Susan Blonshine, RRT, RPFT, AE-C, FAARC
|
|
|
- Branden Dean
- 5 years ago
- Views:
Transcription

1 Susan Blonshine, RRT, RPFT, AE-C, FAARC 1
2 The measurement of TLC to distinguish between restrictive and obstructive processes. The evaluation of the pathophysiology of obstructive lung diseases that may produce artifactual results when measured by dilution methods. Measurements requiring repeated trials. AARC Clinical Practice Guideline 2
3 Bronchodilator response Bronchial provocation testing Pre- and post- surgical intervention for UAO 3
4 Plethysmography Terminology Thoracic Gas Volume (TGV) also known as V pant A non-specific term. Volume of air in thorax at time shutter closure. Measured during lung volume measurements to obtain FRC pleth Measured at the end of airway resistance measurements to correct the resistance measurement to the lung volume at which it was measured 4
5 Plethysmography Terminology Functional Residual Capacity (FRC pleth ) Volume of air contained within the thoracic cage measured by plethysmography and corrected to the average end-expiratory lung volume that preceded the shutter closure that measured TGV 5
 sg aw = 1/sR")

6 sr aw sr aw = R aw X V pant Inverse, linear relationship to lung volume sg aw (G aw relative to measured lung volume) sg aw = 1/sR aw or 1/(R aw X V pant ) sg aw is not volume-dependent; can be used to assess change in airway resistance even if lung volume changes. 6

7 Shutter closure at endexpiration Shutter closure during panting 7
8 Lung volumes requires stable resting EELV Shutter closed after stable EELV established, then: FRC to RV to TLC (preferred) or FRC to TLC to RV Rapid panting of Raw raises EELV Shutter closed at end of collection to measure TGV for correcting Raw to sgaw 8
9 Calibration Quality Aspects Test Performance Instrument Patient Test Review Error Recognition Troubleshooting Data Reduction 9
10 Environmental parameters MUST be checked for accuracy including barometric pressure, temperature, and box volume. Devices to calibrate daily: Flow Sensor Mouth pressure Transducer Box pressure Transducer Box leak test (time constant) 10


11 Changes in mouth pressure and box pressure are the primary signals in closed shutter maneuver During expiratory phase, the cheeks can bow outwards if not supported Mouth pressure signal diminished Can produce unusable TGV loops ATS says support with fingertips but flat of palm works better 11

12 Whenever possible, dentures remain Rigid round or oval filter mouthpiece works for some, not all patients Flanged mouthpiece helps maintain air-tight seal during closed shutter maneuver 12
13 Smoking, eating and physical activity Avoid for 1 hour Discontinue IV* Discontinue supplemental oxygen* Withhold bronchodilators* 13
14 Open-door phase Closed door phase Performance criteria Coaching/reassurance Performance assessment Data selection/reporting 14

15 Reassure the patient to relieve anxiety associated with the test or sitting within the cabinet The test will take 3-4 minutes The door can be released at any time from the inside (manufacturer-specific) 15
16 Patient Management Explanation Open-door phase Thoroughly explain the procedure Open shutter- like a small piston Closed shutter- brief, gentle efforts try panting with your hand over your mouth Cheeks must be supported by hands Demonstrate the maneuver Practice with the patient Emphasize relaxing and breathing normally between measurements Door Closed Phase Practice while waiting for thermal stability 30-45s minimum 16
17 Patient Management Closed Shutter Explanation Patient performance criteria Emphasize consistent, brief, gentle efforts between efforts/sec (30 to 60/minute) Relax between efforts pull pause push pause pull pause push in pause out pause in pause out Emphasize this is NOT an MVV or MIP/MEP Provide continuous feedback on performance 17
18 Patient Management Coaching Provide Real time feedback Practice Maneuver Prior Door Closure Practice Maneuver After Door Closure Evaluate and Correct during Testing 18
 Seat in box proceed to open door phase Get patient to relax talk to them")

