A ONE-WAY-VALVE CHEST WOUND DRESSING: EVALUATION IN A CANINE MODEL OF OPEN CHEST WOUNDS
|
|
|
- Hugh Carter
- 6 years ago
- Views:
Transcription
1 A ONE-WAY-VALVE CHEST WOUND DRESSING: EVALUATION IN A CANINE MODEL OF OPEN CHEST WOUNDS Ernest Ruiz, M.D., F.A.C.E.P. Assistant Professor of Surgery University of Minnesota Department of Emergency Medicine Hennepin County Medical Center Jonathan Lueders, M.D. Emergency Medicine Resident Hennepin County Medical Center Christian Petersen Medical Student University of Minnesota From Department of Emergency Medicine Hennepin County Medical Center 701 Park Avenue Minneapolis, Minnesota and Minneapolis Medical Research Foundation 914 South 8 th Street Minneapolis, Minnesota Supported in part with a grant from: Brunswick Biomedical Technologies, Inc. 6 Thacher lane Wareham, Massachusetts 02571
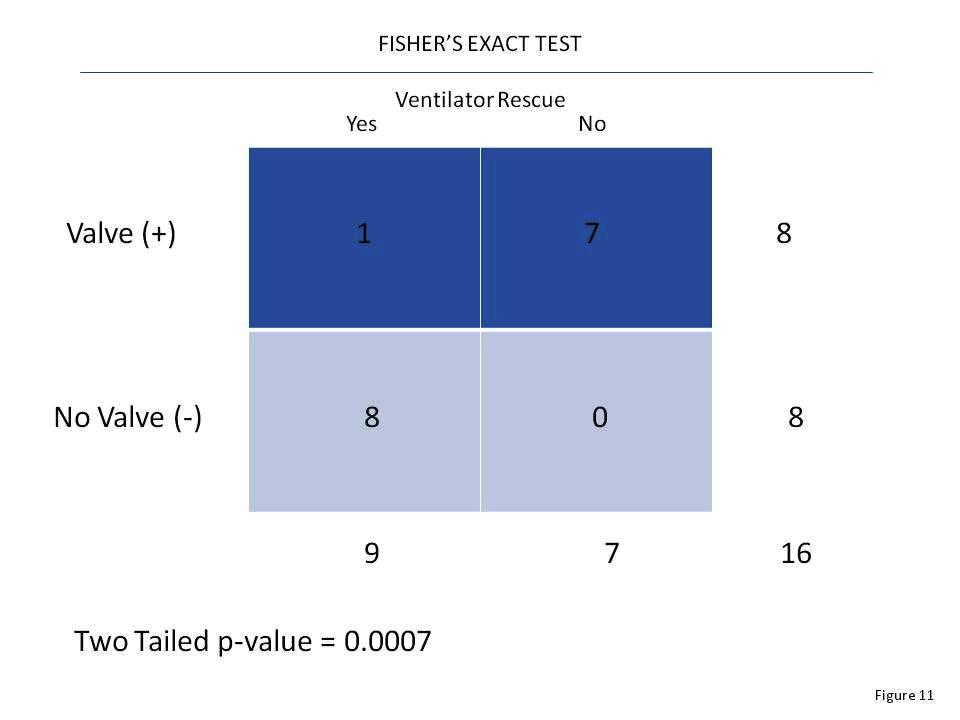
2 ABSTRACT Objective: To test a chest wound dressing incorporating a low profile oneway valve dressing (OWVD) designed for use in prehospital treatment of pneumothorax in penetrating chest trauma by comparing it to conventional petrolatum impregnated gauze dressings (PGD). Design: six dogs were used to develop an anesthetized breathing model using ketamine (40 mg/kg), midazolam (200 ug/kg), and fentanyl (10 ug/kg) maintained with an infusion of 600 ug/kg/min, 5 ug/kg/min, and.5 ug/kg/min respectively. Four dogs served as a control group evaluation this model on and off the ventilator. Eight dogs with bilateral standardized chest wounds were randomized into two groups in a crossover design study. One group tested the PGD first and then the OWVD, both with and without positive pressure ventilation (PPV). The second group tested the OWVD then the PGD. Dogs were stabilized between tests of each device. Respiratory rate, heart rate, arterial blood gases and hemoglobin oxygen saturation (qualitative) were monitored. Results: The control group showed stable vital signs throughout testing. Animals on PPV maintained stable vital signs regardless of the dressing applied. Dogs without PPV were unable to survive a 15 minute period with the PGD, whereas dogs with the OWVD were able to adequately maintain vital signs. The OWVD prevented collapse in 7 of 8 tests while the PGD prevented collapse in none of 8 tests in dogs without PPV. A probability of p = was found when Fisher s exact test was applied to this combined data. Conclusion: The OWVD out-performed the conventional PGD in preventing severe decompensation in dogs with bilateral open chest wounds without PPV.
3 INTRODUCTION The purpose of our study is to test a chest wound dressing incorporating a one-way valve and compare it to the traditional occlusive petrolatum gauze dressing used in pre-hospital care of penetrating chest wounds. A simple, disposable chest wound dressing incorporating a light weight, low profile, and low resistance silicone-leaflet one-way valve has recently become available. Penetrating chest wounds are increasing at an astronomical rate1. These patients pose difficult pre-hospital problems. The patient is usually unstable and in need of immediate transport. The traditional sterile occlusive dressing taped to the skin on three sides is difficult and time consuming to apply under field conditions. Frequently there are multiple wounds to manage, as in through and through gunshot wounds. The open, sucking chest wound allows air to enter the chest and separate the visceral and parietal pleural surfaces, breaking the thin fluid layer between the lung and chest wall. The elastic tissues of the lung normally produce a physiologic negative pressure differential between the potential intrapleural space and the outside of 4 12 cm water2. The elastic recoil of the lung causes it to pull away from the chest wall and air is drawn into the chest through the wound. Unassisted ventilation becomes impossible when respiratory movements of the chest wall and diaphragms result only in air movement through the wound instead of through oropharynx. If the wound is small, the patient can compensate with exaggerated chest wall and diaphragmatic movement because the wound offers more resistance to air flow than the bronchial tree and airway. It has been estimated that wound two-thirds the diameter of the trachea offers less resistance than the normal
4 airway3. When positive pressures is used, the lung can expand if air moves out of the wound or if the pressure of ventilation is high enough to compress the air within the pleural space. Tension pneumothorax can develop if there is a lung injury with an air leak into the pleural space and the wound is occluded or functions as a one-way valve allowing air into but not out of the chest. Tension pneumothorax can develop with or without positive pressure ventilation. A small pneumothorax can quickly become a tension pneumothorax when positive pressure ventilation is added to an occluded wound with underlying lung injury and air leak. An ideal dressing should possess certain qualities. It should be simple, quick, easily applied, and non-invasive. It should have a low profile and be sturdy enough to be used on the posterior thorax of a supine patient. Most importantly it should prevent influx of air on spontaneous inspiration through the wound and allow escape of air from the potential pleural space during any escape of air from the potential pleural space during any phase of respiration or assisted ventilation to avoid a tension pneumothorax. A disposable chest wound dressing incorporating a light weight, low profile and low resistance silicone leaf one-way valve has become available. This chest wound dressing appears to satisfy the qualities discussed above. From experience at our institution, conventional occlusive petrolatum-gauze dressings are frequently unreliable in preventing influx and allowing egress of air from a chest wound. It is virtually impossible for providers to place these dressings while wearing latex gloves and to get tape to stick to a bloody surface. They are time consuming to place at a time when other procedures also need to be performed. This study was designed to determine if this device in a laboratory model of open chest wounds.
