly become fatal Productive frothy cough Severe Dyspnea HR and RR Drowsiness and other CNS symptoms
64 HAPE
65 HAPE Severity Classification Hackett PH, Roach RC: High-Altitude Medicine. In: Auerbach PS (ed): Wilderness Medicine, 4th edition; Mosby, St. Louis, MO 2001; Grade Symptoms Signs Chest X ray 1 Mild Dyspnea on exertion Dry cough Fatigue while moving uphill HR (rest) < RR (rest) < 20 Dusky nail-beds or exertional desaturation +/- localized crackles Minor exudate involving < 25% of one lung field 2 Moderate Dyspnea, weakness, fatigue on level walking Raspy cough Headache, anorexia HR RR Cyanotic nail-beds Crackles present + / - ataxia Some infiltrate involving 50% of one lung or smaller area of both lungs 3 Severe Dyspnea at rest Extreme weakness Orthopnea Productive cough HR > 110 RR > 30 Facial and nail-bed cyanosis Bilateral crackles Blood tinged sputum Stupor or coma Bilateral infiltrates > 50% of each lung
66 HAPE Treatment Descend if possible Oxygen Nifedipine if descent is NOT possible Hyperbaric treatment 1 hour increments; 3-6 hours usually May need 3 days 2 weeks for full recovery Excellent prognosis with rapid recovery May cautiously re-ascend after
67 HAPE Prevention Indicated if a history of repeated episodes Slower ascent Nifedipine Use prophylactically or at the first signs Salmeterol 50% reduction in susceptible persons

68 Other HAPE Prophylaxis Schoene - CHEST 2008; 134:

69 OTHER ALTITUDE RELATED CONDITIONS
 Altitude dependent 4%(4243m) to 50%(5360m) Descend if symptomatic; Usually resolve completely within a few")
70 Other Altitude-Related Conditions High Altitude Syncope first 24 hours No work-up needed unless recurs Focal Neurologic Deficits Unmasked conditions that need evaluation High-Altitude Retinal Hemorrhage (HARH) Altitude dependent 4%(4243m) to 50%(5360m) Descend if symptomatic; Usually resolve completely within a few weeks.
71 Other Altitude-Related Conditions Peripheral Edema Females more at risk; Evaluate for AMS Can use diuretics but caution with dehydration High-altitude cough Altitude dependent; Cold/Arid Paroxyxmal; Forceful; Purulent; Afebrile Normal exercise tolerance and exam Can have associated sore throat Symptomatic treatment UV Keratitis aka Snow Blindness Sunglasses!; Ointment; Analgesics : 24-48h to clear
72 Summary of Management * Am J Respir Crit Care Med 2012; 185:
73 * Am J Respir Crit Care Med 2012; 185:

74 CLIMBER S LITTLE HELPER Several near deaths on the world s highest peaks have shed light on a dangerous trend in mountaineering: rampant use of performance-enhancing drugs, particularly the powerful steroid dexamethasone. OUTSIDE MAGAZINE, APRIL 2013 COUNSEL YOUR PATIENTS ABOUT ILLICIT/UNREGULATED USE!!
75
76
77
78 EXTRA Slides
79 Case CC: Extreme fatigue HPI: This 39 yo male on patrol was carried down from 4800 m with complaints of a cough and extreme fatigue with exercise. He was noted to have gurgling respirations during the night. He denied dyspnea at rest, and had had no orthopnea. He had a fever of 40 C the morning of presentation, along with a moderate headache which partially responded to aspirin and/or descent. He seemed confused on arising at altitude, according to his buddy. He attempted to walk down but was able to walk only 1/2 km before needing to be carried due to fatigue and gross ataxia. PMH: no prior AMS, HACE or HAPE. Resides at sea-level, and is a marathon runner Meds: Amoxicillin, 2 doses for presumed pneumonia. Aspirin for fever and headache.
80 Case Ascent History: Trekked in from a very gradual 7-9 day ascent. x 1 night 3440 m x 1 night 4080 m X 1 night 4750 m ascended to 5500 m on a day hike x 1 night 4690 m crossed pass 5420 m Last night 4840 m Exam: Thin, shivering man. HR 110, BP 120/80, RR 30, SaO2 58% ( normal is 82-86% at 4250 m) Cardiac: tachycardic, otherwise normal Lungs: Right Middle Lobe crackles and some right-sided intercostal retractions noted. Neuro: stepped off line on tandem-gait testing. AMS scores: HA 1 Fatigue/weak 3 Sleep 1 Mental Status 2 Ataxia 2 TOTAL SX 9
81 Case Dx: HAPE HACE Tx: Nifedipine 10 mg chew, plus 10 mg swallow. SaO2 rose to 66% after nifedipine treatment. Dexamethasone 8 mg po stat. The patient was well enough to descend without additional treatment, though the Gamow bag was offered to the patient if he felt too fatigued to walk to Pangboche Plan: Nifedipine 20 mg po q 6 hours. Dexamethasone 4 mg po q 6 hours. Immediate descent. DISCUSSION Classic physically fit man Rapid ascent HAPE HACE Classic denial I cannot have altitude sickness, I am a marathon runner!" Exertion and subsequent fatigue, classic of HAPE
The Traveling Diver and Alpinist LTC Richard Ruck MD, FS, UMO Walter Reed Army Institute of Research Clinical Investigator
 The Traveling Diver and Alpinist LTC Richard Ruck MD, FS, UMO Walter Reed Army Institute of Research Clinical Investigator UNCLASSIFIED Slide 1 Disclosures Views are my own opinion, and not those of the
The Traveling Diver and Alpinist LTC Richard Ruck MD, FS, UMO Walter Reed Army Institute of Research Clinical Investigator UNCLASSIFIED Slide 1 Disclosures Views are my own opinion, and not those of the
SCUBA - self contained underwater breathing apparatus. 5 million sport scuba divers in U.S. 250, ,000 new certifications annually in U.S.