19 Instrument warmed up, then calibrated LEAVE THE DENTURES IN! (unless they interfere) Seat in box proceed to open door phase Get patient to relax talk to them Explain procedure; practice pant with hand over mouth Adjust mouthpiece height, shouldn t be too low or high Practice mouthpiece and nose clip placement Practice cheek support Close door wait for thermal equilibration (30-60s) 19
20 3 Phases of Lung Volume by Plethysmography Measurement 1. Establish FRC - resting tidal breathing, establish stable baseline (EELV) for 3-10 Breaths. 2. Measure TGV - close shutter at end-expiratory lung volume; brief, gentle pant efforts for 2-3 s 3. Measure VC - open Shutter, exhale to RV then inhale to TLC or inhale to TLC and exhale to RV (minimal effort). Shutter closed 20
21 Shutter typically closed for 2-3s Any coaching of cadence (including metronome) before shutter will typically increase respiratory rate Increasing respiratory rate when obstruction is present will increase EELV Control cadence only after shutter closes 21


22 Often good to allow patient to remove noseclips and come off mouthpiece to rest Opening door can reduce stress, allow nasal O 2 Talk to/assess patient Review results Look at stability of EELV prior to shutter Assess line of best fit of 3-5 breaths; adjust if needed Examine TGV loop too small, too large, unidirectional, slope correct? Reinstruct and resume goal is 3-5 repeatable, linked LVs 22
23 Starting the measurement before thermal equilibration achieved No stable resting end-expiratory lung volume (EELV) during tidal breathing Pant effort unidirectional Pant frequency too fast Pant frequency too slow Pant effort too large Pant effort too small Glottis closing during effort Improper vital capacity maneuver after shutter opens Unlinked lung volumes One shutter closure for both lung volumes and airway resistance 23
24 Temperature Box Pressure Typically s after door sealed wide loops Time 24
25 25
26 Causes: Anxiety Dyspnea Confusion Correction Relaxed tone of voice Guided imagery Minimize time Thorough explanation Good coaching 26
27 Causes: Poor understanding Expectation of airflow Loss of attention to coaching Correction Thorough explanation Practice Good coaching 27
28 The assumption that mouth pressure = alveolar pressure no longer valid at pant frequencies above 90/minute. Mouth pressure will underestimate alveolar pressure resulting in an overestimation of FRC pleth. Causes: Improper coaching Anxiety Dyspnea Confusion Airway resistance measurement Correction Relaxed tone of voice Thorough explanation Practice hand over mouth with coaching of cadence 28
29 FRC Try to keep tidal endexpiratory baseline and shutter volume within 200mL TGV 29
30 Thermal drift causes wider TGV loops making slope assignment more difficult Causes: Failure to follow cadence too slow (< 30/minute) Confusion Correction Relaxed tone of voice Thorough explanation Practice with coaching of cadence 30
31 31
32 Difficult to assign TGV slope. Causes: Confusion Anxiety Weakness Correction Coaching at time of testing Between-effort discussion 32
33 Difficult to assign TGV slope. Causes: Confusion/poor understanding Anxiety Correction Coaching at time of testing Between-effort discussion 33
34 34
35 35
36 Examples: Unlinked to baseline and shutter maneuvers Forcing the exhalation Poor ERV maneuver (too short) Poor IC maneuver (no plateau) Correction Instruct and Coach Demonstrate 36
37 Lung volume measurement 3 phases Stable EELV established Lung volume at or near EELV measured Vital capacity measured ERV to TLC (ATS preferred) or IC to RV Linked means 3 phase are tied to each other (patient doesn t come off mouthpiece until all 3 events have been completed) 37

38 Stable resting EELV (minimum of 3 breaths) No evidence of leaks or drift Panting Frequency should be ~ 1.0 br/sec 30-60/min - no higher than 90/min! Linear, appropriately sized loops 3-5 repeatable efforts (FRC pleth range/mean <5%) 38
39 Delete (deactivate) unacceptable efforts Adjust lines representing EELV, if necessary At least 3 breaths Can ignore last breath if patient reacted to imminent shutter closing Adjust TLC and RV points Adjust slopes on TGV loops, if necessary Check FRC (and RV, TLC) variability 39
40 > 3 acceptable FRCpleth within 5% of the mean (Largest FRC pleth smallest FRC pleth ) <0.05 mean FRC pleth Linked VCs show < 0.15L variability 40

41 Evaluating Tidal Breathing Unstable Tidal Breathing Stable Tidal Breathing 41
42 12 breaths in 10s = 72 b/min.