5 MATERIALS AND METHODS Approval of the institutional animal use review committee was obtained for this study. A total of 18 mature mongrel dogs weight 10 to 25 kg were used. Six dogs were used to develop an anesthesia regimen that reliably resulted in a fully anesthetized but breathing model. The regimen included an IV anesthetizing dose of midazolam HCL, 200 ug/kg, alfentanil citrate, 10 ug/kg, and ketamine HCL, 40 mg/kg. Anesthesia was maintained with an infusion pump delivering a solution of midazolam HCL, 5 ug/kg/min, alfentanyl citrate 0.4 ug/kg/min, and ketamine HCL, 600 ug/kg/min. If a dog made spontaneous non-ventilatory movements, additional IV boluses of midazolam HCL, 100 ug/kg were given during the experimental period. All dogs were monitored as follows: Hemoglobin O2 saturation (SaO2) using a Oxisensor adult digit oxygen transducer wrapped around the tongue; Heart rate (HR) using ECG lead II; Central venous pressure (CVP) and mean arterial pressure (MAP) monitored via catheters placed percutaneously into an external jugular vein and femoral artery; Core temperature (CT) using an esophageal probe. The SaO2, HR, MAP and CT were displayed and recorded using a Hewlett-Packard Merlin monitoring system and pressure transducer. CVP was measured using a saline manometer in mmh2o = Pa). Arterial blood gases were measured using a Corning Model 168 blood gas analyzer. All dogs had their chests, neck, and groins shaved after induction of anesthesia. All dogs were orotracheally intubated using a cuffed 8.5 mm I.D. tube. Positive pressure ventilation with room air with a Bennett MA-1 respirator at ten breaths per minute with a tidal volume taken from the Kleinman ventilation graph plus 50 cc to compensate for dead-space in the
6 apparatus. Peak flow was set at 30 L/min. Sigh ventilations of 1000 cc were administered as needed to return the animal to stable state between experimental periods. An infra red heating lamp was placed over the torso to maintain body temperature at 37.0 to 38.5 C. Dogs that were to receive open chest wounds had plastic sleeves with an internal diameter of 6 mm placed bilaterally in the 6 th intercostal space at the anterior axillary line using a guidewire technique. The sleeves were curved to conform to the chest wall and were 7 cm in length with multiple side holes. They were sutured flush to the skin. This ended the period of preparation. Twelve dogs were randomly assigned to one of three groups. Group 3 consisted of four dogs and served as in anesthesia control group. They were monitored at five minute internals for four 20 minute periods, the first and third in which they were breathing spontaneously while the second and fourth were respirator dependant. Groups 1 and 2 were the experimental groups. These dogs had bilateral chest holes placed followed by the application of chest suction to the sleeves at 200 mm of H2O vacuum while on the respirator allowing them to recover from the brief collapse of the lungs cased by the procedure. After a fifteen minute period of stabilization the lungs were allowed to collapse by removing the respirator and chest wall suction for one minute. Either the conventional gauze dressing of the experimental one-way valve dressing was then applied as shown in our experimental algorhytm (Figure 1). During this time the dressings were tested with fifteen minute trials on and off the respirator respectively. The dressing was then removed and the dogs were placed back on the respirator and chest wall suction for a fifteen minute period of restabilization. Lungs were collapsed again by removal of the respirator and chest wall suction for
7 one minute. The opposite dressing as used before was then applied and tested with fifteen minute trials on and then off the respirator. Following this the dogs were euthanized with an IV KCL bolus. The petroleum gauze (PG) dressings were placed over the chest holes, molded to the chest and taped using two inch strips of waterproof adhesive tape. The one-way valve (OWV) dressings were placed over the chest holed and pasted to the skin with silicone sealant. If a dog became agonal with a SaO2 of less than 50 percent while off the respirator, the respirator was reapplied and sigh ventilations were used to re-expand the lungs. When a dog was unable to sustain itself during the fifteen minute trial without respirator support, multiple attempts were made to re-stabilize the dog and try again until the fifteen minute trial had elapsed. One dog randomly assigned to Group 2 was found to have evidence of pneumonia with copious purulent drainage from the trachea and severe hypotension / hypoxia throughout. Another dog was subsequently added to Group 2 and the dog with pneumonia eliminated from the study. One other dog had black pigmentation of the tongue which interfered with SaO2 measurements. In this instance, the dog s vital signs and ECG were used to confirm an agonal condition. RESULTS Anesthesia control Group 3 revealed no significant deterioration of vital signs or blood gases over the experimental period. See Figure 2. We then compared data from Groups 1 and 2 which showed that vital signs of dogs testing the gauze and one-way valve dressings were very stable and similar while the dogs were being ventilated.
8 Data from Group 1A and 2B which represents gauze dressing results was compared with data from Groups 2A and 1B which represents the valve dressing results. Figure 3 graphs the gauze results compared to valve results. Both dressings appeared perform similar based on vital signs. We then looked at whether it made any difference if the dressing was tested early (Groups 1A and 2A) prior to testing the opposite dressing, or late (groups 2A and 2B) after previously testing the opposite dressing. Figure 4 shows these vitals also little variation. This finding allowed the combining of data from groups 1 and 2 to determine the significance of differences in response to either of the two variable dressings. Data showed that both dressings performed equal when dogs were supported by the respirator. There was a very significant difference between the two dressings when the dogs were not supported with a respirator. The one-way valve dressing protected the dogs from severe collapse 7 out of 8 times. Figure 5 shows mean arterial blood pressure of the dogs testing the valve dressing after respirator support has been removed. Mean pressure remains stable. Figure 6 show the heart rate of this same group which also remains stable. Only one dog required rescue support by being placed back on the respirator for three minutes as shown in Figure 7. In contrast, dogs testing the gauze dressings were very unstable and none of them survived the 15 minute trial without rescue and ventilatory support. These vital signs were very unstable, and much of the time actually represents time on a respirator during rescue periods. Figure 10 shows these rescue periods. Figure 10 shows these rescue periods which all eight dogs testing the gauze dressing required. Multiple attempts for rescue were performed in most dogs.
9 ANALYSIS Descriptive statistical techniques were used to determine the stability of the anesthesia control group. Descriptive statistical techniques were also used to determine the effect of the timing of experimental variable periods in group 1 and 2. Fisher s Exact Test of probability was used to determine if there was a significant difference in performance of the two dressings with and without respirator support giving a p value of See Figure 11. DISCUSSION Bench research of pneumothorax and tension pneumothorax is severely limited by the anatomic characteristics of most laboratory animals. The dog, pig, cat, rabbit, and rat all have an incomplete mediastinum4. Sheep and goats do have a complete mediastinum 5 but are relatively unavailable in the laboratory setting. Since the dog has an oxyhemoglobin dissociation curve almost identical to that of humans, very similar blood viscosity properties and red blood cell size and configuration, we elected to develop our model using dogs6. By placing a hole on both sides of the chest we created a severe, constant model of open chest wound simulating bilateral chest wounds in humans. The conventional method of pre-hospital treatment of penetrating chest wounds is to apply an occlusive dressing. Although they make intuitive sense, there is no recent experimental data supporting the use of occlusive dressings taped to the chest. Gauze dressings used in our studies consisted of 4 x 4 inch petrolatum impregnated gauze covered with 4 x 4 inch gauze bandages which were taped to the skin on all four edges. This is similar to a wound dressing on the posterior thorax of a supine patient. Dressings applied were not air-tight.