 SCUBA - self contained underwater breathing apparatus 5 million sport scuba divers in US 250,000-400,000 new certifications annually in US Diving occurs in oceans, freshwater lakes, rivers and quarries
SCUBA - self contained underwater breathing apparatus 5 million sport scuba divers in US 250,000-400,000 new certifications annually in US Diving occurs in oceans, freshwater lakes, rivers and quarries
High Altitude Pulmonary Edema (HAPE)
") High Altitude Pulmonary Edema (HAPE) HAPE is a fluid build-up in the lungs. Cases seen at altitudes as low as 8,000 ft. (e.g., Colorado ski resorts) HAPE: Some Basics Can occur in people with no other
High Altitude Pulmonary Edema (HAPE) HAPE is a fluid build-up in the lungs. Cases seen at altitudes as low as 8,000 ft. (e.g., Colorado ski resorts) HAPE: Some Basics Can occur in people with no other
Espilat Mountaineering Club
 In the name of God Espilat Mountaineering Club May 2013 MEDICAL PROBLEMS IN HIGH MOUNTAIN ENVIRONMENTS Arya Hamedanchi MD, MPH Level one International Anthropometrist International Certificate of Ski Medicine
In the name of God Espilat Mountaineering Club May 2013 MEDICAL PROBLEMS IN HIGH MOUNTAIN ENVIRONMENTS Arya Hamedanchi MD, MPH Level one International Anthropometrist International Certificate of Ski Medicine
Acute Mountain Sickness
 Innere Medizin VII / Sportmedizin Acute Mountain Sickness Peter Bärtsch www.klinikum.uni-heidelberg.de/sportmedizin AMS: Clinical Picture Symptoms: - Headache - Loss of appetite, nausea, vomiting - Dizziness
Innere Medizin VII / Sportmedizin Acute Mountain Sickness Peter Bärtsch www.klinikum.uni-heidelberg.de/sportmedizin AMS: Clinical Picture Symptoms: - Headache - Loss of appetite, nausea, vomiting - Dizziness
Environmental Injuries: The Winter Athlete. Thomas Moran, MD Primary Care Sports Medicine Fellow University of Chicago - NorthShore
 Environmental Injuries: The Winter Athlete Thomas Moran, MD Primary Care Sports Medicine Fellow University of Chicago - NorthShore Introduction Chicago Marathon >41,000 runners 2006 (36 start,48 high with
Environmental Injuries: The Winter Athlete Thomas Moran, MD Primary Care Sports Medicine Fellow University of Chicago - NorthShore Introduction Chicago Marathon >41,000 runners 2006 (36 start,48 high with
Decompression Sickness
 Decompression Sickness Kun-Lun Huang National Defense Medical Center Undersea and Hyperbaric Medical Institute Tri-Service General Hospital Department of Undersea and Hyperbaric Medicine Hazard Diving
Decompression Sickness Kun-Lun Huang National Defense Medical Center Undersea and Hyperbaric Medical Institute Tri-Service General Hospital Department of Undersea and Hyperbaric Medicine Hazard Diving
Outdoor Action Guide to High Altitude: Acclimatization and Illnesses
 Outdoor Action Guide to High Altitude: Acclimatization and Illnesses Last Page update 07/07/1999 by Rick Curtis, Director, Outdoor Action Program Navigation Back to the AEE Wilderness Safety Page OA Guide
Outdoor Action Guide to High Altitude: Acclimatization and Illnesses Last Page update 07/07/1999 by Rick Curtis, Director, Outdoor Action Program Navigation Back to the AEE Wilderness Safety Page OA Guide
1 out of every 5,555 of drivers dies in car accidents 1 out of every 7692 pregnant women die from complications 1 out of every 116,666 skydives ended
 1 out of every 5,555 of drivers dies in car accidents 1 out of every 7692 pregnant women die from complications 1 out of every 116,666 skydives ended in a fatality in 2000 1 out of every 126,626 marathon
1 out of every 5,555 of drivers dies in car accidents 1 out of every 7692 pregnant women die from complications 1 out of every 116,666 skydives ended in a fatality in 2000 1 out of every 126,626 marathon
Unit 3: The Physiology of Diving and Nitrox
 Unit 3: The Physiology of Diving and Nitrox Narcosis Decompression Sickness Physiological Effects of High Oxygen Levels Physiological Effects of High Oxygen Levels Student Performance: By the end of the
Unit 3: The Physiology of Diving and Nitrox Narcosis Decompression Sickness Physiological Effects of High Oxygen Levels Physiological Effects of High Oxygen Levels Student Performance: By the end of the
David A. Connett, DO, FACOFP, dist
 David A. Connett, DO, FACOFP, dist Disclosures Nothing to disclose including pharmaceuticals High Altitude Syndromes Acute Mountain Sickness (AMS) High Altitude Cerebral Edema (HACE) High Altitude Pulmonary
David A. Connett, DO, FACOFP, dist Disclosures Nothing to disclose including pharmaceuticals High Altitude Syndromes Acute Mountain Sickness (AMS) High Altitude Cerebral Edema (HACE) High Altitude Pulmonary
High Altitude Medical Problems
 High Altitude Medical Problems Wilderness Basics Course 2-2015 Jeffrey H. Gertsch, MD Assistant Professor of Neurosciences UCSD School of Medicine Definition/Site ISMM Definitions Altitude in Meters Altitude
High Altitude Medical Problems Wilderness Basics Course 2-2015 Jeffrey H. Gertsch, MD Assistant Professor of Neurosciences UCSD School of Medicine Definition/Site ISMM Definitions Altitude in Meters Altitude
Diving Medicine USN Diver/SEAL Submarine Overview / Tom Kersch, CAPT, MC!!
 Diving Medicine USN Diver/SEAL Submarine Overview / Tom Kersch, CAPT, MC Diving Medicine USN Diver/SEAL Submarine Overview Tom Kersch CAPT, MC SEAL Deliver Vehicle Team 1 Pearl City, HI 1 Content Attestation
Diving Medicine USN Diver/SEAL Submarine Overview / Tom Kersch, CAPT, MC Diving Medicine USN Diver/SEAL Submarine Overview Tom Kersch CAPT, MC SEAL Deliver Vehicle Team 1 Pearl City, HI 1 Content Attestation
the ACUTE MOUNTAIN SICKNESS manual
 the ACUTE MOUNTAIN SICKNESS manual AMS (Acute Mountain Sickness) at high altitude is common. It is your body s way of telling you that it is not able to adapt to the lesser oxygen it is getting. Depending
the ACUTE MOUNTAIN SICKNESS manual AMS (Acute Mountain Sickness) at high altitude is common. It is your body s way of telling you that it is not able to adapt to the lesser oxygen it is getting. Depending
b. Provide consultation service to physicians referring patients. c. Participate in weekly wound care clinic and biweekly diving medicine clinic.
 Curriculum: 1. Required clinical activities: a. Participate in HBO 2 clinical operations by monitoring daily treatment sessions and emergency on-call treatments at least 4 days/week, b. Provide consultation
Curriculum: 1. Required clinical activities: a. Participate in HBO 2 clinical operations by monitoring daily treatment sessions and emergency on-call treatments at least 4 days/week, b. Provide consultation
Outdoor Medicine 2010
 Outdoor Medicine 2010 Outdoor Medicine Preparation Priorities Common injuries and illnesses High altitude illness Preparation Itinerary Extra food and water, filter or iodine Clothes base layer, insulation,
Outdoor Medicine 2010 Outdoor Medicine Preparation Priorities Common injuries and illnesses High altitude illness Preparation Itinerary Extra food and water, filter or iodine Clothes base layer, insulation,
So What Can I do About AMS?