43 tidal volume ~ 0.2L
44
45 Consider that Inspiratory and Expiratory errors are cumulative and sum with each tidal breath. Example: Low flow range expiratory error: -2% Low flow range inspiratory error: +2% Each tidal breath will show 4% discrepancy in volume *inspiratory volume ~ 4% larger than expiratory volume
46 TGV measurements: The TGV loop should always be linear. The source of error in computerized line fitting is usually electronic noise. The line-of-best-fit should lie along the longitudinal axis of the loop. 46
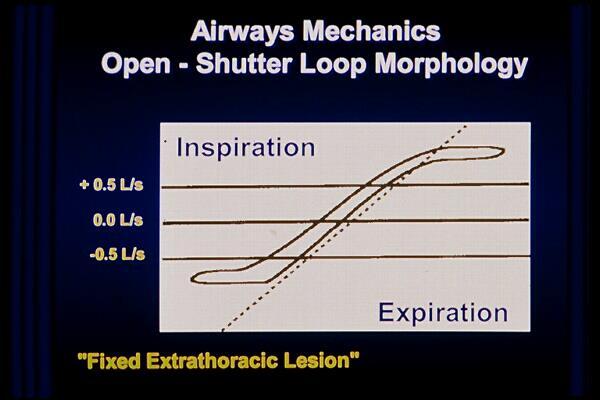
47 Inspiration Mouth Pressure VOLUME TGV = Delta Mouth Pressure / Delta Volume Expiration 47

48 48
49 FRC pleth is mean of all acceptable efforts < 5% variability, (highest lowest)/mean x 100 ERV is mean of ERVs from acceptable linked* vital capacity (ERV then TLC or IC to RV) VC is largest acceptable linked VC * Mean ERV should be close to largest ERV 49
50 RV = mean FRC pleth mean ERV TLC = RV + largest VC alternate TLC calculation: FRC pleth and IC still linked but patient can t perform sustained exhalation TLC = mean of 3 largest FRC pleth + IC sums RV = mean TLC minus largest VC 50
51 Lung Volumes: Perform 3-5 acceptable trials Variability of FRC pleth should be within 5% of the mean. Compare with other methods of volume determination when available 51
52 Volume Acceptability: Compare the VC volume with the FVC volume Alternative Method: IC to TLC after shutter opens TLC = mean of 3 largest FRC pleth + IC sums Use the IC and ERV measurements from the largest acceptable VC maneuver to calculate derived values Compare TLC from different methods Compare VA from DLco and TLC from plethysmography VA should never be higher 52
53 Performance Standard Test Quality Review Lung Volumes Was the pre-shutter EELV stable for 3-10 breaths? Respiratory rate reasonable for patient? EELV (FRC) correctly assigned? Was the shutter closed at the correct level? Start of tidal inspiration (target: within 0.20L of FRC) Effort correct (> 5 cm H20 and < 20 cmh20)? Was the TGV loop bidirectional (inspiratory and expiratory) and closed? Is assigned TGV slope correct? Parallel to TGV loop? RV and TLC points correctly assigned? 53
54 Airway Resistance/Conductance Was the volume small (i.e ml) Was the Pant frequency ~ 1Hz (30-60/m) for TGV Was the Pant frequency ~1.5-2 Hz (90-120/m) for Raw? Is there minimal hysteresis in the open shutter loop? Is the Raw loop measured in the +0.5 to L/sec range? Is the Raw slope parallel with the Raw loop? Are there at least 3 acceptable trials? Has repeatability criteria been met? Is the TGV slope parallel with the TGV loop? 54
 / mean x 100 Is the variability of SVC within 0.15L of the largest SVC? Is the variability for sgaw +.")
55 Variability and Repeatability Is the FRC pleth variability less than 5%? Variability = (max min) / mean x 100 Is the variability of SVC within 0.15L of the largest SVC? Is the variability for sgaw +.01 of mean when below.17 or +.02 of mean when.18 or greater? 55
56 56
57 Airway Resistance Performance and Patient Management 57
")
58 Reassure the patient continually to relieve anxiety associated with the test or sitting within the cabinet The test will take 3-4 minutes The door can be released at any time from the inside (manufacturer specific) 58
59 Patient Management Explanation Open-Door Phase Thoroughly explain the procedure Open shutter- like a small piston Closed shutter- try panting with your hand over your mouth Brief, gentle efforts Cheeks must be supported by hands Demonstrate the maneuver Practice with the patient Emphasize relaxing and breathing normally between measurements Closed-Door Phase Practice while waiting for thermal stability 59
60 Patient Management Explanation Patient performance criteria Small breaths (~50-100ml) Emphasize consistent, gentle efforts between efforts/sec (90 to 120) Relax between efforts Emphasize this is NOT an MVV or MIP/MEP Provide continuous feedback on performance 60
61 Patient Management Coaching Provide real-time feedback Practice maneuver prior to door closure Practice maneuver after door closure Evaluate and correct during testing 61
62 +0.5 LPS -0.5 LPS 62
63 LPS LPS LPS LPS 63
64 +0.5 LPS -0.5 LPS 64
65 Airway Resistance and Conductance Correctly Performed +0.5 LPS -0.5 LPS 65

66 The measurement is generally made a loop intersection with +0.5 and -0.5 L/sec horizontal markers When the loop appears aberrational in the +0.5 and -0.5 L/sec segment, measure through the larger linear portion of the loop. Most importantly, STANDARDIZE the method of measurement in your lab. 66
67 Panting frequency should be ~ breaths/minute open-shutter loops are linear, non-elliptical and closed (or nearly so) intersection of loops with +0.5LPS and -0.5LPS used to construct slope Average of 4-5 acceptable trials sgaw variability is +.01 of mean when below.17 or +.02 of mean when.18 or greater 67