10 LIMITATIONS Limitations include relatively small numbers used and the assumption that our crossover design was valid to make the most of our small numbers. The incomplete mediastinum of a dog was also used. CONCLUSION An open chest wound dressing with a one-way valve improves pulmonary functioning in the absence of positive pressure ventilation, and functions as well as the standard occlusive gauze dressing when positive pressure ventilation is applied.
11 REFERENCES: Sabiston: Textbook of Surgery, 14 th Edition, p
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
Introduction. Respiration. Chapter 10. Objectives. Objectives. The Respiratory System
 Introduction Respiration Chapter 10 The Respiratory System Provides a means of gas exchange between the environment and the body Plays a role in the regulation of acidbase balance during exercise Objectives
Introduction Respiration Chapter 10 The Respiratory System Provides a means of gas exchange between the environment and the body Plays a role in the regulation of acidbase balance during exercise Objectives
EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES
 GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
Respiration - Human 1
 Respiration - Human 1 At the end of the lectures on respiration you should be able to, 1. Describe events in the respiratory processes 2. Discuss the mechanism of lung ventilation in human 3. Discuss the
Respiration - Human 1 At the end of the lectures on respiration you should be able to, 1. Describe events in the respiratory processes 2. Discuss the mechanism of lung ventilation in human 3. Discuss the
AT Kelly Torso. Directions for Use
 AT Kelly Torso Directions for Use Table of Contents Recommends 4 Items Included 5 Skills Taught 5 Preparing the Manikin for Use 6 Head 6 Lungs 6 Abdominal Thrust 6 Instructions for Use 6 Airway Management
AT Kelly Torso Directions for Use Table of Contents Recommends 4 Items Included 5 Skills Taught 5 Preparing the Manikin for Use 6 Head 6 Lungs 6 Abdominal Thrust 6 Instructions for Use 6 Airway Management
AT Kelly Torso. Directions for Use
 AT Kelly Torso Directions for Use 260-00001 2 Table of Contents Recommends 4 Items Included 5 Skills Taught 5 Preparing the Manikin for Use 6 Head 6 Lungs 6 Abdominal Thrust 6 Instructions for Use 6 Airway
AT Kelly Torso Directions for Use 260-00001 2 Table of Contents Recommends 4 Items Included 5 Skills Taught 5 Preparing the Manikin for Use 6 Head 6 Lungs 6 Abdominal Thrust 6 Instructions for Use 6 Airway
War Surgery Dr. Abdulwahid INTRODUCTION: AIRWAY, BREATHING
 War Surgery Dr. Abdulwahid INTRODUCTION: AIRWAY, BREATHING The aims of war surgery: Save life Avoid infectious complications Save limbs Minimize residual disability The outcome is influenced by: Type of
War Surgery Dr. Abdulwahid INTRODUCTION: AIRWAY, BREATHING The aims of war surgery: Save life Avoid infectious complications Save limbs Minimize residual disability The outcome is influenced by: Type of
VENTILATORS PURPOSE OBJECTIVES
 VENTILATORS PURPOSE To familiarize and acquaint the transfer Paramedic with the skills and knowledge necessary to adequately maintain a ventilator in the interfacility transfer environment. COGNITIVE OBJECTIVES
VENTILATORS PURPOSE To familiarize and acquaint the transfer Paramedic with the skills and knowledge necessary to adequately maintain a ventilator in the interfacility transfer environment. COGNITIVE OBJECTIVES
Respiratory System. Part 2
 Respiratory System Part 2 Respiration Exchange of gases between air and body cells Three steps 1. Ventilation 2. External respiration 3. Internal respiration Ventilation Pulmonary ventilation consists
Respiratory System Part 2 Respiration Exchange of gases between air and body cells Three steps 1. Ventilation 2. External respiration 3. Internal respiration Ventilation Pulmonary ventilation consists
LESSON ASSIGNMENT. After completing this lesson, you should be able to:
 LESSON ASSIGNMENT LESSON 1 Chest Trauma LESSON ASSIGNMENT Paragraphs 1-1 through 1-13. LESSON OBJECTIVES After completing this lesson, you should be able to: 1-1. Identify common signs, common treatment,
LESSON ASSIGNMENT LESSON 1 Chest Trauma LESSON ASSIGNMENT Paragraphs 1-1 through 1-13. LESSON OBJECTIVES After completing this lesson, you should be able to: 1-1. Identify common signs, common treatment,
SimBaby. User Guide.
 EN SimBaby User Guide www.laerdal.com Contents Introduction 4 Items Included 5 System Overview & Setup 6 Features 7 Airway Features 7 Breathing Features 7 Cardiovascular Features 7 Vascular Features 7
EN SimBaby User Guide www.laerdal.com Contents Introduction 4 Items Included 5 System Overview & Setup 6 Features 7 Airway Features 7 Breathing Features 7 Cardiovascular Features 7 Vascular Features 7
Respiratory Physiology Gaseous Exchange
 Respiratory Physiology Gaseous Exchange Session Objectives. What you will cover Basic anatomy of the lung including airways Breathing movements Lung volumes and capacities Compliance and Resistance in
Respiratory Physiology Gaseous Exchange Session Objectives. What you will cover Basic anatomy of the lung including airways Breathing movements Lung volumes and capacities Compliance and Resistance in
Department of Biology Work Sheet Respiratory system,9 class
 I. Name the following : Department of Biology Work Sheet Respiratory system,9 class 1. A muscular sheet separating the thoracic and abdominal cavities. 2. A respiratory tube supported by cartilaginous
I. Name the following : Department of Biology Work Sheet Respiratory system,9 class 1. A muscular sheet separating the thoracic and abdominal cavities. 2. A respiratory tube supported by cartilaginous
Mechanical Ventilation
 Mechanical Ventilation Chapter 4 Mechanical Ventilation Equipment When providing mechanical ventilation for pediatric casualties, it is important to select the appropriately sized bag-valve mask or endotracheal
Mechanical Ventilation Chapter 4 Mechanical Ventilation Equipment When providing mechanical ventilation for pediatric casualties, it is important to select the appropriately sized bag-valve mask or endotracheal
Pulmonary Circulation
 Pulmonary Circulation resin cast of pulmonary arteries resin cast of pulmonary veins Blood Flow to the Lungs Pulmonary Circulation Systemic Circulation Blood supply to the conducting zone provided by the
Pulmonary Circulation resin cast of pulmonary arteries resin cast of pulmonary veins Blood Flow to the Lungs Pulmonary Circulation Systemic Circulation Blood supply to the conducting zone provided by the
April KHALED MOUSA BACHA. Physiology #2. Dr. Nayef AL-Gharaibeh. Pulmonary volumes & capacities
 25 th April Physiology #2 Pulmonary volumes & capacities Dr. Nayef AL-Gharaibeh KHALED MOUSA BACHA We will start this lecture by explaining an important concept from the previous one: Intrapleural pressure
25 th April Physiology #2 Pulmonary volumes & capacities Dr. Nayef AL-Gharaibeh KHALED MOUSA BACHA We will start this lecture by explaining an important concept from the previous one: Intrapleural pressure
The physiological functions of respiration and circulation. Mechanics. exercise 7. Respiratory Volumes. Objectives
 exercise 7 Respiratory System Mechanics Objectives 1. To explain how the respiratory and circulatory systems work together to enable gas exchange among the lungs, blood, and body tissues 2. To define respiration,
