Capnography (ICP) Acknowledgement This training package was created by Leonie Wilton. Please direct any questions to your CSO or Team Leader.
|
|
|
- Anne Park
- 5 years ago
- Views:
Transcription


1 Capnography (ICP) Acknowledgement This training package was created by Leonie Wilton. Please direct any questions to your CSO or Team Leader. Offline Reading Download as PDF Welcome Introduction Basic Physiology & Waveforms Capnography in Cardiac Arrest Capnography in Post-ROSC Management Capnography Application
2 Appendix and FAQs CPG Links & References Summative Assessment Details Download PDF for of ine reading
3 Section 1 of 10 Welcome Welcome to the clinical development package which outlines the use of capnography in cardiac arrest (CA) management and post-rosc care. This package was originally prepared for paramedics. Some additional information has been added to make it more relevant to ICP practice, although it is anticipated much of this will be revision. Evidence-based research indicates capnography can provide clinicians with a sensitive indicator of compression effectiveness and ventilation performance; and this can be used as a tool to guide SAAS clinicians when delivering highperformance CPR. Integration of this monitoring into CA management aligns SAAS CPGs with SA Health Policy Guidelines and best practice models of care. References and hyperlinks are provided should you wish to expand your knowledge. Learning Objectives Review the basic principles of how carbon dioxide is measured, including physiology related to capnography Demonstrate an understanding of the structure of the waveform in capnography Review capnography utility in relation to cardiac arrest management Review capnography utility in relation to post-rosc management
4 Use capnography in accordance with the SAAS paramedic Cardiac Arrest and Post-ROSC Management CPGs (ICP) Overview The training will consist of: a review of the underlying physiology of capnography interpretation of basic waveforms and their clinical significance an outline of capnography utility in CPR and post-rosc management interpretation limitations and treatment implications a summative assessment Successful completion of the online package will require at least 80% correct responses to the 15 MCQ, and must occur prior to attending an OHCA conference. This package (including videos) will take approximately 1 hour to complete.
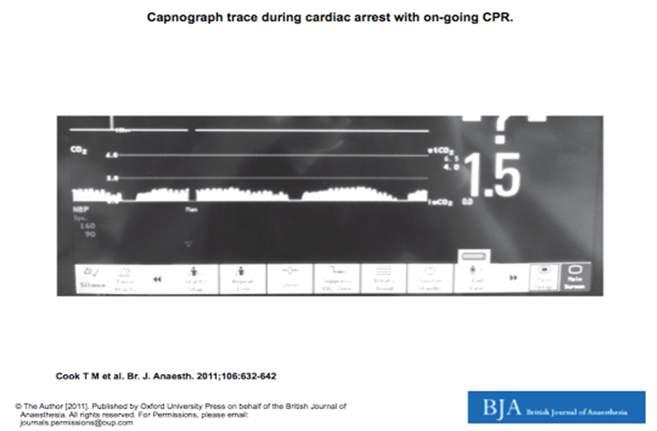
5 Section 2 of 10 Introduction The amount of carbon dioxide (CO 2 ) excreted by the lungs is determined by the amount of pulmonary blood flow and ventilation. Capnography is the monitoring of the concentration or partial pressure of CO 2 in respiratory gases. Traditionally, capnography has been used during anaesthesia and intensive care to confirm and monitor correct ETT placement, equipment circuits and adequacy of ventilation using mainstream or side-stream gas sampling. [10] Capnography provides instantaneous information about: ventilation (how effectively CO 2 is being eliminated by the lungs) perfusion (how effectively CO 2 is being transported through the vascular system) metabolism (how effectively CO 2 is being produced by cellular metabolism).[2] Recent evidence highlights the value of information provided by capnography to monitor the effectiveness of CPR; and hence is the main focus of this CDP. Interpretation of the waveforms outside of cardiac arrest requires a more detailed understanding of the relationship with various pathologies, implications for patient treatment, along with identification of normal variances and false values. The picture below demonstrates the breadth of potential application albeit with a ventilator circuit.
![Correct interpretation of the capnographic curves can only be achieved by comparison with other parameters recorded simultaneously, such as HR, ECG, BP, body temperature and SpO 2 [19].](/docs-images/87/95229386/images/6-0.jpg "This device must be used as a prompt to check the patient and then the equipment to understand why a waveform trend may have changed.")
6 Correct interpretation of the capnographic curves can only be achieved by comparison with other parameters recorded simultaneously, such as HR, ECG, BP, body temperature and SpO 2 [19]. This device must be used as a prompt to check the patient and then the equipment to understand why a waveform trend may have changed. For your awareness, paramedics at this time are only authorised to use capnography in the setting of cardiac arrest and post-rosc management. Main advantages of capnography in CA and post ROSC care: Confirm effectiveness of compressions during CPR Predict and correlate ROSC with other clinical findings Detect decreasing/loss of cardiac output during post-rosc management Assist guiding ventilation to ensure a patient is not hyper or hypo-ventilated.

7 Nb: Paramedics will not be adjusting ventilation on a minute to minute basis according to CO 2 values; rather they will abide by the recommendations in the CPG relevant to that patient and use capnography to detect trends and confirm that ventilation rates are appropriate. For ICPs managing the post-rosc patient, it may be appropriate to cautiously adjust ventilations if CO 2 values are persistently high and the distance to hospital (and patient condition) warrants such intervention. This will be outlined in the ICP post-rosc management CPG. For more information, Capnography.com and capnoacademy.com have some useful information and simulation exercises. The terminology: EtCO 2 refers to maximum Partial pressure of CO 2 at the end of a breath ie end-tidal (about mmhg in a healthy adult and the range for children is not significantly different). This is what we will be measuring. PaCO 2 refers to the Partial pressure of CO 2 in the arterial blood (it is generally 3-5 mmhg higher than EtCO 2 ) and normally in the range mm Hg. Capnogram a plot of EtCO 2 versus time (there are also volume capnograms but time is common in clinical practice). Prediction of PaCO 2 from ETCO 2 is variable (the major limiting factors = blood flow to the lungs and mismatch between ventilation and perfusion); ETCO2 may be
8 misleadingly different in conditions with significant mismatch between ventilation and perfusion. Practice Question Capnography for SAAS paramedics and ICPs is most useful during CA management for: providing feedback about the quality of the seal of the i-gel primarily monitoring ventilation rates and tidal volumes indicating the effectiveness of compressions (including fatigue) during CPR; determining likely ROSC during CPR; and monitoring ventilation rates. diagnosing pulmonary obstructive conditions with 100% sensitivity providing an accurate measure of PaCO 2 to most appropriately direct resuscitative efforts SUBMIT

9 Section 3 of 10 Basic Physiology & Waveforms Physics/ the technology: The first modern capnograph is credited to Karl Fried rich Luft (1937) using infrared technology to measure CO 2 concentration; and is the technologic basis of CO 2 measurement used today. [1] Infrared light is absorbed by gases that have two or more different atoms. Since oxygen has two atoms which are not different it does not absorb infrared waves; whereas carbon dioxide gas has different atoms, it absorbs infrared waves. The more infrared waves that are absorbed the higher the level of CO 2. The amount of CO 2 detected is ultimately converted to a measurement and reflected in the shape and amplitude of the

10 capnogram seen on the monitor display. If you want to know more about the physics, refer to FAQ 7. There are 2 types of configurations available for CO2 measurement by infrared technology: Mainstream analysers contain their IR sensor in an adaptor that is connected in-line with the patient s ventilatory circuit (typically at the hub of the ETT, and it can only be used in intubated patients. Side-stream systems (used by SAAS and most capnographs) have the sensor remote from the patient, making it useful for both intubated and non -intubated patients. The Microstream sample line used by SAAS aspirates a continuous sample of air (about 50 ml/min) from the centre of the lumen of the airway adaptor in expired breath and delivers it to the sensor for analysis.

11 There are a number of factors that can influence the accuracy of readings: In a non-intubated patient, exhaled gases can mix with the ambient air or other gases, diluting the CO 2 concentration and falsely lowering the capnography reading [12]. The tendency for under-reading can occur with small sample volumes, increased dead space and small tidal volumes in paediatric patients Basic physiology and Phases: During capnometry, when a patient inhales air which contains negligible CO 2 (~0.04%) and exhales CO 2 (~4%), a waveform tracing is generated as per the diagrams below. To assist with recall some may consider the normal waveform to resemble the shape of an elephant under a blanket.

