David A. Connett, DO, FACOFP, dist
|
|
|
- Curtis Dorsey
- 5 years ago
- Views:
Transcription
1 David A. Connett, DO, FACOFP, dist
2 Disclosures Nothing to disclose including pharmaceuticals
3 High Altitude Syndromes Acute Mountain Sickness (AMS) High Altitude Cerebral Edema (HACE) High Altitude Pulmonary Edema (HAPE) Decompression Sickness (DCS)
4
5 High Altitude High Altitude-5,000 feet to 11,500 feet ( m) Highest U.S. ski resorts Minor impairment of arterial oxygen transport arterialsao2> 90% AMS common with rapid ascent above 8000 feet Very High Altitude-11,500 feet to 18,000 feet ( m) High peaks in the lower 48, Europe Maximum arterial SaO2 < 90%, PAO2<60 torr Most common range for serious altitude sickness Extreme Altitude-over 18,000 feet (above 5500 m) Denali, Himalaya, Karakoram, Andes Marked hypoxemia and hypercapnia

6 Oxygen Levels at Altitude
7
8 Environment at High Altitude Barometric pressure falls with increasing altitude in logarithmic fashion Partial pressure of oxygen decreases resulting in hypoxia Altitude changes with distance from equator, hypoxia worse at the poles. Pressure is lower in winter than in summer. Temperature decreases with altitude 1000 feet for every 3.56 F Ultraviolet light increases by 4% every thousand feet
9
10 Pathophysiology Acute Mountain Sickness
11 Hypoxic Ventilatory Response (HVR)
12 Pathophysiology Acute Mountain Sickness
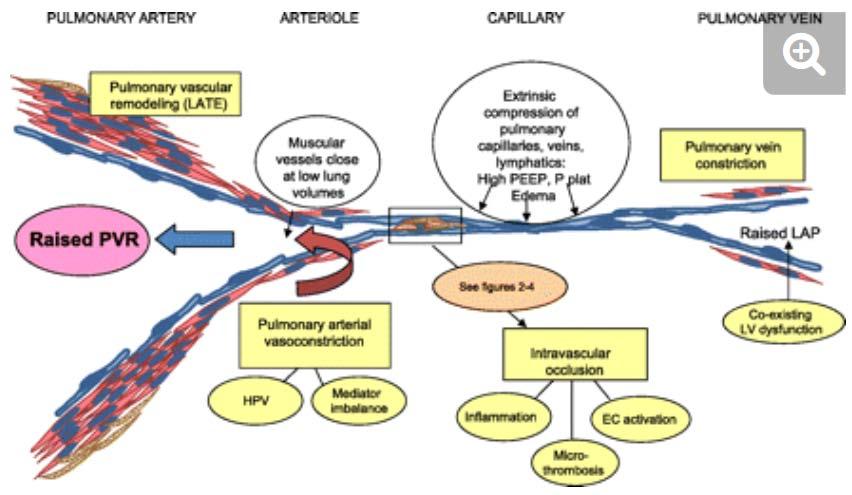
13 Pathophysiology of HAPE
14 Pathophysiology of HAPE Components of endothelial activation/dysfunction in acute lung injury (ALI). This schematic cartoon illustrates the components of endothelial activation including 1) Endothelial cell-leukocyte interactions, 2) Endothelial cell-platelet-neutrophil interactions, and 3) Structural changes between endothelial cells. RBC, red blood cell; MLCK, myosin light chain kinases; PASMC, pulmonary artery smooth muscle cell.
15
16 Pathophysiology of HAPE
17
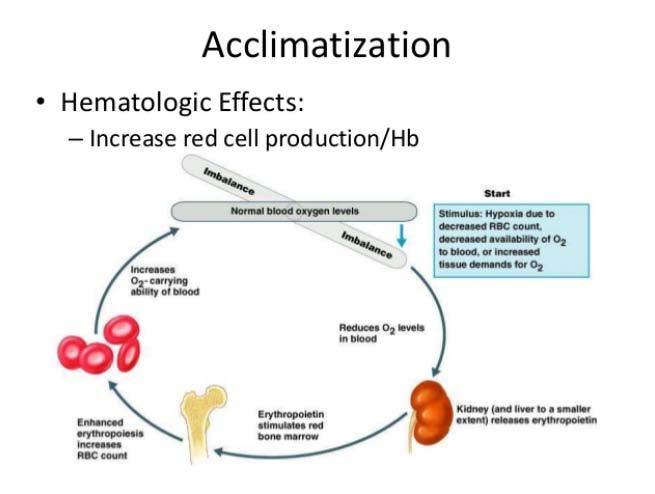
18 Factors Increased by Acclimatization Acute Ventilation Heart rate Cerebral blood flow Diuresis increased hematocrit Chronic Increase in pulmonary ventilation Increase and diffusing capacity in the lung Red blood cell count due to erythropoietin Metabolism (tissue changes over years) Increase in the number of mitochondria Augmentation of the cytochrome oxidase system
19
20 Acclimatization to High Altitude Rapid ascent and exposure to the altitude at the summit of Mount Everest 29,028 feet results in loss of consciousness in a few minutes and death shortly thereafter. Acclimatization occurs over time Ability to acclimatize varies from individuals Just a few days at sea level may make one susceptible to AMS or HAPE
21 Other Aids to Acclimatization Climb high. Sleep low. High carbohydrate diet Mild exercise-avoid exertion Avoid alcohol and sleeping medications
22
 Fatigue or weakness Dizziness or lightheadedness Difficulty")
23 Lake Louis Consensus definitions of High Altitude Acute Mountain Sickness In the setting of a recent gain in altitude, there is precedence of headache and at least one of the following: Gastrointestinal (anorexia, nausea or vomiting) Fatigue or weakness Dizziness or lightheadedness Difficulty sleeping
24 Acute Mountain Sickness Rapid ascent to 8200 feet from altitudes below 5000 feet for unacclimatized Headache Throbbing, by temporal or occipital worse at night Fatigue Dizziness/lightheadedness Anorexia and nausea Difficulty sleeping
25 Mild Acute Mountain Sickness Mild Headache Insomnia Shortness of Breath while Exercising May continue climbing More time for acclimatization
26 Moderate Acute Mountain Sickness Headache may be severe Some lassitude Weakness Loss of appetite Nausea Beginning to lose coordination - ataxia Begin to descend
27 Acute Mountain Sickness Differential Diagnosis Viral illness Hangover Exhaustion Dehydration Hypothermia Sedatives/hypnotic medications Carbon monoxide
28 Acute Mountain Sickness Usually self-limited If untreated may persist for weeks May precede HACE or HAPE Responds well to treatment
29 Lake Louis Consensus definitions of High Altitude High Altitude Pulmonary Edema (HAPE) In the presence of a recent gain in altitude, the presence of the following: Two of the following symptoms: Dyspnea at rest Cough Chest tightness or congestion At least two of the following signs: Crackles or wheezing and at least one lung field Central cyanosis Tachypnea Tachycardia
30 High Altitude Pulmonary Edema The most common cause of death from high-altitude illness. Most often after second night at new altitude Apparent abrupt onset May occur in the absence of Acute Mountain Sickness
31 HAPE Symptoms and Signs Early symptoms: fatigue, weakness, dyspnea on exertion, dry cough Progression to tachycardia, tachypnea, and orthopnea and dyspnea at rest marked shortness of breath even at rest Pink or blood-tinged sputum is a very late finding Crackles usually start in right axilla May also have headache, lassitude, reduced urine output, peripheral edema and ataxia.

32
33 Distribution of Symptoms and signs in 154 Trekkers Nepal with AMS Severity Percent Symptoms Mild 65 Headache, anorexia, nausea and malaise Moderate 30 Unrelieved headache, vomiting, reduced urine output Severe 5 Altered consciousness, ataxia, rales, cyanosis, dyspepsia at rest, possible papilledema
34 Incidents of Altitude Illness in Various Groups Study Group Number at Risk per Year Sleeping Altitude (feet) Maximum Altitude Reached (feet) Average Rate of Assent (days low altitude) Percent with AMS Percent with HAPE and/or HACE Western State Visitors 30 million 6500 ft ft. >9800 ft. 11,500 ft Mount Everest ,000 ft. 1-2 (fly in) 10-13(walk) Mount Denali ,321 feet Mount Rainier ,409 ft Indian soldiers Unknown 18,000 ft
35
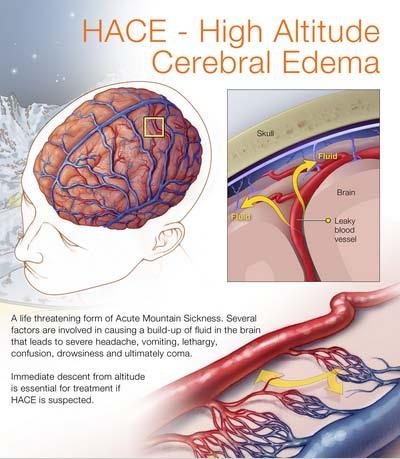
36 Lake Louis Consensus definitions of High Altitude High Altitude Cerebral Edema (HACE) Can be considered end-stage or severe acute Mountain sickness. In the setting of a recent gaining altitude there is either: The presence of a change in mental status and/or ataxia in a person with Acute Mountain Sickness Or the presence of both mental status changes and ataxia any person without Acute Mountain Sickness
37 High Altitude Cerebral Edema Progression of cerebral signs and symptoms of Acute Mountain Sickness Headache, vomiting Truncal ataxia (other focal neurologic deficits may also occur) Severe lassitude Altered consciousness or coma Weakness or paralysis on one side of the body Amnesia or hallucinations Especially common with High Altitude Pulmonary Edema - Shortness of breath, dry cough
38