 So What Can I do About AMS? T he symptoms of AMS will disappear 24-36 hours after appearing if you do not continue to ascend. If the symptoms persist then the only option is to descend to a lower altitude
So What Can I do About AMS? T he symptoms of AMS will disappear 24-36 hours after appearing if you do not continue to ascend. If the symptoms persist then the only option is to descend to a lower altitude
EMS Subspecialty Certification Review Course. Learning Objectives. Question Environmental
 EMS Subspecialty Certification Review Course 1.2.5 Version: 2017 Learning Objectives Differentiate EMS treatment priorities for cold and heat related illnesses Describe EMS treatment considerations for
EMS Subspecialty Certification Review Course 1.2.5 Version: 2017 Learning Objectives Differentiate EMS treatment priorities for cold and heat related illnesses Describe EMS treatment considerations for
Successful use ofthe Gamow Hyperbaric Bag in the treatment ofaltitude illness at MountEverest
 Journal of Wilderness Medicine 1, 193-202 (1990) Successful use ofthe Gamow Hyperbaric Bag in the treatment ofaltitude illness at MountEverest SJ. KINGl* and R.R. GREENLEE2 1Departmentof Emergency Medicine,
Journal of Wilderness Medicine 1, 193-202 (1990) Successful use ofthe Gamow Hyperbaric Bag in the treatment ofaltitude illness at MountEverest SJ. KINGl* and R.R. GREENLEE2 1Departmentof Emergency Medicine,
High Altitude Concerns
 High Altitude Concerns 17 March, 2014 PRESENTED BY: John M. Davenport, Lt. Col., USAF, Ret. International Operators Conference Tampa, FL March 17 20, 2014 Welcome Aviators! High Altitude Concerns Question
High Altitude Concerns 17 March, 2014 PRESENTED BY: John M. Davenport, Lt. Col., USAF, Ret. International Operators Conference Tampa, FL March 17 20, 2014 Welcome Aviators! High Altitude Concerns Question
Immersion pulmonary oedema: is it confused with drowning?
 Immersion pulmonary oedema: is it confused with drowning? Dr Peter Wilmshurst Consultant Cardiologist Royal Stoke University Hospital & UK Diving Medical Committee Drowning and pulmonary oedema Drowning
Immersion pulmonary oedema: is it confused with drowning? Dr Peter Wilmshurst Consultant Cardiologist Royal Stoke University Hospital & UK Diving Medical Committee Drowning and pulmonary oedema Drowning
Is Your Traveler Going to High Altitude?
 Is Your Traveler Going to High Altitude? Dr. Peter Hackett First came to Nepal in 1974 Worked 3 seasons at Himalayan Rescue Association aid post Did an altitude illness survey that was published in The
Is Your Traveler Going to High Altitude? Dr. Peter Hackett First came to Nepal in 1974 Worked 3 seasons at Himalayan Rescue Association aid post Did an altitude illness survey that was published in The
2010 NPC Team Physician Conference. Russ O Connor MD, FRCPC (PMR), Dip Sport Med CASM
, Dip Sport Med CASM") 2010 NPC Team Physician Conference Russ O Connor MD, FRCPC (PMR), Dip Sport Med CASM Overview Trauma and Injury patterns and rates Resuscitation issues Altitude Cold exposure Injury Epidemiology Limited
2010 NPC Team Physician Conference Russ O Connor MD, FRCPC (PMR), Dip Sport Med CASM Overview Trauma and Injury patterns and rates Resuscitation issues Altitude Cold exposure Injury Epidemiology Limited
Over, Under, Hot and Cold. Jamie Syrett, MD Office of Prehospital Care Rochester General Health System
 Over, Under, Hot and Cold Jamie Syrett, MD Office of Prehospital Care Rochester General Health System Pulsecheck 2012 Reality EMS Under - Drowning Over - High Altitude Illness Hot - Hyperthermia Cold -
Over, Under, Hot and Cold Jamie Syrett, MD Office of Prehospital Care Rochester General Health System Pulsecheck 2012 Reality EMS Under - Drowning Over - High Altitude Illness Hot - Hyperthermia Cold -
DCI Demystified By Eric Hexdall, RN, CHRN Duke Dive Medicine
 DCI Demystified By Eric Hexdall, RN, CHRN Duke Dive Medicine Everyone who takes a formal diver training course receives at least a basic education in the signs, symptoms, etiology, and prevention of pressure-related
DCI Demystified By Eric Hexdall, RN, CHRN Duke Dive Medicine Everyone who takes a formal diver training course receives at least a basic education in the signs, symptoms, etiology, and prevention of pressure-related
O-1. American Osteopathic College of Occupational and Preventive Medicine 2013 Mid Year Educational Conference, Phoenix, Arizona February 14-17, 2013
 Administrative Information Risk Assessment: Low AEROSPACE/ OCCUPATIONAL MEDICINE BAROMETRIC CONCERNS Dr. John Campbell, DO, MPH, MFS Environmental Considerations: None Safety Considerations: None Evaluation:
Administrative Information Risk Assessment: Low AEROSPACE/ OCCUPATIONAL MEDICINE BAROMETRIC CONCERNS Dr. John Campbell, DO, MPH, MFS Environmental Considerations: None Safety Considerations: None Evaluation:
Learning Objectives 9/12/2012. Chapter 30. Environmental Emergencies. Chapter Goal
 Chapter 30 Environmental Emergencies Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with environmentally induced or exacerbated emergencies Define
Chapter 30 Environmental Emergencies Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with environmentally induced or exacerbated emergencies Define
Hyperbaric Oxygen Therapy
 1 RSPT 1410 Medical Gas Therapy Part 2: Wilkins: Chapter 38; p. 891-894 Cairo: Chapter 3, p. 78-81 2 Definitions Hyperbaric oxygen (HBO) therapy is the therapeutic use of oxygen at pressures greater than
1 RSPT 1410 Medical Gas Therapy Part 2: Wilkins: Chapter 38; p. 891-894 Cairo: Chapter 3, p. 78-81 2 Definitions Hyperbaric oxygen (HBO) therapy is the therapeutic use of oxygen at pressures greater than
American College of Occupational and Preventive Medicine 2011 Annual Meeting, Orlando, Florida, November 2, 2011
 Administrative Information Risk Assessment: Low AEROSPACE/ OCCUPATIONAL MEDICINE BAROMETRIC CONCERNS Dr. John Campbell, MFS Environmental Considerations: None Safety Considerations: None Evaluation: 50
Administrative Information Risk Assessment: Low AEROSPACE/ OCCUPATIONAL MEDICINE BAROMETRIC CONCERNS Dr. John Campbell, MFS Environmental Considerations: None Safety Considerations: None Evaluation: 50
Civil Air Patrol Auxiliary of the United States Air Force
 Mountain Flying Qualification Course Civil Air Patrol Auxiliary of the United States Air Force Physiological Effects of Altitude Physiological Effects of Altitude OXYGEN DEPRIVATION (HYPOXIA) SINUS PRESSURE
Mountain Flying Qualification Course Civil Air Patrol Auxiliary of the United States Air Force Physiological Effects of Altitude Physiological Effects of Altitude OXYGEN DEPRIVATION (HYPOXIA) SINUS PRESSURE
Challenge in High Altitude related Medical Emergency Recognize, Remedy and Risk Reduction
 Challenge in High Altitude related Medical Emergency Recognize, Remedy and Risk Reduction Dr. M K Ho Resident Consultant in Emergency Medicine Hong Kong Baptist Hospital (Statement of declare that there
Challenge in High Altitude related Medical Emergency Recognize, Remedy and Risk Reduction Dr. M K Ho Resident Consultant in Emergency Medicine Hong Kong Baptist Hospital (Statement of declare that there
Do I have AMS or am I just Knackered?