exercise 7 Respiratory System Mechanics Objectives 1. To explain how the respiratory and circulatory systems work together to enable gas exchange among the lungs, blood, and body tissues 2. To define respiration,
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo
 Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
4/18/12 MECHANISM OF RESPIRATION. Every Breath You Take. Fun Facts
 Objectives MECHANISM OF RESPIRATION Dr Badri Paudel Explain how the intrapulmonary and intrapleural pressures vary during ventilation and relate these pressure changes to Boyle s law. Define the terms
Objectives MECHANISM OF RESPIRATION Dr Badri Paudel Explain how the intrapulmonary and intrapleural pressures vary during ventilation and relate these pressure changes to Boyle s law. Define the terms
Chest Drains. All Covenant Health Intermediate Care Nursery staff. Needle Aspiration
 Approved by: Chest Drains Gail Cameron Director, Maternal, Neonatal & Child Health Programs Neonatal Nursery Policy & Procedures Manual : April 2013 Next Review April 2016 Dr. Ensenat Medical Director,
Approved by: Chest Drains Gail Cameron Director, Maternal, Neonatal & Child Health Programs Neonatal Nursery Policy & Procedures Manual : April 2013 Next Review April 2016 Dr. Ensenat Medical Director,
6 th Accredited Advanced Mechanical Ventilation Course for Anesthesiologists. Course Test Results for the accreditation of the acquired knowledge
 6 th Accredited Advanced Mechanical Ventilation Course for Anesthesiologists Course Test Results for the accreditation of the acquired knowledge Q. Concerning the mechanics of the newborn s respiratory
6 th Accredited Advanced Mechanical Ventilation Course for Anesthesiologists Course Test Results for the accreditation of the acquired knowledge Q. Concerning the mechanics of the newborn s respiratory
Respiratory System. Prepared by: Dorota Marczuk-Krynicka, MD, PhD
 Respiratory System Prepared by: Dorota Marczuk-Krynicka, MD, PhD Lungs: Ventilation Perfusion Gas Exchange - Diffusion 1. Airways and Airway Resistance (AWR) 2. Mechanics of Breathing and Lung (Elastic)
Respiratory System Prepared by: Dorota Marczuk-Krynicka, MD, PhD Lungs: Ventilation Perfusion Gas Exchange - Diffusion 1. Airways and Airway Resistance (AWR) 2. Mechanics of Breathing and Lung (Elastic)
McHENRY WESTERN LAKE COUNTY EMS SYSTEM FALL 2014 CONTINUING EDUCATION MANDATORY FOR ALL PRIMARY AND PROBATIONARY ALS SYSTEM PROVIDERS.
 McHENRY WESTERN LAKE COUNTY EMS SYSTEM FALL 2014 CONTINUING EDUCATION MANDATORY FOR ALL PRIMARY AND PROBATIONARY ALS SYSTEM PROVIDERS ResQPOD In a cardiac arrest blood flow to the organs stop. Key to survival
McHENRY WESTERN LAKE COUNTY EMS SYSTEM FALL 2014 CONTINUING EDUCATION MANDATORY FOR ALL PRIMARY AND PROBATIONARY ALS SYSTEM PROVIDERS ResQPOD In a cardiac arrest blood flow to the organs stop. Key to survival
25/4/2016. Physiology #01 Respiratory system Nayef Garaibeh Rawan Alwaten
 25/4/2016 Physiology #01 Respiratory system Nayef Garaibeh Rawan Alwaten Respiratory System Introduction: - We breath while we are sleeping, talking, working and resting. - Respiratory diseases are abundant
25/4/2016 Physiology #01 Respiratory system Nayef Garaibeh Rawan Alwaten Respiratory System Introduction: - We breath while we are sleeping, talking, working and resting. - Respiratory diseases are abundant
Physiology Unit 4 RESPIRATORY PHYSIOLOGY
 Physiology Unit 4 RESPIRATORY PHYSIOLOGY In Physiology Today Respiration External respiration ventilation gas exchange Internal respiration cellular respiration gas exchange Respiratory Cycle Inspiration
Physiology Unit 4 RESPIRATORY PHYSIOLOGY In Physiology Today Respiration External respiration ventilation gas exchange Internal respiration cellular respiration gas exchange Respiratory Cycle Inspiration
Medical Instruments in the Developing World
 2.2 Ventilators 2.2.1 Clinical Use and Principles of Operation Many patients in an intensive care and the operating room require the mechanical ventilation of their lungs. All thoracic surgery patients,
2.2 Ventilators 2.2.1 Clinical Use and Principles of Operation Many patients in an intensive care and the operating room require the mechanical ventilation of their lungs. All thoracic surgery patients,
Disclosures. The Pediatric Challenge. Topics for Discussion. Traditional Anesthesia Machine. Tidal Volume = mls/kg 2/13/14
 2/13/14 Disclosures Optimal Ventilation of the Pediatric Patient in the OR Consulting Draeger Medical Jeffrey M. Feldman, MD, MSE Division Chief, General Anesthesia Dept. of Anesthesiology and Critical
2/13/14 Disclosures Optimal Ventilation of the Pediatric Patient in the OR Consulting Draeger Medical Jeffrey M. Feldman, MD, MSE Division Chief, General Anesthesia Dept. of Anesthesiology and Critical
Medical Ventilators. Presented by: Edwin Lim
 Medical Ventilators Presented by: Edwin Lim 1 Presentation Outline Respiration and You Medical Ventilators: Why? How? Current Medical Ventilators The Future 2 The Importance of Oxygen People can survive
Medical Ventilators Presented by: Edwin Lim 1 Presentation Outline Respiration and You Medical Ventilators: Why? How? Current Medical Ventilators The Future 2 The Importance of Oxygen People can survive
Capnography in the Veterinary Technician Toolbox. Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA
 Capnography in the Veterinary Technician Toolbox Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA What are Respiration and Ventilation? Respiration includes all those chemical and physical
Capnography in the Veterinary Technician Toolbox Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA What are Respiration and Ventilation? Respiration includes all those chemical and physical
Respiration (revised 2006) Pulmonary Mechanics
 Pulmonary Mechanics") Respiration (revised 2006) Pulmonary Mechanics PUL 1. Diagram how pleural pressure, alveolar pressure, airflow, and lung volume change during a normal quiet breathing cycle. Identify on the figure the
Respiration (revised 2006) Pulmonary Mechanics PUL 1. Diagram how pleural pressure, alveolar pressure, airflow, and lung volume change during a normal quiet breathing cycle. Identify on the figure the
THE PHYSICAL PROPERTIES OF NORMAL LUNGS
 Thorax (1952), 7, 285. THE PHYSICAL PROPERTIES OF NORMAL LUNGS REMOVED AFTER DEATH BY M. B. McILROY From the Medical Professorial Unit, St. Bartholomew's Hospital, London (RECEIVED FOR PUBLICATION OCTOBER
Thorax (1952), 7, 285. THE PHYSICAL PROPERTIES OF NORMAL LUNGS REMOVED AFTER DEATH BY M. B. McILROY From the Medical Professorial Unit, St. Bartholomew's Hospital, London (RECEIVED FOR PUBLICATION OCTOBER
Airway: the tubes through which air flows between atmosphere and alveoli. Upper airway. Lower airway
 Respiration Yu Yanqin ( 虞燕琴 ), PhD Dept. of fph Physiology Zhejiang University, School of Medicine Respiration Definition: the bodily processes involved in exchange of oxygen (O 2 ) and carbon dioxide
Respiration Yu Yanqin ( 虞燕琴 ), PhD Dept. of fph Physiology Zhejiang University, School of Medicine Respiration Definition: the bodily processes involved in exchange of oxygen (O 2 ) and carbon dioxide
RSPT 1060 OBJECTIVES OBJECTIVES OBJECTIVES EQUATION OF MOTION. MODULE C Applied Physics Lesson #1 - Mechanics. Ventilation vs.