12 Phase 1 (dead space ventilation, A-B) represents the beginning of exhalation, where the dead space (area which does not participate in gas exchange and thus contains virtually no CO 2 ) is cleared from the upper airway. Phase II (ascending phase, B-C) represents the rapid rise in carbon dioxide (CO 2 ) concentration in the breath stream as the CO 2 from the alveoli reaches the upper airway (dead space gases mixed with alveolar gases).
13 Phase III (alveolar plateau, C-D) represents the CO 2 concentration reaching a uniform level in the entire breath stream from alveolus to nose. The height and slope of the alveolar plateau is dependent on CO 2 content in the alveoli, which in turn is related to ventilation, cardiac output and most importantly the V/Q relationship. Point D, occurring at the end of the alveolar plateau, represents the maximum CO 2 concentration at the end of the tidal breath and is appropriately named the end-tidal CO 2 (EtCO 2 ). This is the number that appears on the monitor display. (CO 2 evolving from alveoli) Phase IV or sometimes referred to as phase 0 (D-E) represents the inspiratory cycle Dead space: the total is a combination of anatomic (airways leading to the alveoli that do not participate in gas exchange); alveolar (ventilated area in the lung without blood flow) and mechanical (artificial airways including the BVM). Mechanical dead space: Reduction of dead space where possible is particularly relevant for paediatric patients. Extension tubes should never be placed on the patient side of the valve unless absolutely necessary, such as

14 when delivering inline nebulisation to the supine patient requiring assisted ventilation. Whilst previous teaching emphasised the importance of attaching the bacterial /HME filter between the patient and CO 2 sampling line to protect the MRX from aspirated contents via the capnography line, recent technical advice suggests that inbuilt filters (in the sampling line and monitor) may offer adequate protection. The bacterial/ HME (Pall) filter with a dead space of 35 ml should not be used on any patient under 40 kg. This recommendation has recently been endorsed by the clinical governance committee (CGC). Based upon expert advice, it will be at the clinician s discretion to include the HME filter in patients over 40 kg, as the filter within the sampling line along with the filter built into the monitor will afford sufficient protection from contamination. Should the sampling line become contaminated there will be a series of dashes and the line will need to be replaced. The necessity for protecting the BVM from contamination is mitigated by the introduction of disposable BVM units. Oxygen content and ventilation/perfusion (V/Q): Take the average 70 kg patient with a RR of 12 and tidal volume of 500 ml: Normal V (ventilation) is ~ 4 L of air per minute (nearly 2 L is lost to anatomical deadspace). Normal Q (perfusion) is ~ 5 L of blood per minute. So Normal V/Q ratio is ~ 4/5 or 0.8 CO 2 content is in turn dependent on the V/Q ratio of the alveoli.
 eg pulmonary embolus (PE), hypovolaemia, tamponade, shocked patients, cardiac arrest")
15 When ventilation (V) exceeds perfusion : ie V/Q > 0.8 the alveoli contain relatively low PCO 2 there is deadspace in the lungs (eg ventilating unperfused lung area) eg pulmonary embolus (PE), hypovolaemia, tamponade, shocked patients, cardiac arrest When there is a V/Q mismatch caused by poor ventilation (v): the V/Q is < 0.8 the alveoli contain relatively high PCO 2 this is related to blood shunting (eg perfusing unventilated lung area) eg could be due to atelectasis, asthma or an ETT in the mainstream bronchus Ventilation perfusion mismatch can arise from shunting or physiological dead space. In patients who are critically unwell (where there is VQ mismatch), the correlation between EtCO 2 and PaCO 2 is particularly difficult to predict. Practice Question Which part of the capnography waveform represents exhalation?
16 Segments B-C and C-D Segments A-B and B-C Segments B-C; C-D and D-E Segments A-B (latter part) ; B-C and C-D Segments A-B and D-E SUBMIT
17 Section 4 of 10 Capnography in Cardiac Arrest End-tidal CO 2 monitoring during CPR can provide information about the effectiveness of resuscitative efforts that, up until this time, have been unavailable. Any trend changes should prompt the clinician to investigate why a change has occurred, whilst interpreting the information in conjunction with a thorough clinical assessment. It is non-invasive, easy to apply and the theory of its use during CPR is relatively straightforward. During cardiac arrest, when alveolar ventilation and metabolism are essentially constant, EtCO 2 reflects pulmonary blood flow. Therefore, EtCO 2 can be used as a non-invasive gauge of the effectiveness of cardiac compressions. As effective CPR leads to a higher cardiac output, EtCO 2 should rise, reflecting the increase in perfusion. Therefore, EtCO 2 can be used to judge the effectiveness of resuscitative attempts and thus lead to changes in technique that could improve the outcome [1]. Basic principle of directing uses of capnography during CPR [1]: During CPR EtCO 2 levels are low, reflecting the low cardiac output achieved by chest compression. End tidal CO 2 values are associated with compression depth and ventilation rate. Optimising the depth of compressions will increase the amount of CO 2 detected. Ideally, clinicians should see a slow increase in EtCO 2 as perfusion increases through effective chest compressions. Any changes should be promptly investigated and steps taken (where possible) to address the cause.
 and resulting increase in perfusion, leads to a rapid")

18 CO2 in relation to cardiac output: When activity of the heart is restored (ROSC), the dramatic increase in cardiac output (right image above) and resulting increase in perfusion, leads to a rapid increase in EtCO 2. The CO 2 that has accumulated during cardiac arrest is effectively transported to the lungs and exhaled. This process manifests as a sudden rise in EtCO 2 as shown in the representation below [2].

19 Significant correlation between partial pressure of end-tidal-co 2 (EtCO 2 ) and cardiac output that can indicate a return of spontaneous circulation (ROSC) demonstrated in animal and human models [5-9,13] ANZCOR [3] and AHA [21] guidelines for cardiac resuscitation emphasise the importance of continuing chest compressions without interruption until a perfusing rhythm is re-established. Experimental evidence indicates that interruptions in chest compressions are followed by sustained periods of reduced blood flow, which only gradually return to pre-interruption levels. According to an observational study of 145 patients with out of hospital cardiac arrest (OHCA), several seconds may be required after electrical conversion to a potentially perfusing rhythm before effective mechanical contractions and a subsequent rise in EtCO 2 occur [20].
20 High performance CPR indicates that pulse checks need only occur once a non-shockable, organised rhythm appears on the ECG in the charge and check period (2 minutely analysis). A notable rise in waveform capnography suggestive of ROSC may appear at any time during CPR. In this situation, compressions should continue but cardiac drugs which are due should be withheld until after the next charge and check cycle (2 minutely), as these would be detrimental in a patient who has potentially regained a life sustaining rhythm. Resuscitation council recommendations Current ANZCOR (2016), ILCOR, AHA (2010), ERC and Advanced Paediatric Life Support (2016) guidelines advise the usefulness of capnography in adults and children during cardiac arrest resuscitation efforts to indicate the effectiveness of CPR [3,21,22]. EtCO 2 can be used as one marker of cardiac output since a spike in waveform will be detected when the patient goes into ROSC during cycles of CPR. Nevertheless it needs clinical correlation. During a cardiac arrest, the EtCO 2 value (ie in mmhg) should not be used as a guide for ventilation, and clinicians should be wary about using it to guide ventilation in the immediate post resuscitation phase. [ANZCOR ] Low CO 2 in expired breath from a patient under CPR may imply: inadequate cardiac compression or excessive ventilation or both a treatable condition (eg pneumothorax, hypovolaemia, cardiac tamponade, severe aortic stenosis or PE (note it may not be clear what underlying causes are contributing or to what extent); this in conjunction with other information may assist in the clinicians decision making about the appropriateness of mobiling under CPR. [ANZCOR Guideline ]
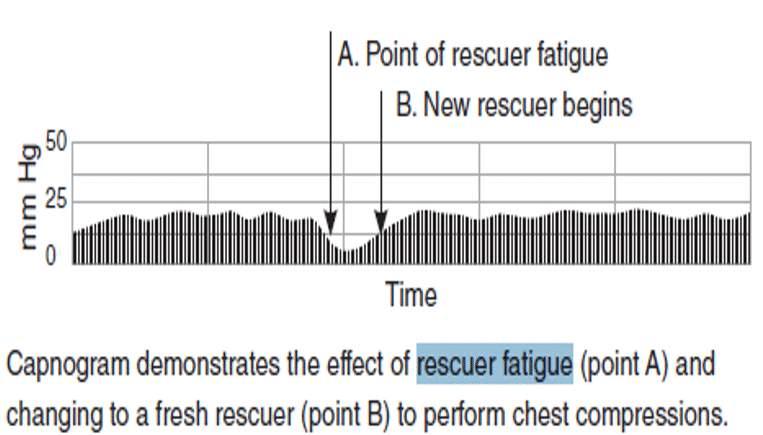
![Utility of Capnography in CPR: CO 2 trend waveform during CPR and indication of fatigue [23] During CPR, decreasing amplitude of the capnogram and lower EtCO 2 values may indicate fatigue,](/docs-images/87/95229386/images/21-0.jpg "characterised by ineffective compressions. Leaning on the chest (providing poor recoil) can compromise venous return; and this may also lead to a decrease in amplitude of the waveform.")
21 Utility of Capnography in CPR: CO 2 trend waveform during CPR and indication of fatigue [23] During CPR, decreasing amplitude of the capnogram and lower EtCO 2 values may indicate fatigue, characterised by ineffective compressions. Leaning on the chest (providing poor recoil) can compromise venous return; and this may also lead to a decrease in amplitude of the waveform. Reevaluation of the clinician s compression technique must occur and if unable to be rectified may prompt an early change of roles if necessary to ensure there is minimal time off chest. An example of re-establishing effective compressions can be seen in the example below with increasing EtCO 2 upon change of operator.
22


23 Capnography is an adjunctive tool; and should never replace a thorough patient assessment and correlation of clinical findings. Success story: 96 minute of CPR with capnography Effective CPR can facilitate adequate cerebral and pulmonary circulation. The pulmonary circulation can be indirectly monitored by capnographic waveform and end tidal carbon dioxide values. The following video illustrates the values of capnography during CPR. YOUTUBE Capnography in Cardiac Arrest
24 Capnography in Cardiac Arrest VIEW ON YOUTUBE Practice question During resuscitative efforts a 55 year old witnessed cardiac arrest with good bystander CPR has been under CPR for 15 minutes and has capnography as outlined following several shocks and adrenaline (the top line is an EtCO 2 level of 45 mm Hg). This low amplitude waveform could best be explained by: Airflow obstruction ie mucous plugging/ bronchospasm
25 Inadequate depth of compressions, excessive ventilations or both Contamination of the sampling line ROSC The patient has just had a can of coke prior to arresting SUBMIT
26 Section 5 of 10 Capnography in Post-ROSC Management Whilst a peak in EtCO 2 level may be one of the earliest signs of ROSC and may occur before return of a palpable pulse or blood pressure, it is one marker and needs to be correlated with clinical findings. Values are higher after an initial asphyxia arrest and with bystander CPR, and these decline over time after cardiac arrest. Whilst studies have shown some correlation between EtCO 2 values during CPR, ROSC rates and mortality, EtCO 2 values should be considered only as part of a multi-modal approach to decision making for prognostication during CPR. [13] Post-ROSC management The cardiac arrest leader can monitor ventilation by primarily observing the waveform trend and correlating this with the numerical respiratory rate displayed in the parameter block (AwRR = airway respiratory rate). ANZCOR [3] advise against focussing on the specific EtCO 2 value in the early post ROSC patient and recommend the clinician: avoid hyperventilation (notable declining height in CO 2 waveform and lowering EtCO 2 ; also evident by increased frequency of capnograms) avoid hypoventilation (significant increasing height in CO 2 waveform and high EtCO 2 ; also evident by reduced frequency of capnograms)
 Baseline")
27 Basic rules for interpretation (just like an algorithm for ECG interpretation): The CO 2 waveform is analysed for five characteristics: Height which depends on the end-tidal CO 2 value Frequency which depends on the respiratory rate Rhythm which depends on the state of the respiratory centre or on the function of the person ventilating (in hospital this would be the ventilator) Baseline which should be zero (unless there is breath stacking or incomplete exhalation) Shape there is only one normal shape The waveforms you will observe on the screen will generally have a 10 second lag (due to sampling time) and the printout will look more elongated since the print out is real time (25mm/second) and the monitor is compressed time. MRX trace with RR 12 and EtCO 2 38 mm Hg; SpO 2 99%; HR 65 bpm.