39
 Irrationality Hallucinations Visual disturbances Focal neurological deficits Abnormal reflexes")
40 High Altitude Cerebral Edema Early Symptoms Headache Anorexia Nausea Emesis Photophobia Fatigue Irritability Decrease socialization Late Symptoms Ataxia (appendicular to truncal) Irrationality Hallucinations Visual disturbances Focal neurological deficits Abnormal reflexes
41 Other Altitude Related Disorders High-altitude retinopathy maintain good fluid intake to reduce hemoconcentration, spontaneously resolves Peripheral edema treat with a diuretic in the absence of AMS, HACE or HAPE; condition spontaneously resolves on descent Venous stasis and thrombotic complications stay active keep well hydrated and descend if needed Altitude pharyngitis and bronchitis suck on hard candy, brie through a facemask and drink plenty of fluids Ultraviolet keratitis ( snow blindness) remove contact lenses, patch affected eye, use oral analgesics to decrease pain; prevented by wearing sunglasses
42
43 Acute Mountain Sickness Management The Golden Rules # 1 AMS symptoms at altitude are AMS until proven otherwise # 2 Don t ascend further if you have symptoms # 3 Descend if very ill or not improving. Descend immediately for ataxia or decreased consciousness #4 Don t let anyone with AMS descend alone
44 Prevention Acute Mountain Sickness Prevention Acetazolamide (Diamox) 125 mg twice a day (or 500 mg slow release daily) Start 12 hours before assent Continue first day at altitude Sleep Acetazolamide (Diamox) mg at dinner time
45 Treating Acute Mountain Sickness The mainstay of treatment of AMS is rest, fluids, and mild analgesics: acetaminophen (Tylenol), aspirin, or ibuprofen. These medications will not cover up worsening symptoms. The natural progression for AMS is to get better, and often simply resting at the altitude at which you became ill is adequate treatment. Improvement usually occurs in one or two days, but may take as long as three or four days. Dehydration is a common cause of headache at altitude. Drink one liter of fluid, and take acetaminophen or aspirin. If the headache resolves quickly and totally (and you have no other symptoms of AMS) it is very unlikely to have been due to AMS. Descent is also an option, and recovery will be quite rapid.
46 Treatment Mild Acute Mountain Sickness Stop ascent, rest, acclimatize at same altitude Acetazolamide, 125 to 150 mg twice a day, to speed acclimatization Symptomatic treatment as necessary with analgesics and anti-medics or Descend 1500 feet or more
47 Treatment Moderate Acute Mountain Sickness Low-flow oxygen, if available Acetazolamide, 125 two 250 mg twice a day with or without Dexamethasone, 4 mg PO,IM, IV q 6hr Hyperbaric therapy or Immediate descent
 above ambient pressure 14,000 feet simulates 8000 feet CO2")
48 Instant Descent Inside a Bag 0.14 atmosphere (102 torr) above ambient pressure 14,000 feet simulates 8000 feet CO2 buildup minimal if used properly (and maybe helpful)
49 Treatment HAPE Minimize exertion and keep warm Oxygen, 4 to 6 L/min until improving it, then 2 to 4 L/min Dexamethasone, 4 mg PO,IM, IV q 6hr
50 HAPE Prevention Graded ascent Nifedipine for HAPE susceptibles 20 mg orally every eight hours or 30 mg every 12 hours-starting 24 hours before arrival and continuing for three days
51 HAPE Prevention Tadalafil and Sildenafil Phosphodiesterase-5 (PDE-5) inhibitors that augment the pulmonary vasodilatory effects of nitric oxide by blocking the degradation of cyclic guanosine monophosphate (cgmp), the intracellular mediator of nitric oxide. Nitric oxide is a potent pulmonary vasodilator and reduces hypoxic pulmonary vasoconstriction (HPV) and pulmonary hypertension in HAPE. Both Tadalafil and sildenafil have been shown to be effective as prophylaxis for HAPE, but neither has been studied as treatment. Nevertheless, based upon their mechanism of action, both Tadalafil and sildenafil may be effective adjunct treatments for established HAPE when neither oxygen nor descent is available options. These drugs may have advantages over nifedipine because they lower PA pressure with less risk of lowering systemic blood pressure. The appropriate dose for treatment is unknown but might be similar to that used for prophylaxis (Tadalafil 10 mg by mouth every 12 hours; sildenafil 50 mg by mouth every eight hours).
52 HAPE Prevention Dexamethasone 8 mg every 12 hours (also helps to prevent Acute Mountain Sickness) Tadalafil 10 mg every 12 hours (no benefit for Acute Mountain Sickness) Salmeterol 125 µg every 12 hours (some benefit for Acute Mountain Sickness) All regimes start 24 hours prior to assent and continue at altitude
53 Other Drugs to Prevent Acute Mountain Sickness Dexamethasone Indicated with contraindication to Acetazolamide Also used in conjunction with acetazolamide for rapid ascent above 10,000 feet (rescue) Dosage 4 mg every six hours
54 Treatment HACE Immediate descent or evacuation Oxygen, 2 to 4 L/min Dexamethasone, 4 mg PO,IM, IV q 6hr Hyperbaric therapy
55
56 Indications for Acetazolamide Rapid ascent to altitudes over 10,000 feet Past history of recurrent Acute Mountain Sickness Treatment of Acute Mountain Sickness Periodic breathing or poor sleep
57
58 High Altitude Medical Contraindications/Cautions Contraindications Uncompensated left heart failure Pulmonary hypertension Sickle cell anemia Moderate-severe COPD Seizure disorders Cautions History of left heart failure Cardiac arrhythmias Cerebral vascular disease Sleep apnea Sickle Trait

59
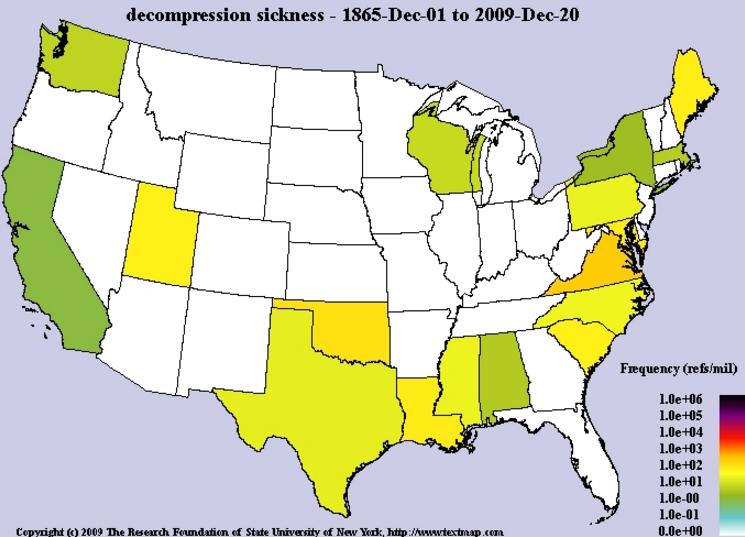
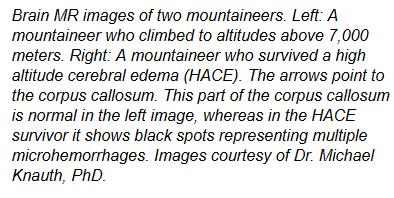
60 Distribution of DCS

61 Decompression Sickness Decompression sickness (DCS) results from the formation of nitrogen bubbles in the tissues or circulation as a result of inadequate elimination of nitrogen after a dive. The formation of nitrogen bubbles may occur following a dive and ascending to high altitudes in a short period of time to include a pressurized commercial aircraft. Bubbles that form are trapped in the joints called the bends. Bubbles that are formed in circulation may become trapped in the brain or spinal cord resulting in serious neurological compromise or death. DCS may also occur in very high altitudes with aircraft or spacecraft without a dive to precipitate the response.