 RSPT 1060 MODULE C Applied Physics Lesson #1 - Mechanics OBJECTIVES At the end of this module, the student should be able to define the terms and abbreviations used in the module. draw & explain the equation
RSPT 1060 MODULE C Applied Physics Lesson #1 - Mechanics OBJECTIVES At the end of this module, the student should be able to define the terms and abbreviations used in the module. draw & explain the equation
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE
 SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: ENDO TRACHEAL SUCTIONING OF THE ADULT PATIENT (suc03) Nursing, Respiratory DATE: REVIEWED: PAGES: 11/82 12/18 1 of 5 RESPONSIBILITY: RN,
SARASOTA MEMORIAL HOSPITAL NURSING PROCEDURE TITLE: ISSUED FOR: ENDO TRACHEAL SUCTIONING OF THE ADULT PATIENT (suc03) Nursing, Respiratory DATE: REVIEWED: PAGES: 11/82 12/18 1 of 5 RESPONSIBILITY: RN,
Respiratory Lecture Test Questions Set 1
 Respiratory Lecture Test Questions Set 1 1. The term "respiration" in its most complete meaning is: a. breathing b. oxygen transport c. carbon dioxide transport d. cellular energy production e. all of
Respiratory Lecture Test Questions Set 1 1. The term "respiration" in its most complete meaning is: a. breathing b. oxygen transport c. carbon dioxide transport d. cellular energy production e. all of
Chapter 16 Respiratory System
 Introduction Chapter 16 Respiratory System The respiratory system consists of tubes that filter incoming air and transport it to alveoli where gases are exchanged. Think pair share: what organs are associated
Introduction Chapter 16 Respiratory System The respiratory system consists of tubes that filter incoming air and transport it to alveoli where gases are exchanged. Think pair share: what organs are associated
Chapter 37: Pulmonary Ventilation. Chad & Angela
 Chapter 37: Pulmonary Ventilation Chad & Angela Respiratory Structures Basic Structures of Respiration Nasal/Oral Cavities Larynx Trachea Bronchi Secondary Bronchi Bronchioles Alveoli Mechanics of Ventilation
Chapter 37: Pulmonary Ventilation Chad & Angela Respiratory Structures Basic Structures of Respiration Nasal/Oral Cavities Larynx Trachea Bronchi Secondary Bronchi Bronchioles Alveoli Mechanics of Ventilation
SPEMS SKILLS PROFICIENCY CRITERIA Paramedic
 SPEMS SKILLS PROFICIENCY CRITERIA Paramedic The following skills are required at the Paramedic Level: 1. King Airway 2. IV 3. Endotracheal Intubation 4. Adult EZ IO 5. Pedi EZ IO 6. Pleural Decompression
SPEMS SKILLS PROFICIENCY CRITERIA Paramedic The following skills are required at the Paramedic Level: 1. King Airway 2. IV 3. Endotracheal Intubation 4. Adult EZ IO 5. Pedi EZ IO 6. Pleural Decompression
COALINGA STATE HOSPITAL. Effective Date: August 31, 2006
 COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION Emergency Procedures POLICY NUMBER: 702 Effective Date: August 31, 2006 SUBJECT: CARDIOPULMONARY RESUSCITATION (CPR) 1. PURPOSE: To provide
COALINGA STATE HOSPITAL NURSING POLICY AND PROCEDURE MANUAL SECTION Emergency Procedures POLICY NUMBER: 702 Effective Date: August 31, 2006 SUBJECT: CARDIOPULMONARY RESUSCITATION (CPR) 1. PURPOSE: To provide
Fabrication of a Nursing Manikin Overlay for Simulation of Chest Drainage Management
 Research Experience for Undergraduates 2014 Milwaukee School of Engineering National Science Foundation Grant June 1- August 8, 2014 Fabrication of a Nursing Manikin Overlay for Simulation of Chest Drainage
Research Experience for Undergraduates 2014 Milwaukee School of Engineering National Science Foundation Grant June 1- August 8, 2014 Fabrication of a Nursing Manikin Overlay for Simulation of Chest Drainage
Understanding Tracheostomy Care
 Understanding Tracheostomy Care Inside this guide: This guide will help you learn how to take care of your tracheostomy (trach). It is important to ask questions. You will be given time to learn. Working
Understanding Tracheostomy Care Inside this guide: This guide will help you learn how to take care of your tracheostomy (trach). It is important to ask questions. You will be given time to learn. Working
Respiratory Physiology 2
 Respiratory Physiology 2 Session Objectives. What you will cover Gaseous Exchange Control of Breathing Rate Your objectives are State the function of support structures and epithelia of the bronchial tree
Respiratory Physiology 2 Session Objectives. What you will cover Gaseous Exchange Control of Breathing Rate Your objectives are State the function of support structures and epithelia of the bronchial tree
Respiratory Pulmonary Ventilation
 Respiratory Pulmonary Ventilation Pulmonary Ventilation Pulmonary ventilation is the act of breathing and the first step in the respiratory process. Pulmonary ventilation brings in air with a new supply
Respiratory Pulmonary Ventilation Pulmonary Ventilation Pulmonary ventilation is the act of breathing and the first step in the respiratory process. Pulmonary ventilation brings in air with a new supply
SimNewB. User Guide.
 EN SimNewB User Guide www.laerdal.com Contents Introduction 4 Items Included & Storage 5 System Overview & Setup 6 Features 7 Airway Features 7 Breathing Features 7 Vascular Features 7 Circulation Features
EN SimNewB User Guide www.laerdal.com Contents Introduction 4 Items Included & Storage 5 System Overview & Setup 6 Features 7 Airway Features 7 Breathing Features 7 Vascular Features 7 Circulation Features
BASIC KNOWLEDGE OF LABORATORY FIRST AID
 BASIC KNOWLEDGE OF LABORATORY FIRST AID RV: 02/02/2015 prevencio@uv.es Page 1 of 7 . General issues to be considered by the rescuer in the event of an accident are described below: - Proceed as follows:
BASIC KNOWLEDGE OF LABORATORY FIRST AID RV: 02/02/2015 prevencio@uv.es Page 1 of 7 . General issues to be considered by the rescuer in the event of an accident are described below: - Proceed as follows:
A V A L A N C H E R E S C U E
 AVALANCHE RESCUE The On-Site Triage And Evacuation Of Avalanche Victims Statistics De Quervain s Mortality Curve 1945 to 1979 and 1979 to 1989 2,611 cases, buried at average 1.06 m After 1 hour 30-40%
AVALANCHE RESCUE The On-Site Triage And Evacuation Of Avalanche Victims Statistics De Quervain s Mortality Curve 1945 to 1979 and 1979 to 1989 2,611 cases, buried at average 1.06 m After 1 hour 30-40%
Hallowell EMC Anesthesia WorkStation Operating Manual
 Hallowell EMC Anesthesia WorkStation Operating Manual PN 000a2770 Anesthesia WorkStation A compact (9" W x 9" D x 15" H), convenient system for use on animals under 7 kg (15 lb.) Hallowell Engineering
Hallowell EMC Anesthesia WorkStation Operating Manual PN 000a2770 Anesthesia WorkStation A compact (9" W x 9" D x 15" H), convenient system for use on animals under 7 kg (15 lb.) Hallowell Engineering
Chapter 4: Ventilation Test Bank MULTIPLE CHOICE
 Instant download and all chapters Test Bank Respiratory Care Anatomy and Physiology Foundations for Clinical Practice 3rd Edition Will Beachey https://testbanklab.com/download/test-bank-respiratory-care-anatomy-physiologyfoundations-clinical-practice-3rd-edition-will-beachey/
Instant download and all chapters Test Bank Respiratory Care Anatomy and Physiology Foundations for Clinical Practice 3rd Edition Will Beachey https://testbanklab.com/download/test-bank-respiratory-care-anatomy-physiologyfoundations-clinical-practice-3rd-edition-will-beachey/
Figure 1. A schematic diagram of the human respiratory system.