28 Capnogram Waveforms: The waveforms illustrated below are semi-schematic diagrams depicting their ideal shape. Nonintubated capnography has merit for use in the continuous assessment of patients with poor perfusion or ventilation; however the wave forms may not be quite as precise as intubated capnography due to mixing of gases/ poor seal. Normal This is a normal capnogram (in real time) seen commonly during controlled ventilation or spontaneous ventilation.
29 There is only one normal shape with the following features: A rapid increase (phase II) Nearly horizontal plateau with slight upward sloping phase III Rapid decrease to zero following the peak (inspiration phase IV) Rounded corners Slope of the plateau depends on the condition of the airways and lung tissue End-tidal value is only equivalent to the alveolar CO 2 when a nearly horizontal plateau is seen Disconnection/ Technical fault/ Apnoea: A sudden drop to zero or to a low level almost always indicates a technical disturbance/defect. In the patient under CPR who had a previously detected waveform check for total disconnection, any issue with ventilation equipment (if the patient were intubated this could be a kinked or blocked ET-tube) or the CO 2 sampling line may be defective and need replacing. In spontaneously breathing patients a sudden drop could not only indicate technical fault but the patient has become apnoeic, so it is important in this circumstance to CHECK PATIENT FIRST and then CHECK EQUIPMENT.

30 No waveform flatline Typically due to a misplaced ETT but could also reveal no metabolic activity; no CPR in cardiac arrest; exsanguination or profound shock; equipment failure; airway obstruction. Inability to detect CO 2 in expired breath from a patient receiving adequate chest compression may be due to lack of ventilation. Hypoventilation (bradypnoeic): Trending escalation in CO 2 : There is a progressively increasing end-tidal EtCO 2 values with waves growing taller with each breath/expiration. Base line remains at zero. The shape of the waveform remains normal.
31 There are 4 components responsible for increased EtCO 2 : Increased CO 2 production Increased pulmonary perfusion ie Cardiac output, BP Decreased alveolar ventilation hypoventilation, partial airway obstruction Equipment malfunction i.e. inadequate fresh gas flow A high CO 2 in expired breath implies inadequate ventilation [3]. Whilst treating to EtCO 2 numbers is not advocated due to limited correlation in actual PaCO 2 and EtCO 2 values in the cardiovascularly deranged patient, it is worth considering that hypoventilation is not the cause and should be a prompt to check your ventilation rate and volume. Consider ventilation strategy in the post-rosc patient For ICPs, if the EtCO 2 is persistently high (ie > 45 mmhg) post ROSC and there is a reasonable transport time, cautiously increasing the ventilation rate to reduce the EtCO 2 by 1 mmhg per minute should be considered (as per post-rosc CPG). As a general guide, vary the ventilation rate by no more than 10% to gradually reduce the EtCO 2 towards the upper range of normal.
.")

32 Hypoventilation (hypopnoeic) Note the top waveform is bradypnoeic hypoventilation whereas the bottom reflects hypopnoeic hypoventilation (google images). Hyperventilation: During hyperventilation, the height of the capnogram decreases gradually whilst the baseline remains at zero. Progressive depression of cardiac output or metabolism can also decrease the height of the capnogram.
33 A gradual lowering of the EtCO 2 (normal shape but height of plateau falls) can also be seen in ventilated patients due to: Gradual hyperventilation Lowering body temperature Decreasing perfusion An exponential decrease in CO 2 generally indicates either: Sudden disturbance in lung function Circulatory arrest Sudden decrease in BP Sudden severe hyperventilation This trend should prompt an immediate check of the patient s output (and commence compressions without delay if required). If the output is adequate check the effectiveness of ventilation. In the spontaneously ventilating patient with a persistently low EtCO 2, causes may include hyperventilation secondary to compensation for hypoxia, metabolic acidosis, pain or profound


34 shock. Expiratory problems In general, any airway obstruction limiting expiration can result in an increase in the phase III as well. Depending on the severity of airway obstruction, phase II can also be prolonged. This waveform resembles a shark fin which loses the alveolar plateau. The waveform changes below may be caused by a kinked or blocked airway device; a foreign body; bronchospasm; emphysema and bronchial asthma.
 With a normal RR and TV but with a low")
35 The slope of the phase III is increased, and phase II is prolonged. With response to treatment, there is normalisation of the capnogram. Low end tidal CO 2 Note a normal respiratory rate and plateau but a lower than normal EtCO2 can be observed in ventilated pts who: Are in shock (ie have a PE) With a normal RR and TV but with a low body temperature Having effective CPR performed during cardiac arrest


36 Sudden change in baseline A gradual up-shift in baseline (ie elevated from zero) can result from an increasing dead space, resulting in rebreathing. It could also indicate incomplete exhalation, a calibration error, or the CO 2 absorber is contaminated. Where possible reduce any unnecessary connections which could contribute to increased dead space or check filter for contamination. Summarising basic rules: A useful link is included if you d like to hear about pitfalls.

37 Capnography versus Pulse Oximetrythe measurement of ventilation vs oxygenation: Certainly the oximeter is an excellent method for detecting hypoxia, however it doesn t necessarily aid in the identification of the aetiology. Capnography on the other hand can reveal situations that may lead to hypoxia (ie more rapidly detects airway obstruction and hypoxaemia before the oximeter may reveal desaturation). Note the strip below. The patient has become apnoeic and this is detected well before the changes in oximetry levels are evident. Practice Question Observing a waveform alone only tells you part of the picture, and it is important to correlate this with other findings. Consider the capnogram below with the decreasing amplitude in EtCO 2 observed over a few minutes. Which answer best explains this waveform in a spontaneously breathing patient who is post-rosc:
 & be prepared to start compressions This waveform reflects the")
38 A slight leak in the seal of the i-gel, with dilution of gases leading to decreased EtCO 2 even if no significant evidence of leak pull out the i-gel just in case. Likely impending circulatory arrest if the waveform continues to decline in amplitude correlate clinically (check quality of pulse) & be prepared to start compressions This waveform reflects the different shape seen in a patient monitored with nasal capnography - it is of no concern Sudden hypoventilation of unknown aetiology - continue to observe closely Normal waveform expected as EtCO 2 levels normalise from accumulated levels post cardiac arrest ignore the change in trend SUBMIT

39 Section 6 of 10 Capnography Application Attachment: If the clinician deems the HME bacterial filter is required in grossly soiled airways, it is placed between the SGA (i-gel) and the EtCO 2 sampling line. This configuration will offer additional protection of the sampling line, MRX and BVM from contamination, but is not recommended in patients under 40 kg due to the extra dead space (as discussed in section 2). The EtCO 2 port is located on the left side of the MRX under the pocket flap and can be exposed by pulling down the protective cover; to ensure a firm connection insert and twist clockwise by 90

40 degrees (figure 2). If there are issues with EtCO 2 reading, this is a good place to start to ensure the connection is firm. An EtCO 2 waveform should appear on the MRX (figure 3)