68 68
69 Inspiration L/s 0.0 L/s -0.5 L/s "TOO FAST" Expiration 69
70 Inspiration L/s 0.0 L/s -0.5 L/s Expiration 70
71 Airway Collapse Pattern 71

72 72
PULMONARY FUNCTION TESTING CORE
 PULMONARY FUNCTION TESTING CORE NHLBI Pulmonary Vascular Disease Phenomics Program Funded by the National Heart, Lung, and Blood Institute of the National Institutes of Health with support from the Pulmonary
PULMONARY FUNCTION TESTING CORE NHLBI Pulmonary Vascular Disease Phenomics Program Funded by the National Heart, Lung, and Blood Institute of the National Institutes of Health with support from the Pulmonary
Stikstofuitwas en Heliumdilutie. Eric Derom Universitair Ziekenhuis Gent
 Stikstofuitwas en Heliumdilutie Eric Derom Universitair Ziekenhuis Gent Background Overview Helium-dilution technique Principle of Technique Equipment Procedure and Calculations Quality Control Nitrogen
Stikstofuitwas en Heliumdilutie Eric Derom Universitair Ziekenhuis Gent Background Overview Helium-dilution technique Principle of Technique Equipment Procedure and Calculations Quality Control Nitrogen
Diffusing Capacity: 2017 ATS/ERS Standards for single-breath carbon uptake in the lung. Susan Blonshine RRT, RPFT, FAARC, AE-C
 Diffusing Capacity: 2017 ATS/ERS Standards for single-breath carbon uptake in the lung Susan Blonshine RRT, RPFT, FAARC, AE-C Joint ATS/ERS Taskforce Recent literature reviewed Surveyed current technical
Diffusing Capacity: 2017 ATS/ERS Standards for single-breath carbon uptake in the lung Susan Blonshine RRT, RPFT, FAARC, AE-C Joint ATS/ERS Taskforce Recent literature reviewed Surveyed current technical
Chapter 53: Clinical Center Single-Breath Carbon Monoxide Diffusing Capacity (DLCO) MOP 53.1 Introduction
 MOP 53.1 Introduction") Chapter 53: Clinical Center Single-Breath Carbon Monoxide Diffusing Capacity (DLCO) MOP 53.1 Introduction The DLCO will determine the degree of pulmonary impairment in participants enrolled in the PVDOMICS
Chapter 53: Clinical Center Single-Breath Carbon Monoxide Diffusing Capacity (DLCO) MOP 53.1 Introduction The DLCO will determine the degree of pulmonary impairment in participants enrolled in the PVDOMICS
EasyWarePro Message Numbers
 Application Note CB 06/2016 EasyWarePro Message Numbers Important note: this application note is only valid beginning from EOPC V1.9.0.18 and EOP / Lab V1.9.0.19. Compared to the previous released version
Application Note CB 06/2016 EasyWarePro Message Numbers Important note: this application note is only valid beginning from EOPC V1.9.0.18 and EOP / Lab V1.9.0.19. Compared to the previous released version
EasyWarePro Message Numbers
 Application Note CB 10/2018 EasyWarePro Message Numbers Important note: this application note is only valid beginning from EOPC V1.9.0.18 and EOP / Lab V1.9.0.19. Compared to the previous released version
Application Note CB 10/2018 EasyWarePro Message Numbers Important note: this application note is only valid beginning from EOPC V1.9.0.18 and EOP / Lab V1.9.0.19. Compared to the previous released version
HARD (Gas Dilution) HARDER (Plethysmography) EASIEST (MiniBox+)
 HARDER (Plethysmography) EASIEST (MiniBox+)") Robert Brown, MD Director PFT Lab, Massachusetts General Hospital, Boston, MA Associate Professor of Medicine, Harvard Medical School o o o HARD (Gas Dilution) HARDER (Plethysmography) EASIEST (MiniBox+)
Robert Brown, MD Director PFT Lab, Massachusetts General Hospital, Boston, MA Associate Professor of Medicine, Harvard Medical School o o o HARD (Gas Dilution) HARDER (Plethysmography) EASIEST (MiniBox+)
LAB 7 HUMAN RESPIRATORY LAB. Complete the charts on pgs. 67 and 68 and read directions for using BIOPAC
 66 LAB 7 HUMAN RESPIRATORY LAB Assignments: Due before lab: Quiz: Three Respiratory Interactive Physiology Animations pages 69 73. Complete the charts on pgs. 67 and 68 and read directions for using BIOPAC
66 LAB 7 HUMAN RESPIRATORY LAB Assignments: Due before lab: Quiz: Three Respiratory Interactive Physiology Animations pages 69 73. Complete the charts on pgs. 67 and 68 and read directions for using BIOPAC
Pulmonary Function I (modified by C. S. Tritt, April 10, 2006) Volumes and Capacities
 Volumes and Capacities") I. Introduction Pulmonary Function I (modified by C. S. Tritt, April 10, 2006) Volumes and Capacities The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer
I. Introduction Pulmonary Function I (modified by C. S. Tritt, April 10, 2006) Volumes and Capacities The volume of air a person inhales (inspires) and exhales (expires) can be measured with a spirometer
PROBLEM SET 8. SOLUTIONS April 15, 2004
 Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Breeze Suite Quick Start Operator Manual. An Introduction to Pulmonary Function Testing