62 Decompression Sickness Limb Bends Central Nervous System (CNS) DCS Cerebral Decompression Sickness Pulmonary DCS Skin Bends Inner Ear Decompression Sickness


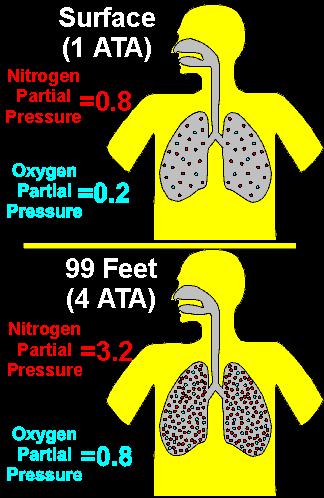
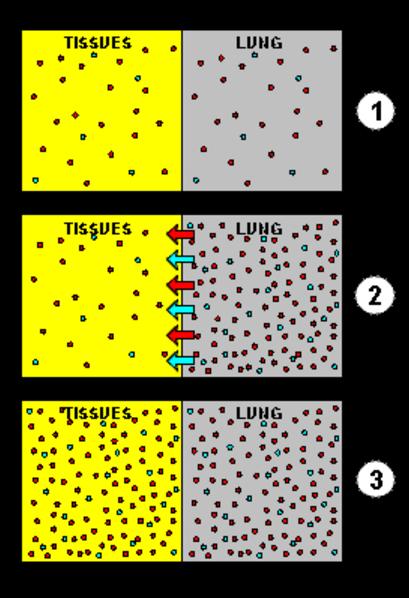
63 Gas Laws - Dalton and Henry Dalton s Law - in a mixture of nonreacting gases, the total pressure exerted is equal to the sum of the partial pressures of the individual gases. Henry s Law - the amount of dissolved gas is proportional to its partial pressure in the gas phase. In diving more gas is dissolved in solution when at pressure.
64 Decompression Sickness

65 Boyles Law - Air Embolism vs Bends

66 Air Embolism Gas (air) entry into the circulation from ruptured pulmonary veins or patent foramen ovale Air bubbles travel in the arterial blood supply and the tissues Air bubbles become lodged in tissues blocking blood flow

67 Air Embolism Occurs within 2-3 minutes Cardiac arrest or arrhythmias Neurological focal paralysis, sensory disturbance, seizures, altered mental status

68 Physiological Atmospheric Divisions
69 Pathophysiology of Bubbles in DCS

70 Dive Table Pushing Your Tables
71 Altitude Decompression Risk Assessment

72 Altitude Decompression Risk Assessment
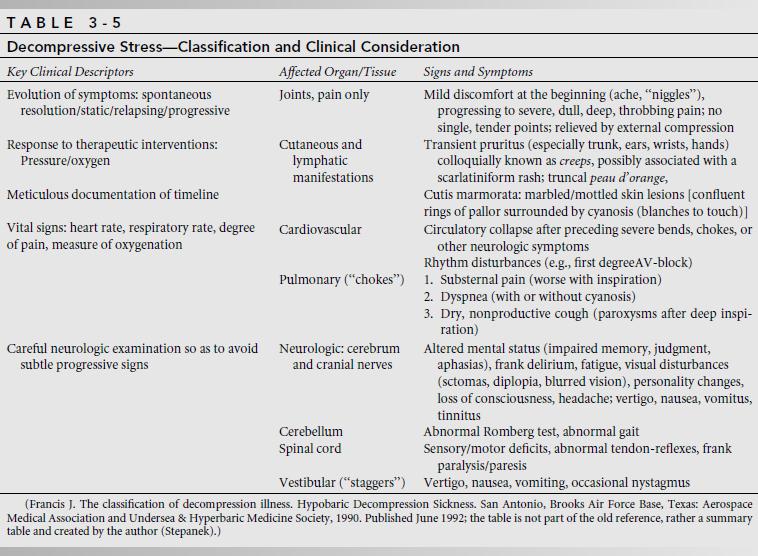
73 Classification DCS
74 Principle Factors for DCS Two principal factors control the risk of a diver suffering DCS: 1.The rate and duration of gas absorption under pressure the deeper or longer the dive the more gas is absorbed into body tissue in higher concentrations than normal (Henry's Law); 2.The rate and duration of outgassing on depressurization the faster the ascent and the shorter the interval between dives the less time there is for absorbed gas to be offloaded safely through the lungs, causing these gases to come out of solution and form "micro bubbles" in the blood. Even when the change in pressure causes no immediate symptoms, rapid pressure change can cause permanent bone injury called dysbaric osteonecrosis (DON). DON can develop from a single exposure to rapid decompression. Risks at Altitude 1. Can happen over 18k ft, especially repeated ascents 2. Is a substantial risk over 30k ft. 3. Is a much greater risk after diving. 4. Risk is related to altitude and rate of ascent. 5. In gliders, is a risk in wave flights. 6. In pressurized aircraft, is likely in depressurization accidents. 7. Can results in permanent injury. 1. Must seek a bariatric physician ASAP % oxygen rebreathing