41 Checklist: Back to the basics airway; breathing; circulation (has anything changed and why has it changed?); thoroughly evaluate patient respiratory and cardiovascular status; take appropriate action. Troubleshoot the technology identify kinked or cut tubing; poor attachment with monitor obstruction of capnography detector; disconnection of BVM ventilation; dislodgement or malposition of the advanced airway device (especially true of ETT but can also apply to a SGA & poor seal) Trust the technology it plays a large part in decision making; do not discard the technology simply because it does not match your expectations; never ignore information that does not make sense as it may be the key to the problem; but use it wisely to correlate with other clinical findings
42 Take action gather accurate information to drive clinical decision making and communicate effectively with colleagues. Troubleshooting This entails looking at how the 3 main components (monitor, sampling line and patient) interact. Practice Question You are the cardiac arrest leader and advise the clinician at the airway to connect capnography. What answer does not account for the following waveform: In a patient under CPR no waveform could be due to complete airway obstruction The post-rosc patient who was breathing re-arrested; no CPR in progress
43 In the patient under CPR there is no detectable EtCO2 possibly a result of exsanguination, profound shock or a long down time Even a slight leak in the i-gel will result in an undetectable EtCO2 waveform In a patient receiving adequate CPR this could be due to equipment failure SUBMIT
44 Section 7 of 10 Appendix and FAQs Appendix
45
46 FAQs / interest only 1. Some facts about compression depth and ventilation rate: The measurement of EtCO 2 varies directly with the cardiac output produced by chest compression and has been described in both prehospital [13] and ICU patients [8]. Two prospective, observational studies (EMS and ICU) found an EtCO 2 level <3 mmhg immediately after cardiac arrest, with a higher level generated during cardiac compressions and a mean peak >7.5 mmhg just before return of spontaneous circulation (ROSC) [13]. Another observational study of data collected during human CPR found a positive correlation between the depth of chest compressions and EtCO 2 (10 mm increase in compression depth increased EtCO 2 by 1.4 mmhg), as well as ventilation rate and EtCO 2 (increase of 10 breaths/minute decreased ETCO 2 by 3 mmhg), and confirmed that higher EtCO 2 values during CPR correlate with increased ROSC and survival [2] 2. Can capnography be used as a prognostic indicator some words of caution? ANZCOR has put a higher value on not relying on a single variable (ETCO 2 ) and cut-off value when their usefulness in actual clinical practice, and variability according to the underlying cause of cardiac arrest, has not been established. The aetiology (e.g. asphyxia, PE) of cardiac arrest could affect ETCO 2 values, and there is concern about the accuracy of ETCO 2 values during CPR. ANZCOR recommends against using ETCO 2 cut-off values alone as a mortality predictor, or for the decision to stop a resuscitation attempt (CoSTR 2015, strong recommendation, low-quality evidence). ANZCOR suggests that an ETCO 2 10 mm Hg or greater measured after tracheal intubation or after 20 min of resuscitation, may be a predictor of ROSC (CoSTR 2015, weak recommendation, low-quality evidence). 3. Will SAAS introduce capnography for paramedics outside CA?
47 We are starting with the basics. More training will be required to ensure interpretation and clinical practice is safe and translates to better patient outcomes. 4. Can we use capnography to make decisions about termination? Currently ANZCOR (2016) states it is not presently possible to specify a EtCO 2 which predicts survival or quality of survival and more research is warranted. 5. Recording of capnography on the PCR Documenting in the presenting complaint section would include that capnography was recorded and a positive waveform noted (record value i.e. EtCO 2 25 mmhg stating observation and trends, however interpretation of the value is not required as it may be confounded by a number of variables). Attach the code summary to PCR. 6. How is SAAS measuring the effectiveness of CA management? Cardiac arrest performance meetings are regularly held by CPAPs and any important information derived from these will be conveyed as appropriate in a Quality and Safety Matters newsletter or clinical communications. Collecting data is important to drive future performance and implement positive evidence-based changes. What is the physics behind waveform capnography?
48 Currently, the most common capnography technology used by clinicians is infrared absorption spectroscopy. The basic principle is based on the Beer Lambert Law. Amount of infrared rays absorbed is proportional to the concentration of the infrared absorbing substance. Infrared is absorbed by gases that have two or more different atoms. Oxygen therefore does not absorb infrared waves, whereas CO 2 does

49 CO 2 absorbs infrared light at a specific wave length (4.26 μm).

50 The concentration of CO 2 in a sample of mixed gases can be calculated by infrared absorption spectroscopy, whereby a beam of infra red radiation from a light source can be conducted through a sample of air to a photodetector. The greater the concentration of CO 2 in the sample, the more light is absorbed by the gas, decreasing the intensity of the light that reaches the detector.