 Do I have AMS or am I just Knackered? An excellent question and one that you should always be asking yourself as you ascend. Early onset of AMS is very difficult to diagnose as the symptoms can be very
Do I have AMS or am I just Knackered? An excellent question and one that you should always be asking yourself as you ascend. Early onset of AMS is very difficult to diagnose as the symptoms can be very
DEFENCE INSTRUCTIONS AND NOTICES (Not to be communicated to anyone outside HM Service without authority)
") Title: Audience: Applies: Expires: Reference: DEFENCE INSTRUCTIONS AND NOTICES (Not to be communicated to anyone outside HM Service without authority) Guidelines for the Conduct of Adventurous Training
Title: Audience: Applies: Expires: Reference: DEFENCE INSTRUCTIONS AND NOTICES (Not to be communicated to anyone outside HM Service without authority) Guidelines for the Conduct of Adventurous Training
Altitude Good Practice Guidelines to Venture Planning and Acclimatisation for Youth Expeditions
 Registered Charity No. 1006211 Company Limited by Guarantee No. 2658616 Altitude Good Practice Guidelines to Venture Planning and Acclimatisation for Youth Expeditions [Young Explorers Trust (YET) Disclaimer:
Registered Charity No. 1006211 Company Limited by Guarantee No. 2658616 Altitude Good Practice Guidelines to Venture Planning and Acclimatisation for Youth Expeditions [Young Explorers Trust (YET) Disclaimer:
3) Water dissipates body heat about times faster than air. a) 4 b) 7 c) 20 d) 200
 Water dissipates body heat about times faster than air. a) 4 b) 7 c) 20 d) 200") PHYSICS 1) If you raise the pressure of a gas in contact with a liquid - a) Gas bubbles form b) The liquid dissolves in the gas c) The gas dissolves into the liquid d) The liquid will evaporate 2) Objects
PHYSICS 1) If you raise the pressure of a gas in contact with a liquid - a) Gas bubbles form b) The liquid dissolves in the gas c) The gas dissolves into the liquid d) The liquid will evaporate 2) Objects
ALTITUDE PHYSIOLOGY. Physiological Zones of the Atmosphere. Composition of the Air AIR ATTENDANTS COURSE. Sea Level Pressure
 AIR ATTENDANTS COURSE ALTITUDE PHYSIOLOGY Physical Divisions of the Atmosphere 1200 miles 600 miles EXOSPHERE Physiological Zones of the Atmosphere 50 miles IONOSPHERE SPACE EQUIVALENT ZONE: 50,000 feet
AIR ATTENDANTS COURSE ALTITUDE PHYSIOLOGY Physical Divisions of the Atmosphere 1200 miles 600 miles EXOSPHERE Physiological Zones of the Atmosphere 50 miles IONOSPHERE SPACE EQUIVALENT ZONE: 50,000 feet
Smoke inhalation 2/1/2013. Disclosures. Smoke Inhalation. Case Study
 Disclosures Smoke inhalation Craig Smollin MD Associate Medical Director, California Poison Control Center, SF Assistant Professor of Emergency Medicine University of California, San Francisco No financial
Disclosures Smoke inhalation Craig Smollin MD Associate Medical Director, California Poison Control Center, SF Assistant Professor of Emergency Medicine University of California, San Francisco No financial
Aerospace Physiology MARYLAND. Cardiopulmonary Physiology. Musculoskeletal Vestibular Neurological. Respiratory Cardiovascular U N I V E R S I T Y O F
 Cardiopulmonary Physiology Respiratory Cardiovascular Musculoskeletal Vestibular Neurological 2003 David L. Akin - All rights reserved http://spacecraft.ssl.umd.edu The Human Circulatory System Lung Measurements
Cardiopulmonary Physiology Respiratory Cardiovascular Musculoskeletal Vestibular Neurological 2003 David L. Akin - All rights reserved http://spacecraft.ssl.umd.edu The Human Circulatory System Lung Measurements
SPQ Module 9 Breathing at Altitude
 SPQ Module 9 Breathing at Altitude For most people traveling 1130 kilometers on foot over a frozen ice cap with no support would be daunting enough without facing the prospect of being short of breath
SPQ Module 9 Breathing at Altitude For most people traveling 1130 kilometers on foot over a frozen ice cap with no support would be daunting enough without facing the prospect of being short of breath
Office. Hypoxia. Or this. Or even this. Hypoxia E-1. COL Brian W. Smalley DO, MSPH, CPE
 Hypoxia Office COL Brian W. Smalley DO, MSPH, CPE Or this Or even this Hypoxia State of oxygen deficiency in the blood cells and tissues sufficient to cause impairment of function 4 Types Hypoxic Hypemic
Hypoxia Office COL Brian W. Smalley DO, MSPH, CPE Or this Or even this Hypoxia State of oxygen deficiency in the blood cells and tissues sufficient to cause impairment of function 4 Types Hypoxic Hypemic
Acute Mountain Sickness
 2012 Scottish Universities Medical Journal, Dundee Published online: Feb 2012 Vol 1 Issue 1: page 98-103 Gomersall T Acute Mountain Sickness Acute Mountain Sickness Tim Gomersall (2 nd Year MBChB) University
2012 Scottish Universities Medical Journal, Dundee Published online: Feb 2012 Vol 1 Issue 1: page 98-103 Gomersall T Acute Mountain Sickness Acute Mountain Sickness Tim Gomersall (2 nd Year MBChB) University
Medical Aspects of Diving in the Offshore Oil Industry
 Medical Aspects of Diving in the Offshore Oil Industry Dr Stephen Watt Retired Consultant in Respiratory and Hyperbaric Medicine Chairman, Diving Medical Advisory Committee What is diving? Diving = Commuting
Medical Aspects of Diving in the Offshore Oil Industry Dr Stephen Watt Retired Consultant in Respiratory and Hyperbaric Medicine Chairman, Diving Medical Advisory Committee What is diving? Diving = Commuting
Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation.
, Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation.") Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation. Paradoxical breathing Hyper-resonance on percussion:
Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation. Paradoxical breathing Hyper-resonance on percussion:
DECOMPRESSION PHYSIOLOGY and SUSCEPTIBILITY
 Chapter 13 DECOMPRESSION PHYSIOLOGY and SUSCEPTIBILITY Decompression Sickness (DCS) is an illness caused by the effects of gas coming out of solution to form bubbles in the body after diving. It is due
Chapter 13 DECOMPRESSION PHYSIOLOGY and SUSCEPTIBILITY Decompression Sickness (DCS) is an illness caused by the effects of gas coming out of solution to form bubbles in the body after diving. It is due
Hyperbarics 2 CEUs By: Michelle E. Duffelmeyer, MD. Co-author: Ellen Smithline, RN. Objectives
 Hyperbarics 2 CEUs By: Michelle E. Duffelmeyer, MD Co-author: Ellen Smithline, RN Objectives By the end of this lecture, the participant should be able to... 1. Describe the basic principles that explain
Hyperbarics 2 CEUs By: Michelle E. Duffelmeyer, MD Co-author: Ellen Smithline, RN Objectives By the end of this lecture, the participant should be able to... 1. Describe the basic principles that explain
PHYSIOLOGY. Let s look at the route in sequence, starting at the lungs where the blood releases CO2 and takes on oxygen at the pulmonary capillaries.
 PHYSIOLOGY Circulation: Blood circulates around your body to fuel the body with oxygen, the body uses the oxygen and changes it to carbon dioxide (CO2) the blood then carries this back to the lungs where
PHYSIOLOGY Circulation: Blood circulates around your body to fuel the body with oxygen, the body uses the oxygen and changes it to carbon dioxide (CO2) the blood then carries this back to the lungs where
Lecture Notes: EMT-P Environmental Keith Conover, M.D., FACEP /5/2013 Homeostasis A system that keeps things the same (roughly).