 Breeze Suite Quick Start Operator Manual An Introduction to Pulmonary Function Testing The MedGraphics Breeze Suite Quick Start Operator Manual is Part No. 142143-001 Rev A. Caution: Federal (USA) law
Breeze Suite Quick Start Operator Manual An Introduction to Pulmonary Function Testing The MedGraphics Breeze Suite Quick Start Operator Manual is Part No. 142143-001 Rev A. Caution: Federal (USA) law
Body Box 5500 Series Pulmonary Function Testing Systems
 Body Box 5500 Series Pulmonary Function Testing Systems The highest quality of respiratory measurement Plethysmography is used to measure all the thoracic gas volume (VTG) whether in communication with
Body Box 5500 Series Pulmonary Function Testing Systems The highest quality of respiratory measurement Plethysmography is used to measure all the thoracic gas volume (VTG) whether in communication with
RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE
 Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Pulmonary Function and
Course n : Course 3 Title: RESPIRATORY PHYSIOLOGY, PHYSICS AND PATHOLOGY IN RELATION TO ANAESTHESIA AND INTENSIVE CARE Sub-category: Intensive Care for Respiratory Distress Topic: Pulmonary Function and
Cornell Institute for. Biology Teachers. Respirometry Part I: Lung Volumes and Capacities. Lab issue/rev. date: 12/12/96. Title:
 Cornell Institute for Biology Teachers Copyright Cornell Institute for Biology Teachers, 1999. This work may be copied by the original recipient from CIBT to provide copies for users working under the
Cornell Institute for Biology Teachers Copyright Cornell Institute for Biology Teachers, 1999. This work may be copied by the original recipient from CIBT to provide copies for users working under the
Respiration Lab Instructions
 Respiration Lab Instructions This laboratory investigation can be performed in any order. Be sure to read all instructions for each section before performing the experiment. PART 1 STUDENT WET SPIROMETER
Respiration Lab Instructions This laboratory investigation can be performed in any order. Be sure to read all instructions for each section before performing the experiment. PART 1 STUDENT WET SPIROMETER
You Are Really Full of Hot Air!
 You Are Really Full of Hot Air! Student Information Page 5B Activity Introduction: You re just full of hot air! How many times has someone said this to you when they didn t quite believe what you were
You Are Really Full of Hot Air! Student Information Page 5B Activity Introduction: You re just full of hot air! How many times has someone said this to you when they didn t quite believe what you were
Introduction. Respiration. Chapter 10. Objectives. Objectives. The Respiratory System
 Introduction Respiration Chapter 10 The Respiratory System Provides a means of gas exchange between the environment and the body Plays a role in the regulation of acidbase balance during exercise Objectives
Introduction Respiration Chapter 10 The Respiratory System Provides a means of gas exchange between the environment and the body Plays a role in the regulation of acidbase balance during exercise Objectives
Part 1: Inspiratory and expiratory pressures
 BIOEN 327 Autumn 2013 Experimental procedures Throughout these experiments, record in your notebook the purpose of the experiments, the methods you used, and the results. Where possible, make predictions
BIOEN 327 Autumn 2013 Experimental procedures Throughout these experiments, record in your notebook the purpose of the experiments, the methods you used, and the results. Where possible, make predictions
Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams)
") Name Lab Partners Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams) Part 1. Lung Volumes and Capacities Objectives 1. Obtain graphical representation of lung capacities
Name Lab Partners Lab 3. The Respiratory System (designed by Heather E. M. Liwanag with T.M. Williams) Part 1. Lung Volumes and Capacities Objectives 1. Obtain graphical representation of lung capacities
For more information about how to cite these materials visit
 Author(s): Louis D Alecy, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Author(s): Louis D Alecy, 2009 License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Non-commercial Share Alike 3.0 License: http://creativecommons.org/licenses/by-nc-sa/3.0/
Lung Volumes and Capacities
 Lung Volumes and Capacities Experiment 19 Measurement of lung volumes provides a tool for understanding normal function of the lungs as well as disease states. The breathing cycle is initiated by expansion
Lung Volumes and Capacities Experiment 19 Measurement of lung volumes provides a tool for understanding normal function of the lungs as well as disease states. The breathing cycle is initiated by expansion
Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo
 Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo Link full download: http://testbankcollection.com/download/pilbeams-mechanicalventilation-physiological-and-clinical-applications-5th-edition-test-bank-cairo