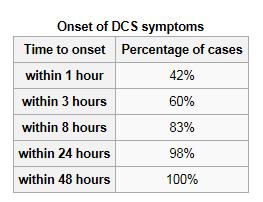
75 Symptoms Frequency and Onset


76 Skin Bends

77 Spinal Cord Bends Infarction of Cord


78 Bends Prevention
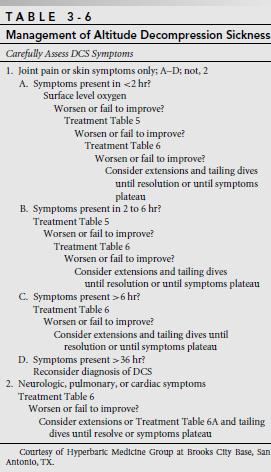


79 DCS Management

80 DCS Management US Navy Table 6

81 DCS Management

82 Important Safety Tip
83 Questions
Espilat Mountaineering Club
 In the name of God Espilat Mountaineering Club May 2013 MEDICAL PROBLEMS IN HIGH MOUNTAIN ENVIRONMENTS Arya Hamedanchi MD, MPH Level one International Anthropometrist International Certificate of Ski Medicine
In the name of God Espilat Mountaineering Club May 2013 MEDICAL PROBLEMS IN HIGH MOUNTAIN ENVIRONMENTS Arya Hamedanchi MD, MPH Level one International Anthropometrist International Certificate of Ski Medicine
High Altitude Pulmonary Edema (HAPE)
") High Altitude Pulmonary Edema (HAPE) HAPE is a fluid build-up in the lungs. Cases seen at altitudes as low as 8,000 ft. (e.g., Colorado ski resorts) HAPE: Some Basics Can occur in people with no other
High Altitude Pulmonary Edema (HAPE) HAPE is a fluid build-up in the lungs. Cases seen at altitudes as low as 8,000 ft. (e.g., Colorado ski resorts) HAPE: Some Basics Can occur in people with no other
Acute Mountain Sickness
 Innere Medizin VII / Sportmedizin Acute Mountain Sickness Peter Bärtsch www.klinikum.uni-heidelberg.de/sportmedizin AMS: Clinical Picture Symptoms: - Headache - Loss of appetite, nausea, vomiting - Dizziness
Innere Medizin VII / Sportmedizin Acute Mountain Sickness Peter Bärtsch www.klinikum.uni-heidelberg.de/sportmedizin AMS: Clinical Picture Symptoms: - Headache - Loss of appetite, nausea, vomiting - Dizziness
SCUBA - self contained underwater breathing apparatus. 5 million sport scuba divers in U.S. 250, ,000 new certifications annually in U.S.
 SCUBA - self contained underwater breathing apparatus 5 million sport scuba divers in US 250,000-400,000 new certifications annually in US Diving occurs in oceans, freshwater lakes, rivers and quarries
SCUBA - self contained underwater breathing apparatus 5 million sport scuba divers in US 250,000-400,000 new certifications annually in US Diving occurs in oceans, freshwater lakes, rivers and quarries
Environmental Injuries: The Winter Athlete. Thomas Moran, MD Primary Care Sports Medicine Fellow University of Chicago - NorthShore
 Environmental Injuries: The Winter Athlete Thomas Moran, MD Primary Care Sports Medicine Fellow University of Chicago - NorthShore Introduction Chicago Marathon >41,000 runners 2006 (36 start,48 high with
Environmental Injuries: The Winter Athlete Thomas Moran, MD Primary Care Sports Medicine Fellow University of Chicago - NorthShore Introduction Chicago Marathon >41,000 runners 2006 (36 start,48 high with
the ACUTE MOUNTAIN SICKNESS manual
 the ACUTE MOUNTAIN SICKNESS manual AMS (Acute Mountain Sickness) at high altitude is common. It is your body s way of telling you that it is not able to adapt to the lesser oxygen it is getting. Depending
the ACUTE MOUNTAIN SICKNESS manual AMS (Acute Mountain Sickness) at high altitude is common. It is your body s way of telling you that it is not able to adapt to the lesser oxygen it is getting. Depending
1 out of every 5,555 of drivers dies in car accidents 1 out of every 7692 pregnant women die from complications 1 out of every 116,666 skydives ended
 1 out of every 5,555 of drivers dies in car accidents 1 out of every 7692 pregnant women die from complications 1 out of every 116,666 skydives ended in a fatality in 2000 1 out of every 126,626 marathon
1 out of every 5,555 of drivers dies in car accidents 1 out of every 7692 pregnant women die from complications 1 out of every 116,666 skydives ended in a fatality in 2000 1 out of every 126,626 marathon
Outdoor Action Guide to High Altitude: Acclimatization and Illnesses
 Outdoor Action Guide to High Altitude: Acclimatization and Illnesses Last Page update 07/07/1999 by Rick Curtis, Director, Outdoor Action Program Navigation Back to the AEE Wilderness Safety Page OA Guide
Outdoor Action Guide to High Altitude: Acclimatization and Illnesses Last Page update 07/07/1999 by Rick Curtis, Director, Outdoor Action Program Navigation Back to the AEE Wilderness Safety Page OA Guide
Civil Air Patrol Auxiliary of the United States Air Force
 Mountain Flying Qualification Course Civil Air Patrol Auxiliary of the United States Air Force Physiological Effects of Altitude Physiological Effects of Altitude OXYGEN DEPRIVATION (HYPOXIA) SINUS PRESSURE
Mountain Flying Qualification Course Civil Air Patrol Auxiliary of the United States Air Force Physiological Effects of Altitude Physiological Effects of Altitude OXYGEN DEPRIVATION (HYPOXIA) SINUS PRESSURE
Decompression Sickness
 Decompression Sickness Kun-Lun Huang National Defense Medical Center Undersea and Hyperbaric Medical Institute Tri-Service General Hospital Department of Undersea and Hyperbaric Medicine Hazard Diving
Decompression Sickness Kun-Lun Huang National Defense Medical Center Undersea and Hyperbaric Medical Institute Tri-Service General Hospital Department of Undersea and Hyperbaric Medicine Hazard Diving
Is Your Traveler Going to High Altitude?
 Is Your Traveler Going to High Altitude? Dr. Peter Hackett First came to Nepal in 1974 Worked 3 seasons at Himalayan Rescue Association aid post Did an altitude illness survey that was published in The
Is Your Traveler Going to High Altitude? Dr. Peter Hackett First came to Nepal in 1974 Worked 3 seasons at Himalayan Rescue Association aid post Did an altitude illness survey that was published in The
DEFENCE INSTRUCTIONS AND NOTICES (Not to be communicated to anyone outside HM Service without authority)
") Title: Audience: Applies: Expires: Reference: DEFENCE INSTRUCTIONS AND NOTICES (Not to be communicated to anyone outside HM Service without authority) Guidelines for the Conduct of Adventurous Training
Title: Audience: Applies: Expires: Reference: DEFENCE INSTRUCTIONS AND NOTICES (Not to be communicated to anyone outside HM Service without authority) Guidelines for the Conduct of Adventurous Training
High Altitude Medical Problems
 High Altitude Medical Problems Wilderness Basics Course 2-2015 Jeffrey H. Gertsch, MD Assistant Professor of Neurosciences UCSD School of Medicine Definition/Site ISMM Definitions Altitude in Meters Altitude
High Altitude Medical Problems Wilderness Basics Course 2-2015 Jeffrey H. Gertsch, MD Assistant Professor of Neurosciences UCSD School of Medicine Definition/Site ISMM Definitions Altitude in Meters Altitude
Do I have AMS or am I just Knackered?
 Do I have AMS or am I just Knackered? An excellent question and one that you should always be asking yourself as you ascend. Early onset of AMS is very difficult to diagnose as the symptoms can be very
Do I have AMS or am I just Knackered? An excellent question and one that you should always be asking yourself as you ascend. Early onset of AMS is very difficult to diagnose as the symptoms can be very
Unit 3: The Physiology of Diving and Nitrox
 Unit 3: The Physiology of Diving and Nitrox Narcosis Decompression Sickness Physiological Effects of High Oxygen Levels Physiological Effects of High Oxygen Levels Student Performance: By the end of the
Unit 3: The Physiology of Diving and Nitrox Narcosis Decompression Sickness Physiological Effects of High Oxygen Levels Physiological Effects of High Oxygen Levels Student Performance: By the end of the
High Altitude Concerns
 High Altitude Concerns 17 March, 2014 PRESENTED BY: John M. Davenport, Lt. Col., USAF, Ret. International Operators Conference Tampa, FL March 17 20, 2014 Welcome Aviators! High Altitude Concerns Question
High Altitude Concerns 17 March, 2014 PRESENTED BY: John M. Davenport, Lt. Col., USAF, Ret. International Operators Conference Tampa, FL March 17 20, 2014 Welcome Aviators! High Altitude Concerns Question
Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation.
, Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation.") Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation. Paradoxical breathing Hyper-resonance on percussion:
Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation. Paradoxical breathing Hyper-resonance on percussion:
So What Can I do About AMS?
 So What Can I do About AMS? T he symptoms of AMS will disappear 24-36 hours after appearing if you do not continue to ascend. If the symptoms persist then the only option is to descend to a lower altitude
So What Can I do About AMS? T he symptoms of AMS will disappear 24-36 hours after appearing if you do not continue to ascend. If the symptoms persist then the only option is to descend to a lower altitude
Challenge in High Altitude related Medical Emergency Recognize, Remedy and Risk Reduction
 Challenge in High Altitude related Medical Emergency Recognize, Remedy and Risk Reduction Dr. M K Ho Resident Consultant in Emergency Medicine Hong Kong Baptist Hospital (Statement of declare that there
Challenge in High Altitude related Medical Emergency Recognize, Remedy and Risk Reduction Dr. M K Ho Resident Consultant in Emergency Medicine Hong Kong Baptist Hospital (Statement of declare that there
American College of Occupational and Preventive Medicine 2011 Annual Meeting, Orlando, Florida, November 2, 2011
 Administrative Information Risk Assessment: Low AEROSPACE/ OCCUPATIONAL MEDICINE BAROMETRIC CONCERNS Dr. John Campbell, MFS Environmental Considerations: None Safety Considerations: None Evaluation: 50