.") Lecture Notes: EMT-P Environmental Keith Conover, M.D., FACEP 1.0 11/5/2013 Homeostasis A system that keeps things the same (roughly). Think thermostat. Water Salt Temperature Hypothalamus Fever basal
Lecture Notes: EMT-P Environmental Keith Conover, M.D., FACEP 1.0 11/5/2013 Homeostasis A system that keeps things the same (roughly). Think thermostat. Water Salt Temperature Hypothalamus Fever basal
Hyperbaric Oxygen Therapy
 Hyperbaric Oxygen Therapy WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A.,
Hyperbaric Oxygen Therapy WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A.,
Doc #: 1000-AD Revision: - WORKING AT ALTITUDE AWARENESS POLICY. Author(s): Tammie Lavoie, Miranda Saucedo, John Dunlop
: Tammie Lavoie, Miranda Saucedo, John Dunlop") Doc #: 1000-AD-015-0020 Revision: - WORKING AT ALTITUDE AWARENESS POLICY Author(s): Tammie Lavoie, Miranda Saucedo, John Dunlop TABLE OF CONTENTS REVISION HISTORY... 3 1.0 INTRODUCTION... 4 2.0 SIGNS/SYMPTOMS
Doc #: 1000-AD-015-0020 Revision: - WORKING AT ALTITUDE AWARENESS POLICY Author(s): Tammie Lavoie, Miranda Saucedo, John Dunlop TABLE OF CONTENTS REVISION HISTORY... 3 1.0 INTRODUCTION... 4 2.0 SIGNS/SYMPTOMS
I look forward to seeing you in the coming month. If you have any questions or comments please feel free to contact me thru or by phone.
 Board of County Commissioners Pete Gerken President Tina Skeldon Wozniak Ben Konop Emergency Medical Services Dennis Cole Director Gary Orlow Manager TO: FROM: ALL LUCAS COUNTY PARAMEDICS Brent Parquette,
Board of County Commissioners Pete Gerken President Tina Skeldon Wozniak Ben Konop Emergency Medical Services Dennis Cole Director Gary Orlow Manager TO: FROM: ALL LUCAS COUNTY PARAMEDICS Brent Parquette,
Some Diving Physics and Physiology; Barotrauma. Robbert Hermanns Occupational Health Risk Management Services Ltd
 Some Diving Physics and Physiology; Barotrauma Robbert Hermanns Occupational Health Risk Management Services Ltd Oil & Gas UK (EBS) conference th 24 May 2017 Dr Robbert Hermanns MFOM Robbert.hermanns@ohrms.co.uk
Some Diving Physics and Physiology; Barotrauma Robbert Hermanns Occupational Health Risk Management Services Ltd Oil & Gas UK (EBS) conference th 24 May 2017 Dr Robbert Hermanns MFOM Robbert.hermanns@ohrms.co.uk
GUIDELINES FOR THE DIVER ** EXAMINATION
 GUIDELINES FOR THE DIVER ** EXAMINATION Dear Diver Enclosed please find the first draft of a recently compiled sample list of Diver ** theory questions. These guidelines are aimed at assisting two groups
GUIDELINES FOR THE DIVER ** EXAMINATION Dear Diver Enclosed please find the first draft of a recently compiled sample list of Diver ** theory questions. These guidelines are aimed at assisting two groups
A FISH FOR YOU! AOCOPM Midyear Meeting San Antonio, March 8-11, 2018 M-1 EDUCATIONAL OBJECTIVES. Boyle s Law GAS LAWS BOYLE S LAW
 EDUCATIONAL OBJECTIVES A FISH FOR YOU! HYPERBARIC MEDICINE REVIEW FOR THE CAQ EXAM MARY E. HANLEY, DO, UHM REVIEW MATERIAL THAT COMMONLY APPEARS ON CAQ EXAM REVIEW GAS LAWS AND THE BASIC MATH OF HYPERBARIC
EDUCATIONAL OBJECTIVES A FISH FOR YOU! HYPERBARIC MEDICINE REVIEW FOR THE CAQ EXAM MARY E. HANLEY, DO, UHM REVIEW MATERIAL THAT COMMONLY APPEARS ON CAQ EXAM REVIEW GAS LAWS AND THE BASIC MATH OF HYPERBARIC
A Dusky Hypoxic Woman. Craig Smollin MD Associate Medical Director California Poison Control Center - SF Div.
 A Dusky Hypoxic Woman Craig Smollin MD Associate Medical Director California Poison Control Center - SF Div. Blue man case #1 A 46 year-old male was sent to the emergency department for cyanosis. In the
A Dusky Hypoxic Woman Craig Smollin MD Associate Medical Director California Poison Control Center - SF Div. Blue man case #1 A 46 year-old male was sent to the emergency department for cyanosis. In the
Smoke inhalation. Disclosures. Smoke Inhalation
 Disclosures Smoke inhalation Craig Smollin MD Associate Medical Director, California Poison Control Center, SF Assistant Professor of Emergency Medicine University of California, San Francisco No financial
Disclosures Smoke inhalation Craig Smollin MD Associate Medical Director, California Poison Control Center, SF Assistant Professor of Emergency Medicine University of California, San Francisco No financial
ANNEX D: PHYSIOLOGICAL EPISODES
 1. The Navy s definition of a physiological episode (PE) is when a pilot experiences loss in performance related to insufficient oxygen, depressurization, or other factors during flight. For the purposes
1. The Navy s definition of a physiological episode (PE) is when a pilot experiences loss in performance related to insufficient oxygen, depressurization, or other factors during flight. For the purposes
Document is provided for sample purposes only. Content is not updated and should not be used for traveler counseling.
 Document is provided for sample purposes only. Content is not updated and should not be used for traveler counseling. Altitude Illness Medical Summary Introduction Altitude illness occurs when a traveler
Document is provided for sample purposes only. Content is not updated and should not be used for traveler counseling. Altitude Illness Medical Summary Introduction Altitude illness occurs when a traveler
Decompression sickness cases treated with recompression therapy between 1963 and 1998 in Turkey: Review of 179 cases
 Decompression sickness cases treated with recompression therapy between 1963 and 1998 in Turkey: Review of 179 cases Akin Savas Toklu 1, Maide Cimsit 1, Senol Yildiz 2, Gunalp Uzun 2, Sefika Korpinar 1,
Decompression sickness cases treated with recompression therapy between 1963 and 1998 in Turkey: Review of 179 cases Akin Savas Toklu 1, Maide Cimsit 1, Senol Yildiz 2, Gunalp Uzun 2, Sefika Korpinar 1,
Hyperbaric Oxygen Therapy. William Tettelbach, MD, FACP, CWS Intermountain Healthcare Salt Lake City, Utah
 Hyperbaric Oxygen Therapy William Tettelbach, MD, FACP, CWS Intermountain Healthcare Salt Lake City, Utah Hyperbaric Oxygen Indications Undersea and Hyperbaric Medical Society (www.uhms.org) FDA accepts
Hyperbaric Oxygen Therapy William Tettelbach, MD, FACP, CWS Intermountain Healthcare Salt Lake City, Utah Hyperbaric Oxygen Indications Undersea and Hyperbaric Medical Society (www.uhms.org) FDA accepts
Spring 1999 Hyperbaric Medicine Newsletter. Fellows Presentations. Saturation Diving
 Spring 1999 Hyperbaric Medicine Newsletter Fellows Presentations Saturation Diving The challenge of diving ever deeper is a goal that intrigues man. The technological advances of the last century have
Spring 1999 Hyperbaric Medicine Newsletter Fellows Presentations Saturation Diving The challenge of diving ever deeper is a goal that intrigues man. The technological advances of the last century have
Your Name. Detailed Course Outline and Learning Objectives. Welcome to American Red Cross Wilderness and Remote First Aid - WaRFA!