Completed downloadable Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 5th Edition by Cairo Link full download: http://testbankcollection.com/download/pilbeams-mechanicalventilation-physiological-and-clinical-applications-5th-edition-test-bank-cairo
Respiratory system & exercise. Dr. Rehab F Gwada
 Respiratory system & exercise Dr. Rehab F Gwada Objectives of lecture Outline the major anatomical components & important functions of the respiratory system. Describe the mechanics of ventilation. List
Respiratory system & exercise Dr. Rehab F Gwada Objectives of lecture Outline the major anatomical components & important functions of the respiratory system. Describe the mechanics of ventilation. List
Respiratory Physiology
 Respiratory Physiology Background Information: When inspiring, the pleura attached to the internal chest wall is pulled outward as the thoracic cavity expands. The pleural cavity [space between the outer
Respiratory Physiology Background Information: When inspiring, the pleura attached to the internal chest wall is pulled outward as the thoracic cavity expands. The pleural cavity [space between the outer
Chapter 37: Pulmonary Ventilation. Chad & Angela
 Chapter 37: Pulmonary Ventilation Chad & Angela Respiratory Structures Basic Structures of Respiration Nasal/Oral Cavities Larynx Trachea Bronchi Secondary Bronchi Bronchioles Alveoli Mechanics of Ventilation
Chapter 37: Pulmonary Ventilation Chad & Angela Respiratory Structures Basic Structures of Respiration Nasal/Oral Cavities Larynx Trachea Bronchi Secondary Bronchi Bronchioles Alveoli Mechanics of Ventilation
Restrictive and Obstructive Airway Diseases
 iworx Physiology Lab Experiment Experiment HS-8-1 Restrictive and Obstructive Airway Diseases Note: The lab presented here is intended for evaluation purposes only. iworx users should refer to the User
iworx Physiology Lab Experiment Experiment HS-8-1 Restrictive and Obstructive Airway Diseases Note: The lab presented here is intended for evaluation purposes only. iworx users should refer to the User
Physiology of the Respiratory System
 Biology 212: Anatomy and Physiology II Physiology of the Respiratory System References: Saladin, KS: Anatomy and Physiology, The Unity of Form and Function 8 th (2018). Required reading before beginning
Biology 212: Anatomy and Physiology II Physiology of the Respiratory System References: Saladin, KS: Anatomy and Physiology, The Unity of Form and Function 8 th (2018). Required reading before beginning
PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: INSTRUCTOR:
 PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: 1. **Identify and name the filters on the 7200ae. 2. **Explain how each filter is sterilized. 3. **Trace the gas flow through the ventilator
PERFORMANCE EVALUATION #34 NAME: 7200 Ventilator Set Up DATE: 1. **Identify and name the filters on the 7200ae. 2. **Explain how each filter is sterilized. 3. **Trace the gas flow through the ventilator
Fashionable, don t you think?
 Fashionable, don t you think? 1. Passageway 2. Structure 3. Passageway 4. What is the name of the structure labeled with # 9 in the model at left? 5. What is the name of the structure labeled with # 11
Fashionable, don t you think? 1. Passageway 2. Structure 3. Passageway 4. What is the name of the structure labeled with # 9 in the model at left? 5. What is the name of the structure labeled with # 11
How to Obtain a Good Spirometry Test Result
 How to obtain a good spirometry test? The spirometry technician is the single most important component in obtaining a good or valid spirometry test result. The technician must be able to explain, demonstrate,
How to obtain a good spirometry test? The spirometry technician is the single most important component in obtaining a good or valid spirometry test result. The technician must be able to explain, demonstrate,
Lesson 12 New Procedure PULMONARY FUNCTION I
 Physiology Lessons for use with the Biopac Student Lab Lesson 12 New Procedure PULMONARY FUNCTION I Volumes and Capacities For Windows 98SE, Me, 2000 Pro, XP or Mac OS X 10.3-10.4 Richard Pflanzer, Ph.D.
Physiology Lessons for use with the Biopac Student Lab Lesson 12 New Procedure PULMONARY FUNCTION I Volumes and Capacities For Windows 98SE, Me, 2000 Pro, XP or Mac OS X 10.3-10.4 Richard Pflanzer, Ph.D.
Activity 2: Examining the Effect of Changing Airway Resistance on Respiratory Volumes
 1 BGYC34 PhysioEx Lab 7 Respiratory Systems Mechanics Marking Scheme Part 1 Complete PhysioEx lab #7. Hand-in all of the pages associated with the lab. Note that there are 5 activities to be completed.
1 BGYC34 PhysioEx Lab 7 Respiratory Systems Mechanics Marking Scheme Part 1 Complete PhysioEx lab #7. Hand-in all of the pages associated with the lab. Note that there are 5 activities to be completed.