 Introduction to Respiration In this experiment, you will investigate various aspects of normal breathing, hyperventilation, rebreathing the effect of changing airway resistance and ways in which to measure
Introduction to Respiration In this experiment, you will investigate various aspects of normal breathing, hyperventilation, rebreathing the effect of changing airway resistance and ways in which to measure
Physiology of the Respiratory System
 Biology 212: Anatomy and Physiology II Physiology of the Respiratory System References: Saladin, KS: Anatomy and Physiology, The Unity of Form and Function 8 th (2018). Required reading before beginning
Biology 212: Anatomy and Physiology II Physiology of the Respiratory System References: Saladin, KS: Anatomy and Physiology, The Unity of Form and Function 8 th (2018). Required reading before beginning
APRV: Moving beyond ARDSnet
 APRV: Moving beyond ARDSnet Matthew Lissauer, MD Associate Professor of Surgery Medical Director, Surgical Critical Care Rutgers, The State University of New Jersey What is APRV? APRV is different from
APRV: Moving beyond ARDSnet Matthew Lissauer, MD Associate Professor of Surgery Medical Director, Surgical Critical Care Rutgers, The State University of New Jersey What is APRV? APRV is different from
Circulatory And Respiration
 Circulatory And Respiration Composition Of Blood Blood Heart 200mmHg 120mmHg Aorta Artery Arteriole 50mmHg Capillary Bed Venule Vein Vena Cava Heart Differences Between Arteries and Veins Veins transport
Circulatory And Respiration Composition Of Blood Blood Heart 200mmHg 120mmHg Aorta Artery Arteriole 50mmHg Capillary Bed Venule Vein Vena Cava Heart Differences Between Arteries and Veins Veins transport
Monitoring, Ventilation & Capnography
 Why do we need to monitor? Monitoring, Ventilation & Capnography Keith Simpson BVSc MRCVS MIET(Electronics) Torquay, Devon. Under anaesthesia animals no longer have the ability to adequately control their
Why do we need to monitor? Monitoring, Ventilation & Capnography Keith Simpson BVSc MRCVS MIET(Electronics) Torquay, Devon. Under anaesthesia animals no longer have the ability to adequately control their
Mechanical Ventilation
 PROCEDURE - Page 1 of 5 Purpose Scope Physician's Order Indications Procedure Mechanical Artificial Ventilation refers to any methods to deliver volumes of gas into a patient's lungs over an extended period
PROCEDURE - Page 1 of 5 Purpose Scope Physician's Order Indications Procedure Mechanical Artificial Ventilation refers to any methods to deliver volumes of gas into a patient's lungs over an extended period
2/28/18. Respiratory System. 1 Copyright 2016 by Elsevier Inc. All rights reserved. Introduction. Anatomy. Physiology. Respiratory System
 Introduction Respiratory System Chapter 28 Respiration: We inhale air, extract oxygen from it, exhale air Cardiovascular and respiratory systems work together Failure of either system: - Disruption of
Introduction Respiratory System Chapter 28 Respiration: We inhale air, extract oxygen from it, exhale air Cardiovascular and respiratory systems work together Failure of either system: - Disruption of
Tactical Emergency Casualty Care (TECC) First Care Provider Guidelines
 First Care Provider Guidelines") Adopted from The Committee for TECC: Current as of June 2016 DIRECT THREAT CARE (DTC) / HOT ZONE GUIDELINES 1. In the presence of a direct threat to life, take definitive action towards mitigating that
Adopted from The Committee for TECC: Current as of June 2016 DIRECT THREAT CARE (DTC) / HOT ZONE GUIDELINES 1. In the presence of a direct threat to life, take definitive action towards mitigating that
Chapter 9 Airway Respirations Metabolism Oxygen Requirements Respiratory Anatomy Respiratory Anatomy Respiratory Anatomy Diaphragm
 1 Chapter 9 Airway 2 Respirations Every cell of the body requires to survive Oxygen must come in and carbon must go out 3 Metabolism Metabolism--Process where the body s cells convert food to Adequate
1 Chapter 9 Airway 2 Respirations Every cell of the body requires to survive Oxygen must come in and carbon must go out 3 Metabolism Metabolism--Process where the body s cells convert food to Adequate
Advanced Ventilator Modes. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine
 Advanced Ventilator Modes Shekhar T. Venkataraman M.D. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Advanced modes Pressure-Regulated
Advanced Ventilator Modes Shekhar T. Venkataraman M.D. Shekhar T. Venkataraman M.D. Professor Critical Care Medicine and Pediatrics University of Pittsburgh School of Medicine Advanced modes Pressure-Regulated
QUICK REFERENCE GUIDE
 cm H O 2 cm H O 2 cm HO 2 PSI cm H O 2 ON OFF UPPER LIMIT LOWER LIMIT UPPER LIMIT LOWER LIMIT LIFE PULSE HIGH-FREQUENCY VENTILATOR QUICK REFERENCE GUIDE 01388-08.11 MONITOR PIP JET VALVE ALARMS READY SILENCE
cm H O 2 cm H O 2 cm HO 2 PSI cm H O 2 ON OFF UPPER LIMIT LOWER LIMIT UPPER LIMIT LOWER LIMIT LIFE PULSE HIGH-FREQUENCY VENTILATOR QUICK REFERENCE GUIDE 01388-08.11 MONITOR PIP JET VALVE ALARMS READY SILENCE
ONLINE DATA SUPPLEMENT. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg
 APPENDIX 1 Appendix 1. Complete respiratory protocol. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg predicted body weight (PBW)) (NEJM 2000; 342
APPENDIX 1 Appendix 1. Complete respiratory protocol. First 24 hours: All patients with ARDS criteria were ventilated during 24 hours with low V T (6-8 ml/kg predicted body weight (PBW)) (NEJM 2000; 342
PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: INSTRUCTOR:
 PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: 1. **Identify and name the filters on the 7200ae. 2. **Explain how each filter is sterilized. 3. **Trace the gas flow through the ventilator
PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: 1. **Identify and name the filters on the 7200ae. 2. **Explain how each filter is sterilized. 3. **Trace the gas flow through the ventilator
Respiratory System Physiology. Dr. Vedat Evren
 Respiratory System Physiology Dr. Vedat Evren Respiration Processes involved in oxygen transport from the atmosphere to the body tissues and the release and transportation of carbon dioxide produced in
Respiratory System Physiology Dr. Vedat Evren Respiration Processes involved in oxygen transport from the atmosphere to the body tissues and the release and transportation of carbon dioxide produced in
Chapter 13 The Respiratory System
 Chapter 13 The Respiratory System by Dr. Jay M. Templin Brooks/Cole - Thomson Learning Atmosphere Tissue cell External respiration Alveoli of lungs 1 Ventilation or gas exchange between the atmosphere
Chapter 13 The Respiratory System by Dr. Jay M. Templin Brooks/Cole - Thomson Learning Atmosphere Tissue cell External respiration Alveoli of lungs 1 Ventilation or gas exchange between the atmosphere
The Respiratory System
 Essentials of Human Anatomy & Physiology Elaine N. Marieb Seventh Edition Chapter 13 The Respiratory System Slides 13.1 13.30 Lecture Slides in PowerPoint by Jerry L. Cook Organs of the Respiratory system
Essentials of Human Anatomy & Physiology Elaine N. Marieb Seventh Edition Chapter 13 The Respiratory System Slides 13.1 13.30 Lecture Slides in PowerPoint by Jerry L. Cook Organs of the Respiratory system
Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams)
") Name Lab Partners Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams) Part 1. Lung Volumes and Capacities Objectives 1. Obtain graphical representation of lung capacities
Name Lab Partners Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams) Part 1. Lung Volumes and Capacities Objectives 1. Obtain graphical representation of lung capacities
The Respiratory System. Medical Terminology
 The Respiratory System Medical Terminology The respiratory system is where gas exchange occurs via respiration; inhalation/exhalation. pick up oxygen from inhaled air expels carbon dioxide and water sinus
The Respiratory System Medical Terminology The respiratory system is where gas exchange occurs via respiration; inhalation/exhalation. pick up oxygen from inhaled air expels carbon dioxide and water sinus
UNIT 9 - RESPIRATORY SYSTEM LECTURE NOTES
 UNIT 9 - RESPIRATORY SYSTEM LECTURE NOTES 9.01 GENERAL FUNCTIONS OF THE RESPIRATORY SYSTEM A. Brings oxygenated air to the alveoli B. Removes air containing carbon dioxide C. Filters, warms, and humidifies
UNIT 9 - RESPIRATORY SYSTEM LECTURE NOTES 9.01 GENERAL FUNCTIONS OF THE RESPIRATORY SYSTEM A. Brings oxygenated air to the alveoli B. Removes air containing carbon dioxide C. Filters, warms, and humidifies
STANDARDIZED PROCEDURE NEONATAL INTUBATION (Neonatal)
") I. Definition This procedure is done in order to establish access to the airway in order to assist ventilation by the use of either endotracheal tube (ET tube) and bag, ET tube and continuous positive
I. Definition This procedure is done in order to establish access to the airway in order to assist ventilation by the use of either endotracheal tube (ET tube) and bag, ET tube and continuous positive
Section 2.9 Decannulation
 Bite- sized training from the GTC Section 2.9 Decannulation This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative. The GTC has developed
Bite- sized training from the GTC Section 2.9 Decannulation This is one of a series of bite- sized chunks of educational material developed by the Global Tracheostomy Collaborative. The GTC has developed
Physiology of Respiration
 Physiology of Respiration External Respiration = pulmonary ventilation breathing involves 2 processes: inspiration expiration Inspiration an active process involves contraction of diaphragm innervated
Physiology of Respiration External Respiration = pulmonary ventilation breathing involves 2 processes: inspiration expiration Inspiration an active process involves contraction of diaphragm innervated
VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL
 VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National
VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National
Initiation and Management of Airway Pressure Release Ventilation (APRV)
") Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Assisting with Insertion. Care of Intraspinal Catheters
 Guidelines included: Assisting with an Insertion Care of Various types of Intraspinal s Care of the Intraspinal Infusion Monitoring Removal of the Short Term Non Assisting with Insertion INR should be
Guidelines included: Assisting with an Insertion Care of Various types of Intraspinal s Care of the Intraspinal Infusion Monitoring Removal of the Short Term Non Assisting with Insertion INR should be
CHAPTER 3: The respiratory system
 CHAPTER 3: The respiratory system Practice questions - text book pages 56-58 1) When the inspiratory muscles contract, which one of the following statements is true? a. the size of the thoracic cavity
CHAPTER 3: The respiratory system Practice questions - text book pages 56-58 1) When the inspiratory muscles contract, which one of the following statements is true? a. the size of the thoracic cavity
Procedure 85 Attaching The Humidifier To The Oxygen Flow Meter Or Regulator. Procedure 86 Administering Oxygen Through A Nasal Cannula
 Chapter 12 Respiratory Procedures Procedure 81 Checking Capillary Refill Procedure 82 Using A Pulse Oximeter Procedure 83 Preparing Wall-Outlet Oxygen Procedure 84 Preparing The Oxygen Cylinder Procedure
Chapter 12 Respiratory Procedures Procedure 81 Checking Capillary Refill Procedure 82 Using A Pulse Oximeter Procedure 83 Preparing Wall-Outlet Oxygen Procedure 84 Preparing The Oxygen Cylinder Procedure
Recitation question # 05
 Recitation and Lab # 05 The goal of this recitations / labs is to review material related to the CV and respiratory lectures for the second test of this course. Info required to answer this recitation
Recitation and Lab # 05 The goal of this recitations / labs is to review material related to the CV and respiratory lectures for the second test of this course. Info required to answer this recitation
Respiratory Physiology
 Respiratory Physiology Background Information: When inspiring, the pleura attached to the internal chest wall is pulled outward as the thoracic cavity expands. The pleural cavity [space between the outer
Respiratory Physiology Background Information: When inspiring, the pleura attached to the internal chest wall is pulled outward as the thoracic cavity expands. The pleural cavity [space between the outer
PROBLEM SET 8. SOLUTIONS April 15, 2004
 Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Introduction to Conventional Ventilation
 Introduction to Conventional Ventilation Dr Julian Eason Consultant Neonatologist Derriford Hospital Mechanics Inspiration diaphragm lowers and thorax expands Negative intrathoracic/intrapleural pressure
Introduction to Conventional Ventilation Dr Julian Eason Consultant Neonatologist Derriford Hospital Mechanics Inspiration diaphragm lowers and thorax expands Negative intrathoracic/intrapleural pressure
HOBIT Trial Checklist
 ED INITIAL IDENTIFICATION AND NOTIFICATION OF HOBIT TRIAL PATIENTS HOBIT eligibility met pending head CT results If patient has pacemaker/aicd/insulin pump/other implantable device, verify that the device
ED INITIAL IDENTIFICATION AND NOTIFICATION OF HOBIT TRIAL PATIENTS HOBIT eligibility met pending head CT results If patient has pacemaker/aicd/insulin pump/other implantable device, verify that the device
Tactical Emergency Casualty Care (TECC)
") Tactical Emergency Casualty Care (TECC) Guidelines For First Care Providers Current as of June 2016 DIRECT THREAT CARE (DTC) / HOT ZONE GUIDELINES 1) In the presence of a direct threat to life, take definitive
Tactical Emergency Casualty Care (TECC) Guidelines For First Care Providers Current as of June 2016 DIRECT THREAT CARE (DTC) / HOT ZONE GUIDELINES 1) In the presence of a direct threat to life, take definitive
Let s talk about Capnography
 Let s talk about Capnography This is one of a series of articles by Keith Simpson BVSc MRCVS MIET (Electronics) discussing the practical aspects of some common monitoring techniques. Capnometry is the
Let s talk about Capnography This is one of a series of articles by Keith Simpson BVSc MRCVS MIET (Electronics) discussing the practical aspects of some common monitoring techniques. Capnometry is the
Module Two. Objectives: Objectives cont. Objectives cont. Objectives cont.