 Your Name Detailed Course Outline and Learning Objectives Note: This outline provides an overview of the course knowledge and skills to be taught in the American Red Cross Wilderness and Remote First Aid
Your Name Detailed Course Outline and Learning Objectives Note: This outline provides an overview of the course knowledge and skills to be taught in the American Red Cross Wilderness and Remote First Aid
MEDICAL DEPARTMENT PASSENGER INFORMATION PHYSICIAN INFORMATION
 MON-FRI 06:00-20:00 EST MEDICAL DEPARTMENT SAT-SUN 06:00-18 :00 EST Email : acmedical@aircanada.ca Fax 1-888-334-7717 (Toll-free from North America) Telephone 1-800-667-4732 (Toll-free from North America)
MON-FRI 06:00-20:00 EST MEDICAL DEPARTMENT SAT-SUN 06:00-18 :00 EST Email : acmedical@aircanada.ca Fax 1-888-334-7717 (Toll-free from North America) Telephone 1-800-667-4732 (Toll-free from North America)
ALFRED HYPERBARIC SERVICE. Service and Care. Information for Patients
 ALFRED HYPERBARIC SERVICE Service and Care Information for Patients ALFRED HEALTH Alfred Hyperbaric Service The Alfred Commercial Road Melbourne, VIC 3004 Phone (03) 9076 2269 Fax (03) 9076 3052 This booklet
ALFRED HYPERBARIC SERVICE Service and Care Information for Patients ALFRED HEALTH Alfred Hyperbaric Service The Alfred Commercial Road Melbourne, VIC 3004 Phone (03) 9076 2269 Fax (03) 9076 3052 This booklet
Environmental Injuries and the Athlete
 Environmental Injuries and the Athlete Presentation subtitle Heat Illness Hypothermia Frostbite Altitude Illness Month Day, Year Thomas Moran MD Northshore University Health System Clinician educator,
Environmental Injuries and the Athlete Presentation subtitle Heat Illness Hypothermia Frostbite Altitude Illness Month Day, Year Thomas Moran MD Northshore University Health System Clinician educator,
Home ( Articles ( Oxygen Toxicity and CCR/Rebreather Diving
 Home (https://www.diverite.com) Articles (https://www.diverite.com/category/articles/) Oxygen Toxicity and CCR/Rebreather Diving OXYGEN TOXICITY AND CCR/RE- BREATHER DIVING A couple of years ago I had
Home (https://www.diverite.com) Articles (https://www.diverite.com/category/articles/) Oxygen Toxicity and CCR/Rebreather Diving OXYGEN TOXICITY AND CCR/RE- BREATHER DIVING A couple of years ago I had
VIKING DIVING SERVICES, Inc Application for employment
 VIKING DIVING SERVICES, Inc Application for employment IRS W-4 Personal Information Nickname Present address City State Zip code Phone Cell Refereed by Place of Birth Date of Birth Email address Emergency
VIKING DIVING SERVICES, Inc Application for employment IRS W-4 Personal Information Nickname Present address City State Zip code Phone Cell Refereed by Place of Birth Date of Birth Email address Emergency
Respiratory Medicine. A-A Gradient & Alveolar Gas Equation Laboratory Diagnostics. Alveolar Gas Equation. See online here
 Respiratory Medicine A-A Gradient & Alveolar Gas Equation Laboratory Diagnostics See online here Alveolar gas equation helps to calculate the partial pressure of oxygen in alveoli and A-a gradient is the
Respiratory Medicine A-A Gradient & Alveolar Gas Equation Laboratory Diagnostics See online here Alveolar gas equation helps to calculate the partial pressure of oxygen in alveoli and A-a gradient is the
Diving Accident Management
 Diving Accident Management From Diving Medicine Online http://scuba-doc.com/ 3/8/2004 Diving Medicine Online 1 Introduction! It is desirable to have a standard approach to the initial management (i.e.
Diving Accident Management From Diving Medicine Online http://scuba-doc.com/ 3/8/2004 Diving Medicine Online 1 Introduction! It is desirable to have a standard approach to the initial management (i.e.
Rescue Swimmer Refresher Course. Practical First Aid Training/Mock Trauma LT 2.2
 Rescue Swimmer Refresher Course Practical First Aid Training/Mock Trauma LT 2.2 Enabling Objectives Respond to an emergency per current American Red Cross standards. Administer CPR per current American
Rescue Swimmer Refresher Course Practical First Aid Training/Mock Trauma LT 2.2 Enabling Objectives Respond to an emergency per current American Red Cross standards. Administer CPR per current American
USARIEM TECHNICAL NOTE 94-2 MEDICAL PROBLEMS IN HIGH MOUNTAIN ENVIRONMENTS. A Handbook for Medical Officers
 AD USARIEM TECHNICAL NOTE 94-2 MEDICAL PROBLEMS IN HIGH MOUNTAIN ENVIRONMENTS A Handbook for Medical Officers U S ARMY RESEARCH INSTITUTE OF ENVIRONMENTAL MEDICINE Natick, Massachusetts 01760-5007 February
AD USARIEM TECHNICAL NOTE 94-2 MEDICAL PROBLEMS IN HIGH MOUNTAIN ENVIRONMENTS A Handbook for Medical Officers U S ARMY RESEARCH INSTITUTE OF ENVIRONMENTAL MEDICINE Natick, Massachusetts 01760-5007 February
ELEDT S APR24 19 DECOMPRESSION SICKNESS AFFECTING THE TEMPOROMANDIBULAR JOINT. Author:
 r V COPY to DECOMPRESSION SICKNESS AFFECTING THE TEMPOROMANDIBULAR JOINT 0 N Author: Frederick W. Rudge, M.D. Major, USAF, MC, FS United States Air Force School of Aerospace Medicine Brooks Air Force Base,
r V COPY to DECOMPRESSION SICKNESS AFFECTING THE TEMPOROMANDIBULAR JOINT 0 N Author: Frederick W. Rudge, M.D. Major, USAF, MC, FS United States Air Force School of Aerospace Medicine Brooks Air Force Base,
Oxygen and Respiration
 THRESHOLDS OF OXYGEN REQUIREMENTS SUMMARY Up to 10,000 ft Air only 10,000-33,700 ft Oxygen/Air mixture 33,700-40,000 ft 100% Oxygen Above 40,000 ft 100% Oxygen under pressure HYPOXIC HYPOXIA The term for
THRESHOLDS OF OXYGEN REQUIREMENTS SUMMARY Up to 10,000 ft Air only 10,000-33,700 ft Oxygen/Air mixture 33,700-40,000 ft 100% Oxygen Above 40,000 ft 100% Oxygen under pressure HYPOXIC HYPOXIA The term for
Medical Section. Fax : (toll-free) or
 or") Departure Date: Medical Section Hours of Operation MON-FRI 06:00-20:00 EST SAT-SUN 06:00-18 :00 EST Email : acmedical@aircanada.ca Fax : 1 888 334-7717 (toll-free) or 514 205-7567 Telephone : 1 800 667-4732
Departure Date: Medical Section Hours of Operation MON-FRI 06:00-20:00 EST SAT-SUN 06:00-18 :00 EST Email : acmedical@aircanada.ca Fax : 1 888 334-7717 (toll-free) or 514 205-7567 Telephone : 1 800 667-4732
CONSENSUS STATEMENT OF THE UIAA MEDICAL COMMISSION VOL: 3
 THE INTERNATIONAL MOUNTAINEERING AND CLIMBING FEDERATION UNION INTERNATIONALE DES ASSOCIATIONS D ALPINISME Office: Monbijoustrasse 61 Postfach CH-3000 Berne 23 SWITZERLAND Tel.: +41 (0)31 3701828 Fax:
THE INTERNATIONAL MOUNTAINEERING AND CLIMBING FEDERATION UNION INTERNATIONALE DES ASSOCIATIONS D ALPINISME Office: Monbijoustrasse 61 Postfach CH-3000 Berne 23 SWITZERLAND Tel.: +41 (0)31 3701828 Fax:
Division of Marine Science & Technology Lockwood School of Diving and Underwater Technology Course Syllabus
 Division of Marine Science & Technology Lockwood School of Diving and Underwater Technology Course Syllabus COURSE TITLE COURSE NUMBER PREREQUISITES Recompression Chamber Operations EOC 2714C Nationally
Division of Marine Science & Technology Lockwood School of Diving and Underwater Technology Course Syllabus COURSE TITLE COURSE NUMBER PREREQUISITES Recompression Chamber Operations EOC 2714C Nationally
Lung Squeeze: Coughing your lungs out...or not!