51 The difference between the intensity of infrared light absorbed and that which passes through the sample yields a calcu lation of CO 2 concentration. In essence the higher the concentration of CO 2 then the greater the amplitude of the capnograms.
52 Section 8 of 10 CPG Links & References Links to CPGs on SAASNet CPG-029-ICP Cardiac Arrest (Adult) - ICP Draft CPG - Post-ROSC Management Download References REFERENCES.pdf 46.4 KB
53 Section 9 of 10 Summative Assessment Details Successful completion of the online package will require at least 80% correct responses to the 15 MCQs. You are allowed three attempts for the quiz. Please speak to your team leader if you have used up all three attempts. Once you have passed the quiz, you can obtain your certificate of completion by returning to your portal. Go to quiz
54 Section 10 of 10 Download PDF for offline reading Download PDF
Capnography in the Veterinary Technician Toolbox. Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA
 Capnography in the Veterinary Technician Toolbox Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA What are Respiration and Ventilation? Respiration includes all those chemical and physical
Capnography in the Veterinary Technician Toolbox Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA What are Respiration and Ventilation? Respiration includes all those chemical and physical
Let s talk about Capnography
 Let s talk about Capnography This is one of a series of articles by Keith Simpson BVSc MRCVS MIET (Electronics) discussing the practical aspects of some common monitoring techniques. Capnometry is the
Let s talk about Capnography This is one of a series of articles by Keith Simpson BVSc MRCVS MIET (Electronics) discussing the practical aspects of some common monitoring techniques. Capnometry is the
RESPIRATORY PHYSIOLOGY, PHYSICS AND
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Techniques Topic: Respiratory monitoring Date: May 05-07, 2016 Language:
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Techniques Topic: Respiratory monitoring Date: May 05-07, 2016 Language:
Monitoring, Ventilation & Capnography
 Why do we need to monitor? Monitoring, Ventilation & Capnography Keith Simpson BVSc MRCVS MIET(Electronics) Torquay, Devon. Under anaesthesia animals no longer have the ability to adequately control their
Why do we need to monitor? Monitoring, Ventilation & Capnography Keith Simpson BVSc MRCVS MIET(Electronics) Torquay, Devon. Under anaesthesia animals no longer have the ability to adequately control their
Capnography. The Other Vital Sign. 3 rd Edition J. D Urbano, RCP, CRT Capnography The Other Vital Sign 3 rd Edition
 The Other Vital Sign 3 rd Edition Send questions or comments to: J. D Urbano, RCP, CRT BreathSounds jdurbano@breathsounds.org Visit Our Website: http://www.breathsounds.org Join Our Forum: http://www.breathsounds.org/reportroom/
The Other Vital Sign 3 rd Edition Send questions or comments to: J. D Urbano, RCP, CRT BreathSounds jdurbano@breathsounds.org Visit Our Website: http://www.breathsounds.org Join Our Forum: http://www.breathsounds.org/reportroom/
High Performance CPR. Offline Reading Download as PDF. Welcome. Introduction. Physiology of CPR. High Performance CPR. Positioning.
 High Performance CPR Acknowledgement This training package was created by Crystal Harris, Clare Collihole, Joseph Schar, and Jordan Pring. Please direct any questions to your CSO or Team Leader. Offline
High Performance CPR Acknowledgement This training package was created by Crystal Harris, Clare Collihole, Joseph Schar, and Jordan Pring. Please direct any questions to your CSO or Team Leader. Offline
II. Set up the monitor
 I. Introduction Capnography monitors the concentration of CO2 in the respiratory gases, which is a rapid and reliable method to detect life-threatening conditions, such as malposition of endotracheal tubes,
I. Introduction Capnography monitors the concentration of CO2 in the respiratory gases, which is a rapid and reliable method to detect life-threatening conditions, such as malposition of endotracheal tubes,
Chapter 4: Ventilation Test Bank MULTIPLE CHOICE
 Instant download and all chapters Test Bank Respiratory Care Anatomy and Physiology Foundations for Clinical Practice 3rd Edition Will Beachey https://testbanklab.com/download/test-bank-respiratory-care-anatomy-physiologyfoundations-clinical-practice-3rd-edition-will-beachey/
Instant download and all chapters Test Bank Respiratory Care Anatomy and Physiology Foundations for Clinical Practice 3rd Edition Will Beachey https://testbanklab.com/download/test-bank-respiratory-care-anatomy-physiologyfoundations-clinical-practice-3rd-edition-will-beachey/
NOTE: If not used, provider must document reason(s) for deferring mechanical ventilation in a patient with an advanced airway
 for deferring mechanical ventilation in a patient with an advanced airway") APPENDIX: TITLE: Mechanical Ventilator Use REVISED: November 1, 2017 I. Introduction: Mechanical Ventilation is the use of an automated device to deliver positive pressure ventilation to a patient. Proper
APPENDIX: TITLE: Mechanical Ventilator Use REVISED: November 1, 2017 I. Introduction: Mechanical Ventilation is the use of an automated device to deliver positive pressure ventilation to a patient. Proper
The physiological functions of respiration and circulation. Mechanics. exercise 7. Respiratory Volumes. Objectives
 exercise 7 Respiratory System Mechanics Objectives 1. To explain how the respiratory and circulatory systems work together to enable gas exchange among the lungs, blood, and body tissues 2. To define respiration,
exercise 7 Respiratory System Mechanics Objectives 1. To explain how the respiratory and circulatory systems work together to enable gas exchange among the lungs, blood, and body tissues 2. To define respiration,
PICU Resident Self-Study Tutorial The Basic Physics of Oxygen Transport. I was told that there would be no math!
 Physiology of Oxygen Transport PICU Resident Self-Study Tutorial I was told that there would be no math! INTRODUCTION Christopher Carroll, MD Although cells rely on oxygen for aerobic metabolism and viability,
Physiology of Oxygen Transport PICU Resident Self-Study Tutorial I was told that there would be no math! INTRODUCTION Christopher Carroll, MD Although cells rely on oxygen for aerobic metabolism and viability,
CARBON DIOXIDE METABOLISM AND CAPNOGRAPHY
 CARBON DIOXIDE METABOLISM AND CAPNOGRAPHY CARBON DIOXIDE METABOLISM Production Transportation Elimination Carbon Dioxide production CO 2 is the metabolite produced by the utilization by cells of oxygen
CARBON DIOXIDE METABOLISM AND CAPNOGRAPHY CARBON DIOXIDE METABOLISM Production Transportation Elimination Carbon Dioxide production CO 2 is the metabolite produced by the utilization by cells of oxygen
VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL
 VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National
VENTILATION STRATEGIES FOR THE CRITICALLY UNWELL Dr Nick Taylor Visiting Emergency Specialist Teaching Hospital Karapitiya Senior Specialist and Director ED Training Clinical Lecturer, Australian National
Name: Oasis: Questions EPCP. Professional Development: ETCO2 Monitoring
 EPCP Professional Development: ET Monitoring Name: Oasis: Questions ET Questions Package 1) Blood entering the pulmonary circuit from the systemic circuit contains on average mmhg. a) 36 b) 46 c) 4 d)
EPCP Professional Development: ET Monitoring Name: Oasis: Questions ET Questions Package 1) Blood entering the pulmonary circuit from the systemic circuit contains on average mmhg. a) 36 b) 46 c) 4 d)
Standard Operating Procedure
 Standard Operating Procedure SOP ID C04 Version 1.0 Title Approved by Capnography: MobiMed Clinical Effectiveness Group Date Issued 1 st February 2013 Review Date 31 st January 2015 Directorate Clinical
Standard Operating Procedure SOP ID C04 Version 1.0 Title Approved by Capnography: MobiMed Clinical Effectiveness Group Date Issued 1 st February 2013 Review Date 31 st January 2015 Directorate Clinical
McHENRY WESTERN LAKE COUNTY EMS SYSTEM FALL 2014 CONTINUING EDUCATION MANDATORY FOR ALL PRIMARY AND PROBATIONARY ALS SYSTEM PROVIDERS.
 McHENRY WESTERN LAKE COUNTY EMS SYSTEM FALL 2014 CONTINUING EDUCATION MANDATORY FOR ALL PRIMARY AND PROBATIONARY ALS SYSTEM PROVIDERS ResQPOD In a cardiac arrest blood flow to the organs stop. Key to survival
McHENRY WESTERN LAKE COUNTY EMS SYSTEM FALL 2014 CONTINUING EDUCATION MANDATORY FOR ALL PRIMARY AND PROBATIONARY ALS SYSTEM PROVIDERS ResQPOD In a cardiac arrest blood flow to the organs stop. Key to survival
Lung Volumes and Capacities
 Lung Volumes and Capacities Normally the volume of air entering the lungs during a single inspiration is approximately equal to the volume leaving on the subsequent expiration and is called the tidal volume.
Lung Volumes and Capacities Normally the volume of air entering the lungs during a single inspiration is approximately equal to the volume leaving on the subsequent expiration and is called the tidal volume.
VENTILATORS PURPOSE OBJECTIVES
 VENTILATORS PURPOSE To familiarize and acquaint the transfer Paramedic with the skills and knowledge necessary to adequately maintain a ventilator in the interfacility transfer environment. COGNITIVE OBJECTIVES
VENTILATORS PURPOSE To familiarize and acquaint the transfer Paramedic with the skills and knowledge necessary to adequately maintain a ventilator in the interfacility transfer environment. COGNITIVE OBJECTIVES
Virginia Beach EMS. Oxylator EMX. Debra H. Brennaman, RN, MPA, NREMT-P
 Virginia Beach EMS Oxylator EMX Debra H. Brennaman, RN, MPA, NREMT-P Oxylator EMX Overview Patient responsive oxygen powered resuscitation / ventilation device intended to provide emergency ventilatory
Virginia Beach EMS Oxylator EMX Debra H. Brennaman, RN, MPA, NREMT-P Oxylator EMX Overview Patient responsive oxygen powered resuscitation / ventilation device intended to provide emergency ventilatory
Cardiac Arrest General
 Date: November 15, 2012 Page 1 of 5 Cardiac Arrest General This protocol should be followed for all adult cardiac arrests. Medical cardiac arrest patients undergoing attempted resuscitation should not
Date: November 15, 2012 Page 1 of 5 Cardiac Arrest General This protocol should be followed for all adult cardiac arrests. Medical cardiac arrest patients undergoing attempted resuscitation should not
EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES
 GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
GENERAL PROVISIONS: EMS INTER-FACILITY TRANSPORT WITH MECHANICAL VENTILATOR COURSE OBJECTIVES Individuals providing Inter-facility transport with Mechanical Ventilator must have successfully completed
2015 Guidelines Summary HeartSine samaritan PAD Automated External Defibrillators
 2015 Guidelines Summary HeartSine samaritan PAD Automated External Defibrillators This document provides a summary of the 2015 guidelines and how the HeartSine samaritan PAD range of products complies
2015 Guidelines Summary HeartSine samaritan PAD Automated External Defibrillators This document provides a summary of the 2015 guidelines and how the HeartSine samaritan PAD range of products complies
Basics of Mechanical Ventilation. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of Mechanical Ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Overview of topics 1. Goals 2. Settings 3. Modes 4. Advantages and disadvantages