HELIUM DILUTION TECHNIQUE
 HELIUM DILUTION TECHNIQUE 21.10.2016 Kodati Rakesh Senior Resident Pulmonary medicine History Indications & contraindications Principle Apparatus Procedure & calculation Drawbacks Miscellaneous (single
HELIUM DILUTION TECHNIQUE 21.10.2016 Kodati Rakesh Senior Resident Pulmonary medicine History Indications & contraindications Principle Apparatus Procedure & calculation Drawbacks Miscellaneous (single
The physiological functions of respiration and circulation. Mechanics. exercise 7. Respiratory Volumes. Objectives
 exercise 7 Respiratory System Mechanics Objectives 1. To explain how the respiratory and circulatory systems work together to enable gas exchange among the lungs, blood, and body tissues 2. To define respiration,
exercise 7 Respiratory System Mechanics Objectives 1. To explain how the respiratory and circulatory systems work together to enable gas exchange among the lungs, blood, and body tissues 2. To define respiration,
April KHALED MOUSA BACHA. Physiology #2. Dr. Nayef AL-Gharaibeh. Pulmonary volumes & capacities
 25 th April Physiology #2 Pulmonary volumes & capacities Dr. Nayef AL-Gharaibeh KHALED MOUSA BACHA We will start this lecture by explaining an important concept from the previous one: Intrapleural pressure
25 th April Physiology #2 Pulmonary volumes & capacities Dr. Nayef AL-Gharaibeh KHALED MOUSA BACHA We will start this lecture by explaining an important concept from the previous one: Intrapleural pressure
LAB 3: RESPIRATORY MECHANICS
 BIOEN 327 Autumn 2012 LAB 3: RESPIRATORY MECHANICS Pressures throughout the cardiovascular system are important for the health of the body and of the system itself. Today we explore pulmonary pressures
BIOEN 327 Autumn 2012 LAB 3: RESPIRATORY MECHANICS Pressures throughout the cardiovascular system are important for the health of the body and of the system itself. Today we explore pulmonary pressures
Principles of mechanical ventilation. Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands
 Principles of mechanical ventilation Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands Disclosure Research grant Chiesi Pharmaceuticals Research grant CareFusion GA: 27 weeks,
Principles of mechanical ventilation Anton van Kaam, MD, PhD Emma Children s Hospital AMC Amsterdam, The Netherlands Disclosure Research grant Chiesi Pharmaceuticals Research grant CareFusion GA: 27 weeks,
Respiratory System Lab
 Respiratory System Lab Note: Review the safety materials and wear goggles when working with chemicals. Read the entire exercise before you begin. Take time to organize the materials you will need and set
Respiratory System Lab Note: Review the safety materials and wear goggles when working with chemicals. Read the entire exercise before you begin. Take time to organize the materials you will need and set
STATIC BIOMECHANICS OF THE MAMMALIAN RESPIRATORY SYSTEM 1
 STATIC BIOMECHANICS OF THE MAMMALIAN RESPIRATORY SYSTEM 1 Summary: We begin a consideration of breathing in mammals. We will start with the definitions of a series of sub- volumes of the total volume of
STATIC BIOMECHANICS OF THE MAMMALIAN RESPIRATORY SYSTEM 1 Summary: We begin a consideration of breathing in mammals. We will start with the definitions of a series of sub- volumes of the total volume of
Lung Volumes and Capacities
 BIOL242 Lung Volumes and Capacities Measurement of lung volumes provides a tool for understanding normal function of the lungs as well as disease states. The breathing cycle is initiated by expansion of
BIOL242 Lung Volumes and Capacities Measurement of lung volumes provides a tool for understanding normal function of the lungs as well as disease states. The breathing cycle is initiated by expansion of
TV = Tidal volume (500ml) IRV = Inspiratory reserve volume (3,000 ml)
 IRV = Inspiratory reserve volume (3,000 ml)") By: Amin alajlouni Lec: 2nd record Date: 29/10/2017 First of all, this is my first sheet so excuse any mistakes I might make and let's start: As we said before in our last lecture about lung capacities
By: Amin alajlouni Lec: 2nd record Date: 29/10/2017 First of all, this is my first sheet so excuse any mistakes I might make and let's start: As we said before in our last lecture about lung capacities
Experiment HS-2: Breathing and Gravity
 Experiment HS-2: Breathing and Gravity Background Over a long time, the amount of oxygen (O 2 ) taken up and carbon dioxide (CO 2 ) given off at the tissues is matched with the amount of O 2 taken up and
Experiment HS-2: Breathing and Gravity Background Over a long time, the amount of oxygen (O 2 ) taken up and carbon dioxide (CO 2 ) given off at the tissues is matched with the amount of O 2 taken up and
Independent Health Facilities
 Independent Health Facilities Assessment Protocol for Pulmonary Function Studies - Technologist Assessor INSTRUCTIONS: Please complete ( ) the attached protocol during the assessment. Ensure that all the
Independent Health Facilities Assessment Protocol for Pulmonary Function Studies - Technologist Assessor INSTRUCTIONS: Please complete ( ) the attached protocol during the assessment. Ensure that all the
mechanical ventilation Arjun Srinivasan
 Respiratory mechanics in mechanical ventilation Arjun Srinivasan Introduction Mechanics during ventilation PV curves Application in health & disease Difficulties & pitfalls The future. Monitoring Mechanics