 Lung Squeeze: Coughing your lungs out...or not! Introduction: Lung squeeze is a condition that is practically unique to Breath-Hold Diving. Scuba divers are not really aware of it and, sadly, most doctors
Lung Squeeze: Coughing your lungs out...or not! Introduction: Lung squeeze is a condition that is practically unique to Breath-Hold Diving. Scuba divers are not really aware of it and, sadly, most doctors
- How do the carotid bodies sense arterial blood gases? o The carotid bodies weigh 25mg, yet they have their own artery. This means that they have
 - How do the carotid bodies sense arterial blood gases? o The carotid bodies weigh 25mg, yet they have their own artery. This means that they have the highest blood flow of all organs, which makes them
- How do the carotid bodies sense arterial blood gases? o The carotid bodies weigh 25mg, yet they have their own artery. This means that they have the highest blood flow of all organs, which makes them
Cold and Heat Emergencies Video Cold & Heat Emergencies
 CHAPTER 20 Cold and Heat Emergencies Video Cold & Heat Emergencies Lesson Objectives 1. Describe the different types of cold and heat emergencies and what you can do to prevent them. 2. Explain factors
CHAPTER 20 Cold and Heat Emergencies Video Cold & Heat Emergencies Lesson Objectives 1. Describe the different types of cold and heat emergencies and what you can do to prevent them. 2. Explain factors
Working in low oxygen-controlled atmospheres. Risks and Prevention Measures Dr Michel Falcy, INRS FRANCE
 Working in low oxygen-controlled atmospheres Risks and Prevention Measures Dr Michel Falcy, INRS FRANCE Use of low O 2 -controlled atmospheres Nitrogenrefrigerated lorries Cryogenic facilities (sperm banks)
Working in low oxygen-controlled atmospheres Risks and Prevention Measures Dr Michel Falcy, INRS FRANCE Use of low O 2 -controlled atmospheres Nitrogenrefrigerated lorries Cryogenic facilities (sperm banks)
Occupational diver medical assessment questionnaire
 Occupational diver medical assessment questionnaire Occupational divers in New Zealand must undergo a full diving medical examination every five years, or as determined by the Diving Medical Consultant
Occupational diver medical assessment questionnaire Occupational divers in New Zealand must undergo a full diving medical examination every five years, or as determined by the Diving Medical Consultant
Adult, Child and Infant Exam
 CPR Pro for the Professional Rescuer Adult, Child and Infant Exam Instructions: Read each of the following questions carefully and then place an X over the correct answer on the separate answer sheet provided.
CPR Pro for the Professional Rescuer Adult, Child and Infant Exam Instructions: Read each of the following questions carefully and then place an X over the correct answer on the separate answer sheet provided.
Deborah Dewaay MD Division of General Internal Medicine and Geriatrics Hospital Medicine Acknowledgment: Antine Stenbit MD
 Deborah Dewaay MD Division of General Internal Medicine and Geriatrics Hospital Medicine 2013 Acknowledgment: Antine Stenbit MD Objectives Knowledge: Understand the difference between hypoxia and hypoxemia
Deborah Dewaay MD Division of General Internal Medicine and Geriatrics Hospital Medicine 2013 Acknowledgment: Antine Stenbit MD Objectives Knowledge: Understand the difference between hypoxia and hypoxemia
ENT & diving pathology: IE Decompression Sickness vs IE Barotrauma
 ENT & diving pathology: IE Decompression Sickness vs IE Barotrauma Dr Peter Germonpré Centre for Hyperbaric Oxygen Therapy Military Hospital Brussels peter.germonpre@mil.be Elke reproductie, geheel of
ENT & diving pathology: IE Decompression Sickness vs IE Barotrauma Dr Peter Germonpré Centre for Hyperbaric Oxygen Therapy Military Hospital Brussels peter.germonpre@mil.be Elke reproductie, geheel of
27 COLD & HYPOTHERMIA
 Chapter 27 COLD & HYPOTHERMIA A diver is usually immersed in water which is considerably colder than the normal body temperature of 37 ο C. Unfortunately, water is particularly efficient at removing body
Chapter 27 COLD & HYPOTHERMIA A diver is usually immersed in water which is considerably colder than the normal body temperature of 37 ο C. Unfortunately, water is particularly efficient at removing body
Patent Foramen Ovale and Fitness
 Guidelines for Patent Foramen Ovale and Fitness Proceedings Summary DAN/UHMS PFO and Fitness to Dive Workshop Introduction Prior to birth, oxygenated blood flows from the mother through the placenta to
Guidelines for Patent Foramen Ovale and Fitness Proceedings Summary DAN/UHMS PFO and Fitness to Dive Workshop Introduction Prior to birth, oxygenated blood flows from the mother through the placenta to
Physiology of Flight
 Physiology of Flight Physiology of Flight Physiology of flight: how the human body functions during flight Overview 1. Physiological Divisions of the Atmosphere 2. Hypoxia and Hyperventilation 3. Trapped
Physiology of Flight Physiology of Flight Physiology of flight: how the human body functions during flight Overview 1. Physiological Divisions of the Atmosphere 2. Hypoxia and Hyperventilation 3. Trapped
Outline What is it and what to expect Pilot physiology Oxygen equipment per FAA Wave windows Relevant FAR s NCSA Rules
 Northern California Soaring Association 2010 Safety Seminar High Altitude Wave Flight Considerations by Mike Voie, CFIG Outline What is it and what to expect Pilot physiology Oxygen equipment per FAA Wave
Northern California Soaring Association 2010 Safety Seminar High Altitude Wave Flight Considerations by Mike Voie, CFIG Outline What is it and what to expect Pilot physiology Oxygen equipment per FAA Wave
PHTY 300 Wk 1 Lectures
 PHTY 300 Wk 1 Lectures Arterial Blood Gas Components The test provides information on - Acid base balance - Oxygenation - Hemoglobin levels - Electrolyte blood glucose, lactate, renal function When initially
PHTY 300 Wk 1 Lectures Arterial Blood Gas Components The test provides information on - Acid base balance - Oxygenation - Hemoglobin levels - Electrolyte blood glucose, lactate, renal function When initially