Basics of Mechanical Ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Overview of topics 1. Goals 2. Settings 3. Modes 4. Advantages and disadvantages
High-Functioning EMS CPR Teams. Sally A Taylor - Paramedic Atlantic Partners EMS
 High-Functioning EMS CPR Teams Cardiac Arrest Management Sally A Taylor - Paramedic Atlantic Partners EMS Insanity: Doing the same thing over and over and expecting a different result. John Dryden The
High-Functioning EMS CPR Teams Cardiac Arrest Management Sally A Taylor - Paramedic Atlantic Partners EMS Insanity: Doing the same thing over and over and expecting a different result. John Dryden The
By: Aseel Jamil Al-twaijer. Lec : physical principles of gas exchange
 By: Aseel Jamil Al-twaijer Lec : physical principles of gas exchange Date:30 /10/2017 this lecture is about the exchange of gases between the blood and the alveoli. I might add some external definitions
By: Aseel Jamil Al-twaijer Lec : physical principles of gas exchange Date:30 /10/2017 this lecture is about the exchange of gases between the blood and the alveoli. I might add some external definitions
Respiration (revised 2006) Pulmonary Mechanics
 Pulmonary Mechanics") Respiration (revised 2006) Pulmonary Mechanics PUL 1. Diagram how pleural pressure, alveolar pressure, airflow, and lung volume change during a normal quiet breathing cycle. Identify on the figure the
Respiration (revised 2006) Pulmonary Mechanics PUL 1. Diagram how pleural pressure, alveolar pressure, airflow, and lung volume change during a normal quiet breathing cycle. Identify on the figure the
Initiation and Management of Airway Pressure Release Ventilation (APRV)
") Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES
 INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES") INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams)
") Name Lab Partners Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams) Part 1. Lung Volumes and Capacities Objectives 1. Obtain graphical representation of lung capacities
Name Lab Partners Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams) Part 1. Lung Volumes and Capacities Objectives 1. Obtain graphical representation of lung capacities
Mechanical Ventilation. Mechanical Ventilation is a Drug!!! is a drug. MV: Indications for use. MV as a Drug: Outline. MV: Indications for use
 Mechanical Ventilation is a Drug!!! Mechanical Ventilation is a drug I am an employee of Philips Healthcare Hospital Respiratory Care Group and they help me pay for my kids education Jim Laging, RRT, RCP
Mechanical Ventilation is a Drug!!! Mechanical Ventilation is a drug I am an employee of Philips Healthcare Hospital Respiratory Care Group and they help me pay for my kids education Jim Laging, RRT, RCP
A CO 2 Waveform Simulator For Evaluation and Testing of Respiratory Gas Analyzers
 2011 ROCKY MOUNTAIN NASA SPACE GRANT CONSORTIUM 1 A CO 2 Waveform Simulator For Evaluation and Testing of Respiratory Gas Analyzers Christina Long, and Joseph Orr, Ph.D. Department of Bioengineering, University
2011 ROCKY MOUNTAIN NASA SPACE GRANT CONSORTIUM 1 A CO 2 Waveform Simulator For Evaluation and Testing of Respiratory Gas Analyzers Christina Long, and Joseph Orr, Ph.D. Department of Bioengineering, University
RESPIRATORY PHYSIOLOGY. Anaesthesiology Block 18 (GNK 586) Prof Pierre Fourie
 Prof Pierre Fourie") RESPIRATORY PHYSIOLOGY Anaesthesiology Block 18 (GNK 586) Prof Pierre Fourie Outline Ventilation Diffusion Perfusion Ventilation-Perfusion relationship Work of breathing Control of Ventilation 2 This image
RESPIRATORY PHYSIOLOGY Anaesthesiology Block 18 (GNK 586) Prof Pierre Fourie Outline Ventilation Diffusion Perfusion Ventilation-Perfusion relationship Work of breathing Control of Ventilation 2 This image
RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Pulmonary Function and
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Pulmonary Function and
I Physical Principles of Gas Exchange
 Respiratory Gases Exchange Dr Badri Paudel, M.D. 2 I Physical Principles of Gas Exchange 3 Partial pressure The pressure exerted by each type of gas in a mixture Diffusion of gases through liquids Concentration
Respiratory Gases Exchange Dr Badri Paudel, M.D. 2 I Physical Principles of Gas Exchange 3 Partial pressure The pressure exerted by each type of gas in a mixture Diffusion of gases through liquids Concentration
ALVEOLAR - BLOOD GAS EXCHANGE 1
 ALVEOLAR - BLOOD GAS EXCHANGE 1 Summary: These notes examine the general means by which ventilation is regulated in terrestrial mammals. It then moves on to a discussion of what happens when someone over
ALVEOLAR - BLOOD GAS EXCHANGE 1 Summary: These notes examine the general means by which ventilation is regulated in terrestrial mammals. It then moves on to a discussion of what happens when someone over
Practical considerations in anaesthetising exotic species. By Keith Simpson BVSc MRCVS AMIIE(Electronics).
.") Practical considerations in anaesthetising exotic species By Keith Simpson BVSc MRCVS AMIIE(Electronics). The term exotic species is very broad and can cover anything from a skink to an elephant. For the
Practical considerations in anaesthetising exotic species By Keith Simpson BVSc MRCVS AMIIE(Electronics). The term exotic species is very broad and can cover anything from a skink to an elephant. For the
UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION MUST, AT ALL TIMES, ACCEPT THE ENTIRE CARDIAC OUTPUT
 UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION MUST, AT ALL TIMES, ACCEPT THE ENTIRE CARDIAC OUTPUT UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION
UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION MUST, AT ALL TIMES, ACCEPT THE ENTIRE CARDIAC OUTPUT UNIQUE CHARACTERISTICS OF THE PULMONARY CIRCULATION THE PULMONARY CIRCULATION
Monitoring. Suzie Ward March 2013
 Monitoring Suzie Ward March 2013 Monitoring 1 Oximetry Capnography Oxygen Vapours FRCA Primary Pulse oximetry; how does it work? Is it fast or slow? What are its problems? Graph of light absorption of
Monitoring Suzie Ward March 2013 Monitoring 1 Oximetry Capnography Oxygen Vapours FRCA Primary Pulse oximetry; how does it work? Is it fast or slow? What are its problems? Graph of light absorption of
Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X
 HELICOPTER OPERATING PROCEDURE HOP No: C/12 Issued: May 2011 Page: 1 of 5 Revision No: Original Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X TRIM No: 09/300 Document No: D10/9973 X
HELICOPTER OPERATING PROCEDURE HOP No: C/12 Issued: May 2011 Page: 1 of 5 Revision No: Original Difficult Oxygenation Distribution: Sydney X Illawarra X Orange X TRIM No: 09/300 Document No: D10/9973 X
Using the Lifebox oximeter in the neonatal unit. Tutorial 1 the basics
 Using the Lifebox oximeter in the neonatal unit Tutorial 1 the basics Lifebox 2014. 2011. All rights reserved The Lifebox Pulse Oximeter In this tutorial you will learn about: The function of a pulse oximeter
Using the Lifebox oximeter in the neonatal unit Tutorial 1 the basics Lifebox 2014. 2011. All rights reserved The Lifebox Pulse Oximeter In this tutorial you will learn about: The function of a pulse oximeter
Basic Life Support. Based on UK Resuscitation Guidelines (2010)
") Basic Life Support Based on UK Resuscitation Guidelines (2010) Clinical Skills and Simulation Team With acknowledgements also to Basic Life Support Faculty - SoNMS PowerPoint content last updated 26/05/2015
Basic Life Support Based on UK Resuscitation Guidelines (2010) Clinical Skills and Simulation Team With acknowledgements also to Basic Life Support Faculty - SoNMS PowerPoint content last updated 26/05/2015
DOWNLOAD OR READ : VENTILATION BLOOD FLOW AND DIFFUSION PDF EBOOK EPUB MOBI
 DOWNLOAD OR READ : VENTILATION BLOOD FLOW AND DIFFUSION PDF EBOOK EPUB MOBI Page 1 Page 2 ventilation blood flow and diffusion ventilation blood flow and pdf ventilation blood flow and diffusion Title:
DOWNLOAD OR READ : VENTILATION BLOOD FLOW AND DIFFUSION PDF EBOOK EPUB MOBI Page 1 Page 2 ventilation blood flow and diffusion ventilation blood flow and pdf ventilation blood flow and diffusion Title:
UNDERSTANDING NEONATAL WAVEFORM GRAPHICS. Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services
 UNDERSTANDING NEONATAL WAVEFORM GRAPHICS Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services Disclosures Purpose: To enhance bedside staff s knowledge of ventilation and oxygenation
UNDERSTANDING NEONATAL WAVEFORM GRAPHICS Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services Disclosures Purpose: To enhance bedside staff s knowledge of ventilation and oxygenation
Rodney Shandukani 14/03/2012
 Rodney Shandukani 14/03/2012 OXYGEN THERAPY Aerobic metabolism accounts for 90% of Oxygen consumption by tissues. generates ATP by oxidative phosphorylation. Oxygen cascade: Oxygen exerts a partial pressure,
Rodney Shandukani 14/03/2012 OXYGEN THERAPY Aerobic metabolism accounts for 90% of Oxygen consumption by tissues. generates ATP by oxidative phosphorylation. Oxygen cascade: Oxygen exerts a partial pressure,
 Question 1: Define vital capacity. What is its significance? Vital capacity is the maximum volume of air that can be exhaled after a maximum inspiration. It is about 3.5 4.5 litres in the human body. It
Question 1: Define vital capacity. What is its significance? Vital capacity is the maximum volume of air that can be exhaled after a maximum inspiration. It is about 3.5 4.5 litres in the human body. It
Anesthesia monitoring
 Anesthesia monitoring The aim of this anesthesia monitoring teorhetical material is for veterinary assistant to be able to monitore vital signs and any other changes during anesthesia and fill the parameters
Anesthesia monitoring The aim of this anesthesia monitoring teorhetical material is for veterinary assistant to be able to monitore vital signs and any other changes during anesthesia and fill the parameters
Selecting and Connecting Breathing Systems
 Selecting and Connecting Breathing Year Group: BVSc3 + Document number: CSL_A03 Equipment for this station: Equipment list: Pen Paper Calculator T-piece (in CSL a strip of white tape is around this system)
Selecting and Connecting Breathing Year Group: BVSc3 + Document number: CSL_A03 Equipment for this station: Equipment list: Pen Paper Calculator T-piece (in CSL a strip of white tape is around this system)
UTSW/BioTel EMS System Training Bulletin June 1, 2015 EMS TB Adult CPR Update: Change to Continuous Chest Compressions (CCC)
") UTSW/BioTel EMS System Training Bulletin June 1, 2015 EMS TB 15-005 Adult CPR Update: Change to Continuous Chest Compressions (CCC) 06/01/2015 FINAL-BioTel 1 Purpose To set forth updated ADULT CPR practice
UTSW/BioTel EMS System Training Bulletin June 1, 2015 EMS TB 15-005 Adult CPR Update: Change to Continuous Chest Compressions (CCC) 06/01/2015 FINAL-BioTel 1 Purpose To set forth updated ADULT CPR practice
Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation.
, Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation.") Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation. Paradoxical breathing Hyper-resonance on percussion:
Respiratory Signs: Tachypnea (RR>30/min), Desaturation, Shallow breathing, Use of accessory muscles Breathing sound: Wheezing, Rhonchi, Crepitation. Paradoxical breathing Hyper-resonance on percussion:
excellence in care Procedure Management of patients with difficult oxygenation. For Review Aug 2015