Administrative Information Risk Assessment: Low AEROSPACE/ OCCUPATIONAL MEDICINE BAROMETRIC CONCERNS Dr. John Campbell, MFS Environmental Considerations: None Safety Considerations: None Evaluation: 50
Outdoor Medicine 2010
 Outdoor Medicine 2010 Outdoor Medicine Preparation Priorities Common injuries and illnesses High altitude illness Preparation Itinerary Extra food and water, filter or iodine Clothes base layer, insulation,
Outdoor Medicine 2010 Outdoor Medicine Preparation Priorities Common injuries and illnesses High altitude illness Preparation Itinerary Extra food and water, filter or iodine Clothes base layer, insulation,
DECOMPRESSION PHYSIOLOGY and SUSCEPTIBILITY
 Chapter 13 DECOMPRESSION PHYSIOLOGY and SUSCEPTIBILITY Decompression Sickness (DCS) is an illness caused by the effects of gas coming out of solution to form bubbles in the body after diving. It is due
Chapter 13 DECOMPRESSION PHYSIOLOGY and SUSCEPTIBILITY Decompression Sickness (DCS) is an illness caused by the effects of gas coming out of solution to form bubbles in the body after diving. It is due
ALTITUDE PHYSIOLOGY. Physiological Zones of the Atmosphere. Composition of the Air AIR ATTENDANTS COURSE. Sea Level Pressure
 AIR ATTENDANTS COURSE ALTITUDE PHYSIOLOGY Physical Divisions of the Atmosphere 1200 miles 600 miles EXOSPHERE Physiological Zones of the Atmosphere 50 miles IONOSPHERE SPACE EQUIVALENT ZONE: 50,000 feet
AIR ATTENDANTS COURSE ALTITUDE PHYSIOLOGY Physical Divisions of the Atmosphere 1200 miles 600 miles EXOSPHERE Physiological Zones of the Atmosphere 50 miles IONOSPHERE SPACE EQUIVALENT ZONE: 50,000 feet
O-1. American Osteopathic College of Occupational and Preventive Medicine 2013 Mid Year Educational Conference, Phoenix, Arizona February 14-17, 2013
 Administrative Information Risk Assessment: Low AEROSPACE/ OCCUPATIONAL MEDICINE BAROMETRIC CONCERNS Dr. John Campbell, DO, MPH, MFS Environmental Considerations: None Safety Considerations: None Evaluation:
Administrative Information Risk Assessment: Low AEROSPACE/ OCCUPATIONAL MEDICINE BAROMETRIC CONCERNS Dr. John Campbell, DO, MPH, MFS Environmental Considerations: None Safety Considerations: None Evaluation:
SPQ Module 9 Breathing at Altitude
 SPQ Module 9 Breathing at Altitude For most people traveling 1130 kilometers on foot over a frozen ice cap with no support would be daunting enough without facing the prospect of being short of breath
SPQ Module 9 Breathing at Altitude For most people traveling 1130 kilometers on foot over a frozen ice cap with no support would be daunting enough without facing the prospect of being short of breath
SECOND EUROPEAN CONSENSUS CONFERENCE ON HYPERBARIC MEDICINE THE TREATMENT OF DECOMPRESSION ACCIDENTS IN RECREATIONAL DIVING
 SECOND EUROPEAN CONSENSUS CONFERENCE ON HYPERBARIC MEDICINE THE TREATMENT OF DECOMPRESSION ACCIDENTS IN RECREATIONAL DIVING MARSEILLE, May 8-10, 1996 RECOMMENDATIONS OF THE JURY* QUESTION 1 : Is there
SECOND EUROPEAN CONSENSUS CONFERENCE ON HYPERBARIC MEDICINE THE TREATMENT OF DECOMPRESSION ACCIDENTS IN RECREATIONAL DIVING MARSEILLE, May 8-10, 1996 RECOMMENDATIONS OF THE JURY* QUESTION 1 : Is there
Successful use ofthe Gamow Hyperbaric Bag in the treatment ofaltitude illness at MountEverest
 Journal of Wilderness Medicine 1, 193-202 (1990) Successful use ofthe Gamow Hyperbaric Bag in the treatment ofaltitude illness at MountEverest SJ. KINGl* and R.R. GREENLEE2 1Departmentof Emergency Medicine,
Journal of Wilderness Medicine 1, 193-202 (1990) Successful use ofthe Gamow Hyperbaric Bag in the treatment ofaltitude illness at MountEverest SJ. KINGl* and R.R. GREENLEE2 1Departmentof Emergency Medicine,
b. Provide consultation service to physicians referring patients. c. Participate in weekly wound care clinic and biweekly diving medicine clinic.
 Curriculum: 1. Required clinical activities: a. Participate in HBO 2 clinical operations by monitoring daily treatment sessions and emergency on-call treatments at least 4 days/week, b. Provide consultation
Curriculum: 1. Required clinical activities: a. Participate in HBO 2 clinical operations by monitoring daily treatment sessions and emergency on-call treatments at least 4 days/week, b. Provide consultation
Decompression illness, or DCI, is a term used to describe illness that results
 Decompression Illness: By Dr. Ed Thalmann DAN America, 2004. Decompression illness, or DCI, is a term used to describe illness that results from a reduction in the ambient pressure surrounding a body.
Decompression Illness: By Dr. Ed Thalmann DAN America, 2004. Decompression illness, or DCI, is a term used to describe illness that results from a reduction in the ambient pressure surrounding a body.
Doc #: 1000-AD Revision: - WORKING AT ALTITUDE AWARENESS POLICY. Author(s): Tammie Lavoie, Miranda Saucedo, John Dunlop
: Tammie Lavoie, Miranda Saucedo, John Dunlop") Doc #: 1000-AD-015-0020 Revision: - WORKING AT ALTITUDE AWARENESS POLICY Author(s): Tammie Lavoie, Miranda Saucedo, John Dunlop TABLE OF CONTENTS REVISION HISTORY... 3 1.0 INTRODUCTION... 4 2.0 SIGNS/SYMPTOMS
Doc #: 1000-AD-015-0020 Revision: - WORKING AT ALTITUDE AWARENESS POLICY Author(s): Tammie Lavoie, Miranda Saucedo, John Dunlop TABLE OF CONTENTS REVISION HISTORY... 3 1.0 INTRODUCTION... 4 2.0 SIGNS/SYMPTOMS
Blood Gas Interpretation
 Blood Gas Interpretation Pa O2 Saturation (SaO 2 ) Oxygen Therapy Monitoring Oxygen content (O( 2 Ct) Venous Oximetry Mixed venous oxygen saturation SvO 2 Surrogate for Systemic oxygen delivery and
Blood Gas Interpretation Pa O2 Saturation (SaO 2 ) Oxygen Therapy Monitoring Oxygen content (O( 2 Ct) Venous Oximetry Mixed venous oxygen saturation SvO 2 Surrogate for Systemic oxygen delivery and
CHAPTER 6. Oxygen Transport. Copyright 2008 Thomson Delmar Learning
 CHAPTER 6 Oxygen Transport Normal Blood Gas Value Ranges Table 6-1 OXYGEN TRANSPORT Oxygen Dissolved in the Blood Plasma Dissolve means that the gas maintains its precise molecular structure About.003
CHAPTER 6 Oxygen Transport Normal Blood Gas Value Ranges Table 6-1 OXYGEN TRANSPORT Oxygen Dissolved in the Blood Plasma Dissolve means that the gas maintains its precise molecular structure About.003
Hyperbaric Oxygen Therapy
 Hyperbaric Oxygen Therapy WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A.,
Hyperbaric Oxygen Therapy WWW.RN.ORG Reviewed September 2017, Expires September 2019 Provider Information and Specifics available on our Website Unauthorized Distribution Prohibited 2017 RN.ORG, S.A.,
Office. Hypoxia. Or this. Or even this. Hypoxia E-1. COL Brian W. Smalley DO, MSPH, CPE
 Hypoxia Office COL Brian W. Smalley DO, MSPH, CPE Or this Or even this Hypoxia State of oxygen deficiency in the blood cells and tissues sufficient to cause impairment of function 4 Types Hypoxic Hypemic
Hypoxia Office COL Brian W. Smalley DO, MSPH, CPE Or this Or even this Hypoxia State of oxygen deficiency in the blood cells and tissues sufficient to cause impairment of function 4 Types Hypoxic Hypemic
Diving Medicine USN Diver/SEAL Submarine Overview / Tom Kersch, CAPT, MC!!
 Diving Medicine USN Diver/SEAL Submarine Overview / Tom Kersch, CAPT, MC Diving Medicine USN Diver/SEAL Submarine Overview Tom Kersch CAPT, MC SEAL Deliver Vehicle Team 1 Pearl City, HI 1 Content Attestation
Diving Medicine USN Diver/SEAL Submarine Overview / Tom Kersch, CAPT, MC Diving Medicine USN Diver/SEAL Submarine Overview Tom Kersch CAPT, MC SEAL Deliver Vehicle Team 1 Pearl City, HI 1 Content Attestation
DCI Demystified By Eric Hexdall, RN, CHRN Duke Dive Medicine
 DCI Demystified By Eric Hexdall, RN, CHRN Duke Dive Medicine Everyone who takes a formal diver training course receives at least a basic education in the signs, symptoms, etiology, and prevention of pressure-related
DCI Demystified By Eric Hexdall, RN, CHRN Duke Dive Medicine Everyone who takes a formal diver training course receives at least a basic education in the signs, symptoms, etiology, and prevention of pressure-related
Learning Objectives 9/12/2012. Chapter 30. Environmental Emergencies. Chapter Goal
 Chapter 30 Environmental Emergencies Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with environmentally induced or exacerbated emergencies Define
Chapter 30 Environmental Emergencies Chapter Goal Use assessment findings to formulate field impression & implement treatment plan for patients with environmentally induced or exacerbated emergencies Define
High altitude Headache. July KCGMH Lian Hui Lee
 High altitude Headache July 17.2010 KCGMH Lian Hui Lee High altitude Headache I. High altitude Headache (HAD) II. Flight Associated Headache 1. Altitude Sickness on Flights 2. Long-Haul Flights May Promote
High altitude Headache July 17.2010 KCGMH Lian Hui Lee High altitude Headache I. High altitude Headache (HAD) II. Flight Associated Headache 1. Altitude Sickness on Flights 2. Long-Haul Flights May Promote
Document is provided for sample purposes only. Content is not updated and should not be used for traveler counseling.
 Document is provided for sample purposes only. Content is not updated and should not be used for traveler counseling. Altitude Illness Medical Summary Introduction Altitude illness occurs when a traveler
Document is provided for sample purposes only. Content is not updated and should not be used for traveler counseling. Altitude Illness Medical Summary Introduction Altitude illness occurs when a traveler
Acute Mountain Sickness