 Transition to the New National EMS Education Standards: EMT-B B to EMT Module Two Objectives: Upon completion, each participant will do the following to a degree of accuracy that meets the Ntl EMS Education
Transition to the New National EMS Education Standards: EMT-B B to EMT Module Two Objectives: Upon completion, each participant will do the following to a degree of accuracy that meets the Ntl EMS Education
Tourniquet Systems Pressure Infusion
 Tourniquet Systems Pressure Infusion VBM Medizintechnik GmbH VBM 1 VBM 2 Summary Tourniquets and Accessories Digital Tourniquets... Compressed Air Tourniquets... Electronic Tourniquets... Application Tourniquets...
Tourniquet Systems Pressure Infusion VBM Medizintechnik GmbH VBM 1 VBM 2 Summary Tourniquets and Accessories Digital Tourniquets... Compressed Air Tourniquets... Electronic Tourniquets... Application Tourniquets...
Tactical Combat Casualty Care Guidelines for All Combatants
 Tactical Combat Casualty Care Guidelines for All Combatants August 2017 (Based on TCCC Guidelines for Medical Personnel 170131) These recommendations are intended to be guidelines only and are not a substitute
Tactical Combat Casualty Care Guidelines for All Combatants August 2017 (Based on TCCC Guidelines for Medical Personnel 170131) These recommendations are intended to be guidelines only and are not a substitute
Proceedings of the World Small Animal Veterinary Association Sydney, Australia 2007
 Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress NURSES SETTING UP FOR ANAESTHESIA HOW TO PLAN FOR A SAFE ANAESTHETIC Sandra Forysth, BVSc DipACVA Institute of
Proceedings of the World Small Animal Sydney, Australia 2007 Hosted by: Next WSAVA Congress NURSES SETTING UP FOR ANAESTHESIA HOW TO PLAN FOR A SAFE ANAESTHETIC Sandra Forysth, BVSc DipACVA Institute of
From First Care Provider Trauma
 From First Care Provider Trauma Trauma presents unique challenges to the rescuer. When trauma happens, time is critical; therefore, it s best to have an easy to follow, validated procedure in place. The
From First Care Provider Trauma Trauma presents unique challenges to the rescuer. When trauma happens, time is critical; therefore, it s best to have an easy to follow, validated procedure in place. The
Endotracheal Suctioning: In Line ETT
 Approved by: Endotracheal Suctioning: In Line ETT Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures
Approved by: Endotracheal Suctioning: In Line ETT Gail Cameron Senior Director Operations, Maternal, Neonatal & Child Health Programs Dr. Paul Byrne Medical Director, Neonatology Neonatal Policy & Procedures
PROBLEM SET 9. SOLUTIONS April 23, 2004
 Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Patient Information for the: Humanitarian Device for use in the Control of Air Leaks
 Patient Information for the: Humanitarian Device for use in the Control of Air Leaks Glossary Airway: The tubes in the lungs that pass air to and from the lung tissue. Anesthesia: Technique to make the
Patient Information for the: Humanitarian Device for use in the Control of Air Leaks Glossary Airway: The tubes in the lungs that pass air to and from the lung tissue. Anesthesia: Technique to make the
Instructions/Procedure for Use of the Speaking Valve
 Instructions/Procedure for Use of the Speaking Valve Notes on the use of the speaking valve for ventilator-dependent and non-ventilator dependent patients The speaking valve is a one-way valve that allows
Instructions/Procedure for Use of the Speaking Valve Notes on the use of the speaking valve for ventilator-dependent and non-ventilator dependent patients The speaking valve is a one-way valve that allows
Lectures on Medical Biophysics Department of Biophysics, Medical Faculty, Masaryk University in Brno. Biophysics of breathing.
 Lectures on Medical Biophysics Department of Biophysics, Medical Faculty, Masaryk University in Brno Biophysics of breathing. Spirometry 1 Lecture outline Mechanisms of gas exchange between organism and
Lectures on Medical Biophysics Department of Biophysics, Medical Faculty, Masaryk University in Brno Biophysics of breathing. Spirometry 1 Lecture outline Mechanisms of gas exchange between organism and
PROBLEM SET 7. Assigned: April 1, 2004 Due: April 9, 2004
 Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
A Liter a Lung Measuring Lung Capacity
 A Liter a Lung Measuring Lung Capacity OBJECTIVE In this investigation, students will compare the actual and expected vital capacities of their classmates. LEVEL Middle Grades Life Science CONNECTIONS
A Liter a Lung Measuring Lung Capacity OBJECTIVE In this investigation, students will compare the actual and expected vital capacities of their classmates. LEVEL Middle Grades Life Science CONNECTIONS
Unit 15 Manual Resuscitators
 15-1 Unit 15 Manual Resuscitators GOAL On completion of this unit, the student should comprehend the proper operation of self-inflating resuscitation bags, flow-inflating resuscitation bags and gas-powered
15-1 Unit 15 Manual Resuscitators GOAL On completion of this unit, the student should comprehend the proper operation of self-inflating resuscitation bags, flow-inflating resuscitation bags and gas-powered
Notes on BIPAP/CPAP. M.Berry Emergency physician St Vincent s Hospital, Sydney
 Notes on BIPAP/CPAP M.Berry Emergency physician St Vincent s Hospital, Sydney 2 DEFINITIONS Non-Invasive Positive Pressure Ventilation (NIPPV) Encompasses both CPAP and BiPAP Offers ventilation support
Notes on BIPAP/CPAP M.Berry Emergency physician St Vincent s Hospital, Sydney 2 DEFINITIONS Non-Invasive Positive Pressure Ventilation (NIPPV) Encompasses both CPAP and BiPAP Offers ventilation support
Understanding Tracheostomy Care for your Child
 Understanding Tracheostomy Care for your Child 2 Inside this guide: This guide will help you learn how to take care of your child s tracheostomy (trach). It is important to ask questions. You will be given
Understanding Tracheostomy Care for your Child 2 Inside this guide: This guide will help you learn how to take care of your child s tracheostomy (trach). It is important to ask questions. You will be given
a personal guide to M A N A G I N G Chest Drainage
 a personal guide to M A N A G I N G Chest Drainage Table of Contents Your personal guide to Managing Chest Drainage is a quick and easy reference to help extend your understanding of chest tube drainage
a personal guide to M A N A G I N G Chest Drainage Table of Contents Your personal guide to Managing Chest Drainage is a quick and easy reference to help extend your understanding of chest tube drainage
Lung Volumes and Capacities
 Lung Volumes and Capacities Normally the volume of air entering the lungs during a single inspiration is approximately equal to the volume leaving on the subsequent expiration and is called the tidal volume.
Lung Volumes and Capacities Normally the volume of air entering the lungs during a single inspiration is approximately equal to the volume leaving on the subsequent expiration and is called the tidal volume.
Guidelines for Care: Management of Patients with a Chest Drainage Unit
 GMHA NURSING SERVICES DEPARTMENT Guidelines for Care: Management of Patients with a Chest Drainage Unit Roseann Apuron, RNC OB, Staff Nurse Training Officer OBJECTIVES: 1. Identify the indications, contraindications,
GMHA NURSING SERVICES DEPARTMENT Guidelines for Care: Management of Patients with a Chest Drainage Unit Roseann Apuron, RNC OB, Staff Nurse Training Officer OBJECTIVES: 1. Identify the indications, contraindications,
Unit II Problem 4 Physiology: Diffusion of Gases and Pulmonary Circulation
 Unit II Problem 4 Physiology: Diffusion of Gases and Pulmonary Circulation - Physical principles of gases: Pressure of a gas is caused by the movement of its molecules against a surface (more concentration
Unit II Problem 4 Physiology: Diffusion of Gases and Pulmonary Circulation - Physical principles of gases: Pressure of a gas is caused by the movement of its molecules against a surface (more concentration