 Difficult Oxygenation HELI.CLI.12 Purpose This procedure describes the processes and procedures for a lung protective strategy in the mechanical ventilation of patients that are difficult to oxygenate
Difficult Oxygenation HELI.CLI.12 Purpose This procedure describes the processes and procedures for a lung protective strategy in the mechanical ventilation of patients that are difficult to oxygenate
Respiratory Physiology. Adeyomoye O.I
 Respiratory Physiology By Adeyomoye O.I Outline Introduction Hypoxia Dyspnea Control of breathing Ventilation/perfusion ratios Respiratory/barometric changes in exercise Intra-pulmonary & intra-pleural
Respiratory Physiology By Adeyomoye O.I Outline Introduction Hypoxia Dyspnea Control of breathing Ventilation/perfusion ratios Respiratory/barometric changes in exercise Intra-pulmonary & intra-pleural
Section Two Diffusion of gases
 Section Two Diffusion of gases Lecture 5: Partial pressure and the composition of gasses in air. Factors affecting diffusion of gases. Ventilation perfusion ratio effect on alveolar gas concentration.
Section Two Diffusion of gases Lecture 5: Partial pressure and the composition of gasses in air. Factors affecting diffusion of gases. Ventilation perfusion ratio effect on alveolar gas concentration.
Lung Volumes and Capacities
 BIOL242 Lung Volumes and Capacities Measurement of lung volumes provides a tool for understanding normal function of the lungs as well as disease states. The breathing cycle is initiated by expansion of
BIOL242 Lung Volumes and Capacities Measurement of lung volumes provides a tool for understanding normal function of the lungs as well as disease states. The breathing cycle is initiated by expansion of
VENTILATION AND PERFUSION IN HEALTH AND DISEASE. Dr.HARIPRASAD VS
 VENTILATION AND PERFUSION IN HEALTH AND DISEASE Dr.HARIPRASAD VS Ventilation Total ventilation - total rate of air flow in and out of the lung during normal tidal breathing. Alveolar ventilation -represents
VENTILATION AND PERFUSION IN HEALTH AND DISEASE Dr.HARIPRASAD VS Ventilation Total ventilation - total rate of air flow in and out of the lung during normal tidal breathing. Alveolar ventilation -represents
Errors in Monitoring. BWH Clinical Conference 10/06/04. Copyright 2004, James H Philip, all rights reserved.
 Errors in Monitoring BWH Clinical Conference 10/06/04 Copyright 2004, James H Philip, all rights reserved. Technology Block 2004 10/06/04 James Philip MD Low flow&closed circuit safety&danger 10/06/04
Errors in Monitoring BWH Clinical Conference 10/06/04 Copyright 2004, James H Philip, all rights reserved. Technology Block 2004 10/06/04 James Philip MD Low flow&closed circuit safety&danger 10/06/04
Basic Life Support Adult
 1/3.4.1 Version 4, 03/2016 Basic Life Support Adult CFR - A EFR Collapse Initiate mobilisation of 3 to 4 practitioners / responders Unresponsive and breathing abnormally or gasping 112 / 999 Go to Primary
1/3.4.1 Version 4, 03/2016 Basic Life Support Adult CFR - A EFR Collapse Initiate mobilisation of 3 to 4 practitioners / responders Unresponsive and breathing abnormally or gasping 112 / 999 Go to Primary
Operating Instructions for Microprocessor Controlled Ventilators
 Page 1 of 5 Operating Instructions for Microprocessor Controlled Ventilators Purpose Audience Scope Physician's Order To provide guidelines for the procedure for the use of microprocessor controlled ventilators.
Page 1 of 5 Operating Instructions for Microprocessor Controlled Ventilators Purpose Audience Scope Physician's Order To provide guidelines for the procedure for the use of microprocessor controlled ventilators.
Mechanical Ventilation
 Mechanical Ventilation Chapter 4 Mechanical Ventilation Equipment When providing mechanical ventilation for pediatric casualties, it is important to select the appropriately sized bag-valve mask or endotracheal
Mechanical Ventilation Chapter 4 Mechanical Ventilation Equipment When providing mechanical ventilation for pediatric casualties, it is important to select the appropriately sized bag-valve mask or endotracheal
Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo
 Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo Link full download: http://testbankcollection.com/download/pilbeams-mechanicalventilation-physiological-and-clinical-applications-5th-edition-test-bank-cairo
Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo Link full download: http://testbankcollection.com/download/pilbeams-mechanicalventilation-physiological-and-clinical-applications-5th-edition-test-bank-cairo
Determination of the Frequency Response of an End Tidal CO2 Analyser
 The ITB Journal Volume 4 Issue 2 Article 5 2003 Determination of the Frequency Response of an End Tidal CO2 Analyser Kabita Shakya Catherine Deegan Fran Hegarty Follow this and additional works at: https://arrow.dit.ie/itbj
The ITB Journal Volume 4 Issue 2 Article 5 2003 Determination of the Frequency Response of an End Tidal CO2 Analyser Kabita Shakya Catherine Deegan Fran Hegarty Follow this and additional works at: https://arrow.dit.ie/itbj
Selecting the Ventilator and the Mode. Chapter 6
 Selecting the Ventilator and the Mode Chapter 6 Criteria for Ventilator Selection Why does the patient need ventilatory support? Does the ventilation problem require a special mode? What therapeutic goals
Selecting the Ventilator and the Mode Chapter 6 Criteria for Ventilator Selection Why does the patient need ventilatory support? Does the ventilation problem require a special mode? What therapeutic goals
PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: INSTRUCTOR:
 PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: 1. **Identify and name the filters on the 7200ae. 2. **Explain how each filter is sterilized. 3. **Trace the gas flow through the ventilator
PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: 1. **Identify and name the filters on the 7200ae. 2. **Explain how each filter is sterilized. 3. **Trace the gas flow through the ventilator
APNOEA AND PRE-OXYGENATION
 APNOEA AND PRE-OXYGENATION Original article by Dr Andrew Biffen, Dr Richard Hughes Torbay Hospital, UK INTRODUCTION The purpose of pre-oxygenation is to increase physiological stores of oxygen in order
APNOEA AND PRE-OXYGENATION Original article by Dr Andrew Biffen, Dr Richard Hughes Torbay Hospital, UK INTRODUCTION The purpose of pre-oxygenation is to increase physiological stores of oxygen in order
Mechanical Ventilation
 PROCEDURE - Page 1 of 5 Purpose Scope Physician's Order Indications Procedure Mechanical Artificial Ventilation refers to any methods to deliver volumes of gas into a patient's lungs over an extended period
PROCEDURE - Page 1 of 5 Purpose Scope Physician's Order Indications Procedure Mechanical Artificial Ventilation refers to any methods to deliver volumes of gas into a patient's lungs over an extended period
Disclosures. The Pediatric Challenge. Topics for Discussion. Traditional Anesthesia Machine. Tidal Volume = mls/kg 2/13/14
 2/13/14 Disclosures Optimal Ventilation of the Pediatric Patient in the OR Consulting Draeger Medical Jeffrey M. Feldman, MD, MSE Division Chief, General Anesthesia Dept. of Anesthesiology and Critical
2/13/14 Disclosures Optimal Ventilation of the Pediatric Patient in the OR Consulting Draeger Medical Jeffrey M. Feldman, MD, MSE Division Chief, General Anesthesia Dept. of Anesthesiology and Critical
bespoke In general health and rehabilitation Breath-by-breath multi-functional respiratory gas analyser In human performance
 Introduction Expired Gas Analysis or indirect calorimetry, can be used to measure ventilation and the fractions of oxygen and carbon dioxide in expired air. From these measurements, the body's oxygen consumption
Introduction Expired Gas Analysis or indirect calorimetry, can be used to measure ventilation and the fractions of oxygen and carbon dioxide in expired air. From these measurements, the body's oxygen consumption
Automatic Transport Ventilator
 Automatic Transport Ventilator David M. Landsberg, MD, FACP, FCCP, EMT-P Luke J. Gasowski, RRT, NPS, ACCS, CCP-C, FP-C Christopher J. Fullagar, MD, FACEP, EMT-P Stan Goettel, MS, EMT-P Author credits /
Automatic Transport Ventilator David M. Landsberg, MD, FACP, FCCP, EMT-P Luke J. Gasowski, RRT, NPS, ACCS, CCP-C, FP-C Christopher J. Fullagar, MD, FACEP, EMT-P Stan Goettel, MS, EMT-P Author credits /
 Introduction Welcome to COMPREHENSIVE BASIC LIFE SUPPORT Course. BLS is the foundation for saving lives after cardiac arrest. You will learn the skills of highquality cardiopulmonary resuscitation (CPR)
Introduction Welcome to COMPREHENSIVE BASIC LIFE SUPPORT Course. BLS is the foundation for saving lives after cardiac arrest. You will learn the skills of highquality cardiopulmonary resuscitation (CPR)
Recitation question # 05
 Recitation and Lab # 05 The goal of this recitations / labs is to review material related to the CV and respiratory lectures for the second test of this course. Info required to answer this recitation
Recitation and Lab # 05 The goal of this recitations / labs is to review material related to the CV and respiratory lectures for the second test of this course. Info required to answer this recitation
Unit II Problem 4 Physiology: Diffusion of Gases and Pulmonary Circulation
 Unit II Problem 4 Physiology: Diffusion of Gases and Pulmonary Circulation - Physical principles of gases: Pressure of a gas is caused by the movement of its molecules against a surface (more concentration
Unit II Problem 4 Physiology: Diffusion of Gases and Pulmonary Circulation - Physical principles of gases: Pressure of a gas is caused by the movement of its molecules against a surface (more concentration
Chapter 9 Airway Respirations Metabolism Oxygen Requirements Respiratory Anatomy Respiratory Anatomy Respiratory Anatomy Diaphragm
 1 Chapter 9 Airway 2 Respirations Every cell of the body requires to survive Oxygen must come in and carbon must go out 3 Metabolism Metabolism--Process where the body s cells convert food to Adequate
1 Chapter 9 Airway 2 Respirations Every cell of the body requires to survive Oxygen must come in and carbon must go out 3 Metabolism Metabolism--Process where the body s cells convert food to Adequate
Figure 1. A schematic diagram of the human respiratory system.
 Introduction to Respiration In this experiment, you will investigate various aspects of normal breathing, hyperventilation, rebreathing the effect of changing airway resistance and ways in which to measure
Introduction to Respiration In this experiment, you will investigate various aspects of normal breathing, hyperventilation, rebreathing the effect of changing airway resistance and ways in which to measure
Stratégie ventilatoire pendant la RCP Pr Jean-Christophe M Richard
 Stratégie ventilatoire pendant la RCP Pr Jean-Christophe M Richard Pôle SAMU 74 Urgence et Réanimation Centre Hospitalier Annecy Genevois CONFLICTS OF INTEREST - Air Liquide Medical Systems (part time)
Stratégie ventilatoire pendant la RCP Pr Jean-Christophe M Richard Pôle SAMU 74 Urgence et Réanimation Centre Hospitalier Annecy Genevois CONFLICTS OF INTEREST - Air Liquide Medical Systems (part time)
VT PLUS HF performance verification of Bunnell Life-Pulse HFJV (High Frequency Jet Ventilator)
") VT PLUS HF performance verification of Bunnell Life-Pulse HFJV (High Frequency Jet Ventilator) VT PLUS HF provides a special mode for evaluating the performance of high frequency ventilators while connected