 2012 Scottish Universities Medical Journal, Dundee Published online: Feb 2012 Vol 1 Issue 1: page 98-103 Gomersall T Acute Mountain Sickness Acute Mountain Sickness Tim Gomersall (2 nd Year MBChB) University
2012 Scottish Universities Medical Journal, Dundee Published online: Feb 2012 Vol 1 Issue 1: page 98-103 Gomersall T Acute Mountain Sickness Acute Mountain Sickness Tim Gomersall (2 nd Year MBChB) University
2010 NPC Team Physician Conference. Russ O Connor MD, FRCPC (PMR), Dip Sport Med CASM
, Dip Sport Med CASM") 2010 NPC Team Physician Conference Russ O Connor MD, FRCPC (PMR), Dip Sport Med CASM Overview Trauma and Injury patterns and rates Resuscitation issues Altitude Cold exposure Injury Epidemiology Limited
2010 NPC Team Physician Conference Russ O Connor MD, FRCPC (PMR), Dip Sport Med CASM Overview Trauma and Injury patterns and rates Resuscitation issues Altitude Cold exposure Injury Epidemiology Limited
EMS Subspecialty Certification Review Course. Learning Objectives. Question Environmental
 EMS Subspecialty Certification Review Course 1.2.5 Version: 2017 Learning Objectives Differentiate EMS treatment priorities for cold and heat related illnesses Describe EMS treatment considerations for
EMS Subspecialty Certification Review Course 1.2.5 Version: 2017 Learning Objectives Differentiate EMS treatment priorities for cold and heat related illnesses Describe EMS treatment considerations for
Exam Key. NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: % of grade in class
 NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: 100 20% of grade in class 1) An arterial blood sample for a patient at sea level is obtained, and the following physiological values
NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: 100 20% of grade in class 1) An arterial blood sample for a patient at sea level is obtained, and the following physiological values
Smith Seminars Online Continuing Education AARC-Approved for 2 CRCE Altitude-Related Disorders
 Smith Seminars Online Continuing Education AARC-Approved for 2 CRCE Altitude-Related Disorders Objectives Be able to describe the various medical problems associated with ascent to high altitude Understand
Smith Seminars Online Continuing Education AARC-Approved for 2 CRCE Altitude-Related Disorders Objectives Be able to describe the various medical problems associated with ascent to high altitude Understand
Over, Under, Hot and Cold. Jamie Syrett, MD Office of Prehospital Care Rochester General Health System
 Over, Under, Hot and Cold Jamie Syrett, MD Office of Prehospital Care Rochester General Health System Pulsecheck 2012 Reality EMS Under - Drowning Over - High Altitude Illness Hot - Hyperthermia Cold -
Over, Under, Hot and Cold Jamie Syrett, MD Office of Prehospital Care Rochester General Health System Pulsecheck 2012 Reality EMS Under - Drowning Over - High Altitude Illness Hot - Hyperthermia Cold -
Medical Aspects of Diving in the Offshore Oil Industry
 Medical Aspects of Diving in the Offshore Oil Industry Dr Stephen Watt Retired Consultant in Respiratory and Hyperbaric Medicine Chairman, Diving Medical Advisory Committee What is diving? Diving = Commuting
Medical Aspects of Diving in the Offshore Oil Industry Dr Stephen Watt Retired Consultant in Respiratory and Hyperbaric Medicine Chairman, Diving Medical Advisory Committee What is diving? Diving = Commuting
Environmental Considerations
 Environmental Considerations I. Hyperthermia a. Heat stress i. Take extreme caution in hot, humid weather ii. Every year athletes die from heat related causes iii. Body temperature must be obtained by
Environmental Considerations I. Hyperthermia a. Heat stress i. Take extreme caution in hot, humid weather ii. Every year athletes die from heat related causes iii. Body temperature must be obtained by
Diving Accident Management
 Diving Accident Management From Diving Medicine Online http://scuba-doc.com/ 3/8/2004 Diving Medicine Online 1 Introduction! It is desirable to have a standard approach to the initial management (i.e.
Diving Accident Management From Diving Medicine Online http://scuba-doc.com/ 3/8/2004 Diving Medicine Online 1 Introduction! It is desirable to have a standard approach to the initial management (i.e.
Lung Volumes and Capacities
 Lung Volumes and Capacities Normally the volume of air entering the lungs during a single inspiration is approximately equal to the volume leaving on the subsequent expiration and is called the tidal volume.
Lung Volumes and Capacities Normally the volume of air entering the lungs during a single inspiration is approximately equal to the volume leaving on the subsequent expiration and is called the tidal volume.
Patent Foramen Ovale and Fitness
 Guidelines for Patent Foramen Ovale and Fitness Proceedings Summary DAN/UHMS PFO and Fitness to Dive Workshop Introduction Prior to birth, oxygenated blood flows from the mother through the placenta to
Guidelines for Patent Foramen Ovale and Fitness Proceedings Summary DAN/UHMS PFO and Fitness to Dive Workshop Introduction Prior to birth, oxygenated blood flows from the mother through the placenta to
Physiology of Flight
 Physiology of Flight Physiology of Flight Physiology of flight: how the human body functions during flight Overview 1. Physiological Divisions of the Atmosphere 2. Hypoxia and Hyperventilation 3. Trapped
Physiology of Flight Physiology of Flight Physiology of flight: how the human body functions during flight Overview 1. Physiological Divisions of the Atmosphere 2. Hypoxia and Hyperventilation 3. Trapped
Environmental Injuries and the Athlete
 Environmental Injuries and the Athlete Presentation subtitle Heat Illness Hypothermia Frostbite Altitude Illness Month Day, Year Thomas Moran MD Northshore University Health System Clinician educator,
Environmental Injuries and the Athlete Presentation subtitle Heat Illness Hypothermia Frostbite Altitude Illness Month Day, Year Thomas Moran MD Northshore University Health System Clinician educator,
GENETIC INFLUENCE ON FACTORS OF OXYGEN TRANSPORT
 GENETIC INFLUENCE ON FACTORS OF OXYGEN TRANSPORT Claudio Marconi IBFM-Sect. of Muscle Physiology and Proteome National Research Council Milano, Italy 100 90 80 % s.l. VO 2 max. 70 60 50 40 30 20 10 0 2
GENETIC INFLUENCE ON FACTORS OF OXYGEN TRANSPORT Claudio Marconi IBFM-Sect. of Muscle Physiology and Proteome National Research Council Milano, Italy 100 90 80 % s.l. VO 2 max. 70 60 50 40 30 20 10 0 2
Hyperbarics 2 CEUs By: Michelle E. Duffelmeyer, MD. Co-author: Ellen Smithline, RN. Objectives
 Hyperbarics 2 CEUs By: Michelle E. Duffelmeyer, MD Co-author: Ellen Smithline, RN Objectives By the end of this lecture, the participant should be able to... 1. Describe the basic principles that explain
Hyperbarics 2 CEUs By: Michelle E. Duffelmeyer, MD Co-author: Ellen Smithline, RN Objectives By the end of this lecture, the participant should be able to... 1. Describe the basic principles that explain
Respiration (revised 2006) Pulmonary Mechanics
 Pulmonary Mechanics") Respiration (revised 2006) Pulmonary Mechanics PUL 1. Diagram how pleural pressure, alveolar pressure, airflow, and lung volume change during a normal quiet breathing cycle. Identify on the figure the
Respiration (revised 2006) Pulmonary Mechanics PUL 1. Diagram how pleural pressure, alveolar pressure, airflow, and lung volume change during a normal quiet breathing cycle. Identify on the figure the
USARIEM TECHNICAL NOTE 94-2 MEDICAL PROBLEMS IN HIGH MOUNTAIN ENVIRONMENTS. A Handbook for Medical Officers
 AD USARIEM TECHNICAL NOTE 94-2 MEDICAL PROBLEMS IN HIGH MOUNTAIN ENVIRONMENTS A Handbook for Medical Officers U S ARMY RESEARCH INSTITUTE OF ENVIRONMENTAL MEDICINE Natick, Massachusetts 01760-5007 February
AD USARIEM TECHNICAL NOTE 94-2 MEDICAL PROBLEMS IN HIGH MOUNTAIN ENVIRONMENTS A Handbook for Medical Officers U S ARMY RESEARCH INSTITUTE OF ENVIRONMENTAL MEDICINE Natick, Massachusetts 01760-5007 February
Pulmonary Circulation Linda Costanzo Ph.D.
 Pulmonary Circulation Linda Costanzo Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The differences between pressures in the pulmonary and systemic circulations. 2. How
Pulmonary Circulation Linda Costanzo Ph.D. OBJECTIVES: After studying this lecture, the student should understand: 1. The differences between pressures in the pulmonary and systemic circulations. 2. How
Control of Respiration. Central Control of Ventilation
 Central Control of Goal: maintain sufficient ventilation with minimal energy Process steps: mechanics + aerodynamics Points of Regulation Breathing rate and depth, coughing, swallowing, breath holding
Central Control of Goal: maintain sufficient ventilation with minimal energy Process steps: mechanics + aerodynamics Points of Regulation Breathing rate and depth, coughing, swallowing, breath holding
REMOTE LOCATION FIRST AID
 LESSON 23 REMOTE LOCATION FIRST AID 23-1 First Aid Differences in Remote Locations Most first aid based on fact that help will arrive within 10 20 minutes of 9-1-1 call Most first aid intended to meet
LESSON 23 REMOTE LOCATION FIRST AID 23-1 First Aid Differences in Remote Locations Most first aid based on fact that help will arrive within 10 20 minutes of 9-1-1 call Most first aid intended to meet
CARBON MONOXIDE POISONING
 CARBON MONOXIDE POISONING Matthew Valento, MD Assistant Professor, UW Department of Emergency Medicine Washington Poison Center Carbon monoxide (CO) Incomplete combustion of carbon-containing compounds