Hyperbaric Oxygen Therapy Patient Information
 Hyperbaric Oxygen Therapy Patient Information One of only two in Wichita, Kansas, our hyperbaric oxygen chamber is truly unique. Hyperbaric therapy was originally used to treat deep sea divers who were
Hyperbaric Oxygen Therapy Patient Information One of only two in Wichita, Kansas, our hyperbaric oxygen chamber is truly unique. Hyperbaric therapy was originally used to treat deep sea divers who were
Diving History N.C. State University Diving Safety Program Application for Scientific Diving Authorization Section 1. Applicant Information
 N.C. State University Diving Safety Program Application for Scientific Diving Authorization Section 1. Applicant Information Date: Applicant Name: Date of Birth: Social Security No.: Sex: N.C. State Faculty:
N.C. State University Diving Safety Program Application for Scientific Diving Authorization Section 1. Applicant Information Date: Applicant Name: Date of Birth: Social Security No.: Sex: N.C. State Faculty:
Medical Issues in Aviation
 Medical Issues in Aviation Passenger Fitness to Fly Lima, Peru, April 2009 Claude Thibeault MD Medical Advisor Lima 2009 1 Passenger Fitness to Fly Plan - Review real cases based on altitude physiology
Medical Issues in Aviation Passenger Fitness to Fly Lima, Peru, April 2009 Claude Thibeault MD Medical Advisor Lima 2009 1 Passenger Fitness to Fly Plan - Review real cases based on altitude physiology
First Aid - immediate care that is given to the victim of an injury or illness until experts can take over - Oftentimes, it s the difference between
 First Aid First Aid - immediate care that is given to the victim of an injury or illness until experts can take over - Oftentimes, it s the difference between life and death or recovery vs permanent disability
First Aid First Aid - immediate care that is given to the victim of an injury or illness until experts can take over - Oftentimes, it s the difference between life and death or recovery vs permanent disability
CHAPTER 19 'LYLQJ'LVRUGHUV1RW5HTXLULQJ 5HFRPSUHVVLRQ7KHUDS\
 CHAPTER 19 'LYLQJ'LVRUGHUV1RW5HTXLULQJ 5HFRPSUHVVLRQ7KHUDS\ 19-1 INTRODUCTION 19-1.1 Purpose. This chapter covers diagnosis and treatment of diving disorders for which recompression therapy usually is
CHAPTER 19 'LYLQJ'LVRUGHUV1RW5HTXLULQJ 5HFRPSUHVVLRQ7KHUDS\ 19-1 INTRODUCTION 19-1.1 Purpose. This chapter covers diagnosis and treatment of diving disorders for which recompression therapy usually is
Working safely under pressure: Field experience in occupational medicine
 Working safely under pressure: Field experience in occupational medicine Dr. med. Claudia Pletscher Suva, Department of Occupational Medicine Head of Preventative Occupational Medicine Sector Agenda Introduction
Working safely under pressure: Field experience in occupational medicine Dr. med. Claudia Pletscher Suva, Department of Occupational Medicine Head of Preventative Occupational Medicine Sector Agenda Introduction
Medical declaration for divers
 Medical declaration for divers Participant details Name Birth date Age Male/ Female Address City State/Province/Region Country Zip/Postal code Postal Address (if different to home address) City State/Province/Region
Medical declaration for divers Participant details Name Birth date Age Male/ Female Address City State/Province/Region Country Zip/Postal code Postal Address (if different to home address) City State/Province/Region
To develop understanding of mental and physical standards required for operating an aircraft
 Aeromedical Factors Objective To develop understanding of mental and physical standards required for operating an aircraft Outline Obtaining a medical certificate Causes, symptoms, effects, and corrective
Aeromedical Factors Objective To develop understanding of mental and physical standards required for operating an aircraft Outline Obtaining a medical certificate Causes, symptoms, effects, and corrective
SECOND EUROPEAN CONSENSUS CONFERENCE ON HYPERBARIC MEDICINE THE TREATMENT OF DECOMPRESSION ACCIDENTS IN RECREATIONAL DIVING
 SECOND EUROPEAN CONSENSUS CONFERENCE ON HYPERBARIC MEDICINE THE TREATMENT OF DECOMPRESSION ACCIDENTS IN RECREATIONAL DIVING MARSEILLE, May 8-10, 1996 RECOMMENDATIONS OF THE JURY* QUESTION 1 : Is there
SECOND EUROPEAN CONSENSUS CONFERENCE ON HYPERBARIC MEDICINE THE TREATMENT OF DECOMPRESSION ACCIDENTS IN RECREATIONAL DIVING MARSEILLE, May 8-10, 1996 RECOMMENDATIONS OF THE JURY* QUESTION 1 : Is there
GENETIC INFLUENCE ON FACTORS OF OXYGEN TRANSPORT
 GENETIC INFLUENCE ON FACTORS OF OXYGEN TRANSPORT Claudio Marconi IBFM-Sect. of Muscle Physiology and Proteome National Research Council Milano, Italy 100 90 80 % s.l. VO 2 max. 70 60 50 40 30 20 10 0 2
GENETIC INFLUENCE ON FACTORS OF OXYGEN TRANSPORT Claudio Marconi IBFM-Sect. of Muscle Physiology and Proteome National Research Council Milano, Italy 100 90 80 % s.l. VO 2 max. 70 60 50 40 30 20 10 0 2
Decompression illness, or DCI, is a term used to describe illness that results
 Decompression Illness: By Dr. Ed Thalmann DAN America, 2004. Decompression illness, or DCI, is a term used to describe illness that results from a reduction in the ambient pressure surrounding a body.
Decompression Illness: By Dr. Ed Thalmann DAN America, 2004. Decompression illness, or DCI, is a term used to describe illness that results from a reduction in the ambient pressure surrounding a body.
Aerospace Physiology. Lecture #11 Oct. 7, 2014 Cardiopulmonary physiology. Musculoskeletal Vestibular Neurological Environmental Effects MARYLAND
 Lecture #11 Oct. 7, 2014 Cardiopulmonary physiology Respiratory Cardiovascular Musculoskeletal Vestibular Neurological Environmental Effects 1 2014 David L. Akin - All rights reserved http://spacecraft.ssl.umd.edu
Lecture #11 Oct. 7, 2014 Cardiopulmonary physiology Respiratory Cardiovascular Musculoskeletal Vestibular Neurological Environmental Effects 1 2014 David L. Akin - All rights reserved http://spacecraft.ssl.umd.edu