VT PLUS HF performance verification of Bunnell Life-Pulse HFJV (High Frequency Jet Ventilator) VT PLUS HF provides a special mode for evaluating the performance of high frequency ventilators while connected
Proficiency with Zoll in Manual Mode: There is a new Dashboard screen that you will see on the Zoll while in manual mode
 1 Recognizing a shockable rhythm: Will be discussing the difference between course VF and fine VF and that if you are unsure if it is fine VF or asystole treated as asystole and do not shock Proficiency
1 Recognizing a shockable rhythm: Will be discussing the difference between course VF and fine VF and that if you are unsure if it is fine VF or asystole treated as asystole and do not shock Proficiency
BREATH-BY-BREATH METHOD
 BREATH-BY-BREATH METHOD COR-MAN-0000-005-IN / EN Issue A, Rev. 2 2013-07 INNOISION ApS Skovvænge DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
BREATH-BY-BREATH METHOD COR-MAN-0000-005-IN / EN Issue A, Rev. 2 2013-07 INNOISION ApS Skovvænge DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
PROBLEM SET 9. SOLUTIONS April 23, 2004
 Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Hypoxia Following Rapid Decompression to 18,288 m (60,000 ft) Attributable to Alveolar Hypoventilation
 Attributable to Alveolar Hypoventilation") Hypoxia Following Rapid Decompression to 18,288 m (60,000 ft) Attributable to Alveolar Hypoventilation Desmond M Connolly PhD QinetiQ Aircrew Systems Senior Medical Officer Timothy J D Oyly BSc Amanda
Hypoxia Following Rapid Decompression to 18,288 m (60,000 ft) Attributable to Alveolar Hypoventilation Desmond M Connolly PhD QinetiQ Aircrew Systems Senior Medical Officer Timothy J D Oyly BSc Amanda
CHAPTER 6. Oxygen Transport. Copyright 2008 Thomson Delmar Learning
 CHAPTER 6 Oxygen Transport Normal Blood Gas Value Ranges Table 6-1 OXYGEN TRANSPORT Oxygen Dissolved in the Blood Plasma Dissolve means that the gas maintains its precise molecular structure About.003
CHAPTER 6 Oxygen Transport Normal Blood Gas Value Ranges Table 6-1 OXYGEN TRANSPORT Oxygen Dissolved in the Blood Plasma Dissolve means that the gas maintains its precise molecular structure About.003
Medical Instruments in the Developing World
 2.2 Ventilators 2.2.1 Clinical Use and Principles of Operation Many patients in an intensive care and the operating room require the mechanical ventilation of their lungs. All thoracic surgery patients,
2.2 Ventilators 2.2.1 Clinical Use and Principles of Operation Many patients in an intensive care and the operating room require the mechanical ventilation of their lungs. All thoracic surgery patients,
Exploring the relationship between Heart Rate (HR) and Ventilation Rate (R) in humans.
 and Ventilation Rate (R) in humans.") Exploring the relationship between Heart Rate (HR) and Ventilation Rate (R) in humans. The Research Question In this investigation I will be considering the following general research question: Does increased
Exploring the relationship between Heart Rate (HR) and Ventilation Rate (R) in humans. The Research Question In this investigation I will be considering the following general research question: Does increased
Mechanical Ventilation. Which of the following is true regarding ventilation? Basics of Ventilation
 Mechanical Ventilation Jeffrey L. Wilt, MD, FACP, FCCP Associate Professor of Medicine Michigan State University Associate Program Director MSU-Grand Rapids Internal Medicine Residency Which of the following
Mechanical Ventilation Jeffrey L. Wilt, MD, FACP, FCCP Associate Professor of Medicine Michigan State University Associate Program Director MSU-Grand Rapids Internal Medicine Residency Which of the following
Collin County Community College. Lung Physiology
 Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 9 Respiratory System 1 Lung Physiology Factors affecting Ventillation 1. Airway resistance Flow = Δ P / R Most resistance is encountered
Collin County Community College BIOL. 2402 Anatomy & Physiology WEEK 9 Respiratory System 1 Lung Physiology Factors affecting Ventillation 1. Airway resistance Flow = Δ P / R Most resistance is encountered
Breathing Process: Inhalation
 Airway Chapter 6 Breathing Process: Inhalation Active part of breathing Diaphragm and intercostal muscles contract, allowing the lungs to expand. The decrease in pressure allows lungs to fill with air.
Airway Chapter 6 Breathing Process: Inhalation Active part of breathing Diaphragm and intercostal muscles contract, allowing the lungs to expand. The decrease in pressure allows lungs to fill with air.
Indications for Mechanical Ventilation. Mechanical Ventilation. Indications for Mechanical Ventilation. Modes. Modes: Volume cycled
 Mechanical Ventilation Eric A. Libré, MD VCU School of Medicine Inova Fairfax Hospital and VHC Indications for Mechanical Ventilation Inadequate ventilatory effort Rising pco2 with resp acidosis (7.25)
Mechanical Ventilation Eric A. Libré, MD VCU School of Medicine Inova Fairfax Hospital and VHC Indications for Mechanical Ventilation Inadequate ventilatory effort Rising pco2 with resp acidosis (7.25)
How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital. Synopsis
 How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital Synopsis Definition of an oscillator Historical perspective Differences between HFOV and CMV Determinants
How does HFOV work? John F Mills MBBS, FRACP, M Med Sc, PhD Neonatologist Royal Children s Hospital Synopsis Definition of an oscillator Historical perspective Differences between HFOV and CMV Determinants
AED Plus AL The Best Support For Rescuers
 AED Plus AL-80166 The Best Support For Rescuers AL-80166 CPR Required The latest American Heart Association (AHA) Guidelines issued in 2010, are clear: successful defibrillation requires high-quality CPR
AED Plus AL-80166 The Best Support For Rescuers AL-80166 CPR Required The latest American Heart Association (AHA) Guidelines issued in 2010, are clear: successful defibrillation requires high-quality CPR
AUTOVENT 4000 VENTILATOR
 OVERVIEW AUTOVENT 4000 Only properly trained and approved Escambia County Bureau of Public Safety Paramedics are to use the AutoVent 4000 ventilator manufactured by LSP to transport patients already on
OVERVIEW AUTOVENT 4000 Only properly trained and approved Escambia County Bureau of Public Safety Paramedics are to use the AutoVent 4000 ventilator manufactured by LSP to transport patients already on
Training Presentation. TFD-EMS Ver. 1 09/15
 Training Presentation TFD-EMS Ver. 1 09/15 Agenda ResQCPR System: Definition and Labeling IPR Therapy Physiology of Conventional CPR ResQPOD ITD 16 and Instructions for Use ResQPUMP ACD-CPR Device and
Training Presentation TFD-EMS Ver. 1 09/15 Agenda ResQCPR System: Definition and Labeling IPR Therapy Physiology of Conventional CPR ResQPOD ITD 16 and Instructions for Use ResQPUMP ACD-CPR Device and
3100A Competency Exam
 NAME DATE (Circle the appropriate answer) 3100A Competency Exam 1. Of the following, which best describes the mechanics of ventilation used by the 3100A? a. Active inspiration with passive exhalation b.
NAME DATE (Circle the appropriate answer) 3100A Competency Exam 1. Of the following, which best describes the mechanics of ventilation used by the 3100A? a. Active inspiration with passive exhalation b.
AED Plus. The Best Support For Rescuers
 AED Plus The Best Support For Rescuers CPR Required The latest American Heart Association (AHA) Guidelines, issued in 2010, are clear: successful defibrillation requires high-quality CPR performed at the
AED Plus The Best Support For Rescuers CPR Required The latest American Heart Association (AHA) Guidelines, issued in 2010, are clear: successful defibrillation requires high-quality CPR performed at the
Module Two. Objectives: Objectives cont. Objectives cont. Objectives cont.
 Transition to the New National EMS Education Standards: EMT-B B to EMT Module Two Objectives: Upon completion, each participant will do the following to a degree of accuracy that meets the Ntl EMS Education
Transition to the New National EMS Education Standards: EMT-B B to EMT Module Two Objectives: Upon completion, each participant will do the following to a degree of accuracy that meets the Ntl EMS Education
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo
 Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
Automatic Transport Ventilators. ICU Quality Ventilation on the Street.
 Automatic Transport Ventilators ICU Quality Ventilation on the Street. Kevin Bowden, March 20 th 2014 Ventilator Definition A ventilator is an automatic mechanical device designed to provide all or part
Automatic Transport Ventilators ICU Quality Ventilation on the Street. Kevin Bowden, March 20 th 2014 Ventilator Definition A ventilator is an automatic mechanical device designed to provide all or part
ANZCOR Guideline 6 Compressions
 ANZCOR Guideline 6 Compressions Who does this guideline apply to? Summary This guideline applies to all persons who are unresponsive and not breathing normally. Who is the audience for this guideline?
ANZCOR Guideline 6 Compressions Who does this guideline apply to? Summary This guideline applies to all persons who are unresponsive and not breathing normally. Who is the audience for this guideline?
Respiratory Response to Physiologic Challenges. Evaluation copy
 Respiratory Response to Physiologic Challenges Computer 20 The respiratory cycle of inspiration and expiration is controlled by complex mechanisms involving neurons in the cerebral cortex, brain stem,
Respiratory Response to Physiologic Challenges Computer 20 The respiratory cycle of inspiration and expiration is controlled by complex mechanisms involving neurons in the cerebral cortex, brain stem,
Organis TestChest. Flight Simulator for Intensive Care Clinicians
 Organis TestChest Flight Simulator for Intensive Care Clinicians Organis TestChest Critical Care challenges Training on ventilation modes with simulation is crucial for patient safety The equipment and
Organis TestChest Flight Simulator for Intensive Care Clinicians Organis TestChest Critical Care challenges Training on ventilation modes with simulation is crucial for patient safety The equipment and
 http://www.priory.com/cmol/hfov.htm INTRODUCTION The vast majority of patients who are admitted to an Intensive Care Unit (ICU) will need artificial ventilation (Jones et al 1998). The usual means through
http://www.priory.com/cmol/hfov.htm INTRODUCTION The vast majority of patients who are admitted to an Intensive Care Unit (ICU) will need artificial ventilation (Jones et al 1998). The usual means through
Respiratory physiology II.
 Respiratory physiology II. Learning objectives: 29. Pulmonary gas exchange. 30. Oxygen transport in the blood. 31. Carbon-dioxide transport in the blood. 1 Pulmonary gas exchange The transport mechanism
Respiratory physiology II. Learning objectives: 29. Pulmonary gas exchange. 30. Oxygen transport in the blood. 31. Carbon-dioxide transport in the blood. 1 Pulmonary gas exchange The transport mechanism
Respiratory Medicine. A-A Gradient & Alveolar Gas Equation Laboratory Diagnostics. Alveolar Gas Equation. See online here
 Respiratory Medicine A-A Gradient & Alveolar Gas Equation Laboratory Diagnostics See online here Alveolar gas equation helps to calculate the partial pressure of oxygen in alveoli and A-a gradient is the
Respiratory Medicine A-A Gradient & Alveolar Gas Equation Laboratory Diagnostics See online here Alveolar gas equation helps to calculate the partial pressure of oxygen in alveoli and A-a gradient is the