CARBON MONOXIDE POISONING Matthew Valento, MD Assistant Professor, UW Department of Emergency Medicine Washington Poison Center Carbon monoxide (CO) Incomplete combustion of carbon-containing compounds
Essential Skills Course Acute Care Module. Respiratory Day 2 (Arterial Blood Gases) Pre course Workbook
 Pre course Workbook") Essential Skills Course Acute Care Module Respiratory Day 2 (Arterial Blood Gases) Pre course Workbook Acknowledgements This pre course workbook has been complied and updated with reference to the original
Essential Skills Course Acute Care Module Respiratory Day 2 (Arterial Blood Gases) Pre course Workbook Acknowledgements This pre course workbook has been complied and updated with reference to the original
GEMINI VISITOR S GUIDE VISITOR S VERSION
 Gemini Observatory Northern Operations Center 670 N. A ohoku Place, Hilo, Hawaii 96720 Phone: (808) 974-2500 Fax: (808) 974-2589 Dear Visitor, For your personal safety, please read this entire safety policy
Gemini Observatory Northern Operations Center 670 N. A ohoku Place, Hilo, Hawaii 96720 Phone: (808) 974-2500 Fax: (808) 974-2589 Dear Visitor, For your personal safety, please read this entire safety policy
Rescue Swimmer Refresher Course. Practical First Aid Training/Mock Trauma LT 2.2
 Rescue Swimmer Refresher Course Practical First Aid Training/Mock Trauma LT 2.2 Enabling Objectives Respond to an emergency per current American Red Cross standards. Administer CPR per current American
Rescue Swimmer Refresher Course Practical First Aid Training/Mock Trauma LT 2.2 Enabling Objectives Respond to an emergency per current American Red Cross standards. Administer CPR per current American
Breathing Process: Inhalation
 Airway Chapter 6 Breathing Process: Inhalation Active part of breathing Diaphragm and intercostal muscles contract, allowing the lungs to expand. The decrease in pressure allows lungs to fill with air.
Airway Chapter 6 Breathing Process: Inhalation Active part of breathing Diaphragm and intercostal muscles contract, allowing the lungs to expand. The decrease in pressure allows lungs to fill with air.
PHTY 300 Wk 1 Lectures
 PHTY 300 Wk 1 Lectures Arterial Blood Gas Components The test provides information on - Acid base balance - Oxygenation - Hemoglobin levels - Electrolyte blood glucose, lactate, renal function When initially
PHTY 300 Wk 1 Lectures Arterial Blood Gas Components The test provides information on - Acid base balance - Oxygenation - Hemoglobin levels - Electrolyte blood glucose, lactate, renal function When initially
Rodney Shandukani 14/03/2012
 Rodney Shandukani 14/03/2012 OXYGEN THERAPY Aerobic metabolism accounts for 90% of Oxygen consumption by tissues. generates ATP by oxidative phosphorylation. Oxygen cascade: Oxygen exerts a partial pressure,
Rodney Shandukani 14/03/2012 OXYGEN THERAPY Aerobic metabolism accounts for 90% of Oxygen consumption by tissues. generates ATP by oxidative phosphorylation. Oxygen cascade: Oxygen exerts a partial pressure,
STANDARD OPERATING PROCEDURES TACTICAL OPERATIONS NERVE AGENT RESPONSE EFFECTIVE: OCTOBER 2007
 STANDARD OPERATING PROCEDURES TACTICAL OPERATIONS 202.12 NERVE AGENT RESPONSE EFFECTIVE: OCTOBER 2007 BACKGROUND The following establishes procedures for treatment in the event that Department members
STANDARD OPERATING PROCEDURES TACTICAL OPERATIONS 202.12 NERVE AGENT RESPONSE EFFECTIVE: OCTOBER 2007 BACKGROUND The following establishes procedures for treatment in the event that Department members
Hyperbaric Oxygen Therapy Patient Information
 Hyperbaric Oxygen Therapy Patient Information One of only two in Wichita, Kansas, our hyperbaric oxygen chamber is truly unique. Hyperbaric therapy was originally used to treat deep sea divers who were
Hyperbaric Oxygen Therapy Patient Information One of only two in Wichita, Kansas, our hyperbaric oxygen chamber is truly unique. Hyperbaric therapy was originally used to treat deep sea divers who were
ANNEX D: PHYSIOLOGICAL EPISODES
 1. The Navy s definition of a physiological episode (PE) is when a pilot experiences loss in performance related to insufficient oxygen, depressurization, or other factors during flight. For the purposes
1. The Navy s definition of a physiological episode (PE) is when a pilot experiences loss in performance related to insufficient oxygen, depressurization, or other factors during flight. For the purposes
Hyperbaric Oxygen Therapy
 1 RSPT 1410 Medical Gas Therapy Part 2: Wilkins: Chapter 38; p. 891-894 Cairo: Chapter 3, p. 78-81 2 Definitions Hyperbaric oxygen (HBO) therapy is the therapeutic use of oxygen at pressures greater than
1 RSPT 1410 Medical Gas Therapy Part 2: Wilkins: Chapter 38; p. 891-894 Cairo: Chapter 3, p. 78-81 2 Definitions Hyperbaric oxygen (HBO) therapy is the therapeutic use of oxygen at pressures greater than
VENTILATION AND PERFUSION IN HEALTH AND DISEASE. Dr.HARIPRASAD VS
 VENTILATION AND PERFUSION IN HEALTH AND DISEASE Dr.HARIPRASAD VS Ventilation Total ventilation - total rate of air flow in and out of the lung during normal tidal breathing. Alveolar ventilation -represents
VENTILATION AND PERFUSION IN HEALTH AND DISEASE Dr.HARIPRASAD VS Ventilation Total ventilation - total rate of air flow in and out of the lung during normal tidal breathing. Alveolar ventilation -represents
Aurora Health Care South Region EMS rd Quarter CE Packet
 Aurora Health Care South Region EMS 2010 3 rd Quarter CE Packet Carbon Monoxide and Cyanide Poisoning www.aurorahealthcare.org Carbon monoxide is the leading cause of poisoning in the United States for
Aurora Health Care South Region EMS 2010 3 rd Quarter CE Packet Carbon Monoxide and Cyanide Poisoning www.aurorahealthcare.org Carbon monoxide is the leading cause of poisoning in the United States for
- How do the carotid bodies sense arterial blood gases? o The carotid bodies weigh 25mg, yet they have their own artery. This means that they have
 - How do the carotid bodies sense arterial blood gases? o The carotid bodies weigh 25mg, yet they have their own artery. This means that they have the highest blood flow of all organs, which makes them
- How do the carotid bodies sense arterial blood gases? o The carotid bodies weigh 25mg, yet they have their own artery. This means that they have the highest blood flow of all organs, which makes them
S.I.T.E.M.S.H Congress
 S.I.T.E.M.S.H Congress Tehran University of Medical Sciences (TUMS) December 2015, Tehran Farzin Halabchi M.D. Associate Professor, Sports & Exercise Medicine, TUMS Head, Iranian Association of Sports
S.I.T.E.M.S.H Congress Tehran University of Medical Sciences (TUMS) December 2015, Tehran Farzin Halabchi M.D. Associate Professor, Sports & Exercise Medicine, TUMS Head, Iranian Association of Sports
Welcome to Alpharetta Wellness Clinic Mild Hyperbaric Oxygen Therapy! We are committed to providing quality and affordable therapy to our clients!
 Welcome to Alpharetta Wellness Clinic Mild Hyperbaric Oxygen Therapy! Below you will find many answers to your questions about Mild Hyperbaric Oxygen Therapy. If you do not find the answers please feel
Welcome to Alpharetta Wellness Clinic Mild Hyperbaric Oxygen Therapy! Below you will find many answers to your questions about Mild Hyperbaric Oxygen Therapy. If you do not find the answers please feel
4/18/2012. Northern Fur Seal Three Foraging Patterns. Thermocline. Diving Physiology and Behavior
 Northern Fur Seal Three Foraging Patterns Thermocline Diving Physiology and Behavior 1 Fundamental Constraint on Foraging Behavior Return to Surface to Breathe 2 Studies of Dive Behavior Dive depths from
Northern Fur Seal Three Foraging Patterns Thermocline Diving Physiology and Behavior 1 Fundamental Constraint on Foraging Behavior Return to Surface to Breathe 2 Studies of Dive Behavior Dive depths from
Some Diving Physics and Physiology; Barotrauma. Robbert Hermanns Occupational Health Risk Management Services Ltd
 Some Diving Physics and Physiology; Barotrauma Robbert Hermanns Occupational Health Risk Management Services Ltd Oil & Gas UK (EBS) conference th 24 May 2017 Dr Robbert Hermanns MFOM Robbert.hermanns@ohrms.co.uk
Some Diving Physics and Physiology; Barotrauma Robbert Hermanns Occupational Health Risk Management Services Ltd Oil & Gas UK (EBS) conference th 24 May 2017 Dr Robbert Hermanns MFOM Robbert.hermanns@ohrms.co.uk
More Water, Less Bubbles
 HYDRATION More Water, Less Bubbles PROMOTING THE IMPORTANCE OF HYDRATION IN DIVING INTRODUCTION Dehydration and its influence on diving safety Dehydration occurs when your body loses more fluid than is
HYDRATION More Water, Less Bubbles PROMOTING THE IMPORTANCE OF HYDRATION IN DIVING INTRODUCTION Dehydration and its influence on diving safety Dehydration occurs when your body loses more fluid than is
EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES
 GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
Cold and Heat Emergencies Video Cold & Heat Emergencies
 CHAPTER 20 Cold and Heat Emergencies Video Cold & Heat Emergencies Lesson Objectives 1. Describe the different types of cold and heat emergencies and what you can do to prevent them. 2. Explain factors
CHAPTER 20 Cold and Heat Emergencies Video Cold & Heat Emergencies Lesson Objectives 1. Describe the different types of cold and heat emergencies and what you can do to prevent them. 2. Explain factors
To develop understanding of mental and physical standards required for operating an aircraft
 Aeromedical Factors Objective To develop understanding of mental and physical standards required for operating an aircraft Outline Obtaining a medical certificate Causes, symptoms, effects, and corrective
Aeromedical Factors Objective To develop understanding of mental and physical standards required for operating an aircraft Outline Obtaining a medical certificate Causes, symptoms, effects, and corrective
Immersion pulmonary oedema: is it confused with drowning?
 Immersion pulmonary oedema: is it confused with drowning? Dr Peter Wilmshurst Consultant Cardiologist Royal Stoke University Hospital & UK Diving Medical Committee Drowning and pulmonary oedema Drowning
Immersion pulmonary oedema: is it confused with drowning? Dr Peter Wilmshurst Consultant Cardiologist Royal Stoke University Hospital & UK Diving Medical Committee Drowning and pulmonary oedema Drowning
Hyperbaric Oxygen and TBI: What Does Science Tell Us. Kathleen Bell, MD Department of Rehabilitation Medicine
 Hyperbaric Oxygen and TBI: What Does Science Tell Us Kathleen Bell, MD Department of Rehabilitation Medicine Look at scientific research on using hyperbaric oxygen treatment and neurofeedback treatment
Hyperbaric Oxygen and TBI: What Does Science Tell Us Kathleen Bell, MD Department of Rehabilitation Medicine Look at scientific research on using hyperbaric oxygen treatment and neurofeedback treatment
Urgent Hyperbaric Oxygen Therapy
 Urgent Hyperbaric Oxygen Therapy Information for patients and families Read this booklet to learn: what hyperbaric oxygen therapy is what it helps treat what happens after your therapy who to call if you
Urgent Hyperbaric Oxygen Therapy Information for patients and families Read this booklet to learn: what hyperbaric oxygen therapy is what it helps treat what happens after your therapy who to call if you
The Allure of the Deep
 The Allure of the Deep by Bob Bailey Many divers, especially newer divers, develop a fascination for how deep they can go. I can recall that, as a new diver, I couldn t wait to notch my first 100-foot
The Allure of the Deep by Bob Bailey Many divers, especially newer divers, develop a fascination for how deep they can go. I can recall that, as a new diver, I couldn t wait to notch my first 100-foot
UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION MUST, AT ALL TIMES, ACCEPT THE ENTIRE CARDIAC OUTPUT
 UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION MUST, AT ALL TIMES, ACCEPT THE ENTIRE CARDIAC OUTPUT UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION
UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION MUST, AT ALL TIMES, ACCEPT THE ENTIRE CARDIAC OUTPUT UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION
NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: % of grade in class
 NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: 100 20% of grade in class 1) An arterial blood sample for a patient at sea level is obtained, and the following physiological values
NROSCI/BIOSC 1070 and MSNBIO 2070 Exam # 2 October 28, 2016 Total POINTS: 100 20% of grade in class 1) An arterial blood sample for a patient at sea level is obtained, and the following physiological values
OUTLINE SHEET Respond to an emergency per current American Red Cross standards.
 INTRODUCTION OUTLINE SHEET 2.2-1 PRACTICAL FIRST AID TRAINING/MOCK TRAUMA PAGE 1 of 8 First Aid, in any situation, consists of emergency treatment of the sick or injured before medical help can be obtained.
INTRODUCTION OUTLINE SHEET 2.2-1 PRACTICAL FIRST AID TRAINING/MOCK TRAUMA PAGE 1 of 8 First Aid, in any situation, consists of emergency treatment of the sick or injured before medical help can be obtained.
CHAPTER 9 $LU'HFRPSUHVVLRQ
 CHAPTER 9 $LU'HFRPSUHVVLRQ 9-1 INTRODUCTION 9-1.1 Purpose. This chapter discusses decompression requirements for air diving operations. 9-1.2 Scope. This chapter discusses five different tables, each with
CHAPTER 9 $LU'HFRPSUHVVLRQ 9-1 INTRODUCTION 9-1.1 Purpose. This chapter discusses decompression requirements for air diving operations. 9-1.2 Scope. This chapter discusses five different tables, each with
PHYSIOLOGY. Let s look at the route in sequence, starting at the lungs where the blood releases CO2 and takes on oxygen at the pulmonary capillaries.
 PHYSIOLOGY Circulation: Blood circulates around your body to fuel the body with oxygen, the body uses the oxygen and changes it to carbon dioxide (CO2) the blood then carries this back to the lungs where
PHYSIOLOGY Circulation: Blood circulates around your body to fuel the body with oxygen, the body uses the oxygen and changes it to carbon dioxide (CO2) the blood then carries this back to the lungs where
Altitude and Travel. Philippe Lagacé-Wiens MD, DTM&H, FRCPC
 Altitude and Travel Philippe Lagacé-Wiens MD, DTM&H, FRCPC Outline Basic physiology of altitude medicine The dangers of altitude and acute altitude illnesses. Diagnosis of altitude related illnesses Treatment
Altitude and Travel Philippe Lagacé-Wiens MD, DTM&H, FRCPC Outline Basic physiology of altitude medicine The dangers of altitude and acute altitude illnesses. Diagnosis of altitude related illnesses Treatment
Respiratory Physiology. Adeyomoye O.I
 Respiratory Physiology By Adeyomoye O.I Outline Introduction Hypoxia Dyspnea Control of breathing Ventilation/perfusion ratios Respiratory/barometric changes in exercise Intra-pulmonary & intra-pleural
Respiratory Physiology By Adeyomoye O.I Outline Introduction Hypoxia Dyspnea Control of breathing Ventilation/perfusion ratios Respiratory/barometric changes in exercise Intra-pulmonary & intra-pleural
Ascent to Altitude After Diving
 Ascent to Altitude After Diving On many occasions, divers have a need to ascend to a higher altitude after diving, and they need guidance on how long they need to wait before doing so. The reason they
Ascent to Altitude After Diving On many occasions, divers have a need to ascend to a higher altitude after diving, and they need guidance on how long they need to wait before doing so. The reason they
Wildland Fire School. Heat Illness Prevention Program
 Monterey County Fire Training Officers Association www.mcftoa.org Heat Illness Prevention Program I. Purpose: The purpose of this program is to provide a safe training environment for attendees and participants
Monterey County Fire Training Officers Association www.mcftoa.org Heat Illness Prevention Program I. Purpose: The purpose of this program is to provide a safe training environment for attendees and participants
Outline What is it and what to expect Pilot physiology Oxygen equipment per FAA Wave windows Relevant FAR s NCSA Rules
 Northern California Soaring Association 2010 Safety Seminar High Altitude Wave Flight Considerations by Mike Voie, CFIG Outline What is it and what to expect Pilot physiology Oxygen equipment per FAA Wave
Northern California Soaring Association 2010 Safety Seminar High Altitude Wave Flight Considerations by Mike Voie, CFIG Outline What is it and what to expect Pilot physiology Oxygen equipment per FAA Wave
Health Forensics Steven Magee. Altitude
 Copyright Steven Magee Health Forensics Steven Magee Altitude I have a lot of experience with altitude. I spent three years working at approximately 7,775 feet followed by five years at 13,796 feet and
Copyright Steven Magee Health Forensics Steven Magee Altitude I have a lot of experience with altitude. I spent three years working at approximately 7,775 feet followed by five years at 13,796 feet and
Aviation Medicine Seminar Series
 Aviation Medicine Seminar Series Bruce R. Gilbert, M.D., Ph.D. Associate Clinical Professor of Urology Weill Cornell Medical College Stony Brook University Medical College Head, Section of Male Reproduction
Aviation Medicine Seminar Series Bruce R. Gilbert, M.D., Ph.D. Associate Clinical Professor of Urology Weill Cornell Medical College Stony Brook University Medical College Head, Section of Male Reproduction
Chapter 9 Airway Respirations Metabolism Oxygen Requirements Respiratory Anatomy Respiratory Anatomy Respiratory Anatomy Diaphragm
 1 Chapter 9 Airway 2 Respirations Every cell of the body requires to survive Oxygen must come in and carbon must go out 3 Metabolism Metabolism--Process where the body s cells convert food to Adequate
1 Chapter 9 Airway 2 Respirations Every cell of the body requires to survive Oxygen must come in and carbon must go out 3 Metabolism Metabolism--Process where the body s cells convert food to Adequate
An Overview of Decompression
 Diving Medicine just add water An Overview of Decompression Vandenhoven Guy, M.D., Ph.D. BVOOG Belgische Vereniging voor Overdruk en Onderwater Geneeskunde HEPHS - ISEK - Environmental, Ageing & Occupational
Diving Medicine just add water An Overview of Decompression Vandenhoven Guy, M.D., Ph.D. BVOOG Belgische Vereniging voor Overdruk en Onderwater Geneeskunde HEPHS - ISEK - Environmental, Ageing & Occupational
Some major points on the Effects of Hypoxia
 Some major points on the Effects of Hypoxia Source: Kings College London http://www.kcl.ac.uk/teares/gktvc/vc/dental/year1/lectures/rbmsmajorpoints/effectsofhypoxia.htm Cells obtain their energy from oxygen.
Some major points on the Effects of Hypoxia Source: Kings College London http://www.kcl.ac.uk/teares/gktvc/vc/dental/year1/lectures/rbmsmajorpoints/effectsofhypoxia.htm Cells obtain their energy from oxygen.