Respiratory mechanics in mechanical ventilation Arjun Srinivasan Introduction Mechanics during ventilation PV curves Application in health & disease Difficulties & pitfalls The future. Monitoring Mechanics
3/24/2009 LAB D.HAMMOUDI.MD. 1. Trachea 2. Thoracic wall 3. Lungs 4. Primary bronchi 5. Diaphragm
 RESPIRATORY PHYSIOLOGY LAB D.HAMMOUDI.MD 1. Trachea 2. Thoracic wall 3. Lungs 4. Primary bronchi 5. Diaphragm 1 KEY WORDS TO KNOW BOYLE S LAW INTERCOSTAL NERVES PHRENIC NERVE DIAPHRAGM EXTERNAL INTERCOSTAL
RESPIRATORY PHYSIOLOGY LAB D.HAMMOUDI.MD 1. Trachea 2. Thoracic wall 3. Lungs 4. Primary bronchi 5. Diaphragm 1 KEY WORDS TO KNOW BOYLE S LAW INTERCOSTAL NERVES PHRENIC NERVE DIAPHRAGM EXTERNAL INTERCOSTAL
A Pulmonary Function Product of Rare Distinction
 A Pulmonary Function Product of Rare Distinction SpiroAir Fully Digital Positive Displacement PFT System How do you recognize PFT Excellence? The ultimate in volume and flow accuracy Reliable and reproducible
A Pulmonary Function Product of Rare Distinction SpiroAir Fully Digital Positive Displacement PFT System How do you recognize PFT Excellence? The ultimate in volume and flow accuracy Reliable and reproducible
Breathing. Physics of Breathing 11/14/2011. Function of Respiratory Tract. Structure of Respiratory Tract. Parts of the Respiratory Tract
 Breathing Function of Respiratory Tract The respiratory tract is a series of spaces and semirigid tubes designed to convey air into and out of the respiratory organs (lungs). Parts of the Respiratory Tract
Breathing Function of Respiratory Tract The respiratory tract is a series of spaces and semirigid tubes designed to convey air into and out of the respiratory organs (lungs). Parts of the Respiratory Tract
UNDERSTANDING NEONATAL WAVEFORM GRAPHICS. Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services
 UNDERSTANDING NEONATAL WAVEFORM GRAPHICS Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services Disclosures Purpose: To enhance bedside staff s knowledge of ventilation and oxygenation
UNDERSTANDING NEONATAL WAVEFORM GRAPHICS Brandon Kuehne, MBA, RRT-NPS, RPFT Director- Neonatal Respiratory Services Disclosures Purpose: To enhance bedside staff s knowledge of ventilation and oxygenation
EasyOne Pro LAB Measurement Technology Background
 Application Note CB, June 2017 EasyOne Pro LAB Measurement Technology Background Content EasyOne Pro LAB Measurement Technology Background... 1 1 Introduction... 2 2 EasyOne Pro LAB System Layout... 2
Application Note CB, June 2017 EasyOne Pro LAB Measurement Technology Background Content EasyOne Pro LAB Measurement Technology Background... 1 1 Introduction... 2 2 EasyOne Pro LAB System Layout... 2
Biology 347 General Physiology Lab Basic Pulmonary Functions: Respirometry and Factors that Effect Respiration
 Biology 347 General Physiology Lab Basic Pulmonary Functions: Respirometry and Factors that Effect Respiration Objectives Students will measure breathing parameters in a resting subject. Students will
Biology 347 General Physiology Lab Basic Pulmonary Functions: Respirometry and Factors that Effect Respiration Objectives Students will measure breathing parameters in a resting subject. Students will
bespoke In general health and rehabilitation Breath-by-breath multi-functional respiratory gas analyser In human performance
 Introduction Expired Gas Analysis or indirect calorimetry, can be used to measure ventilation and the fractions of oxygen and carbon dioxide in expired air. From these measurements, the body's oxygen consumption
Introduction Expired Gas Analysis or indirect calorimetry, can be used to measure ventilation and the fractions of oxygen and carbon dioxide in expired air. From these measurements, the body's oxygen consumption
Respiration. Exercise 1A: Breathing in Resting Volunteers Aim: To measure breathing parameters in a resting individual.
 Respiration Background The amount of air that moves in or out of the lungs during any one breathing cycle is called the tidal volume. Above and beyond normal inspiration, it is possible to breathe in additional
Respiration Background The amount of air that moves in or out of the lungs during any one breathing cycle is called the tidal volume. Above and beyond normal inspiration, it is possible to breathe in additional
What is ultrasonic plethysmography and how can we use it in airway disease?
 What is ultrasonic plethysmography and how can we use it in airway disease? Christian Buess ndd Medizintechnik AG, Zürich, Switzerland ERS 2007-1/19 Background Until approx. the year 2000 mainly the following
What is ultrasonic plethysmography and how can we use it in airway disease? Christian Buess ndd Medizintechnik AG, Zürich, Switzerland ERS 2007-1/19 Background Until approx. the year 2000 mainly the following
Figure 1. A schematic diagram of the human respiratory system.
 Introduction to Respiration In this experiment, you will investigate various aspects of normal breathing, hyperventilation, rebreathing the effect of changing airway resistance and ways in which to measure
Introduction to Respiration In this experiment, you will investigate various aspects of normal breathing, hyperventilation, rebreathing the effect of changing airway resistance and ways in which to measure
Respiratory Physiology 2
 Respiratory Physiology 2 Session Objectives. What you will cover Gaseous Exchange Control of Breathing Rate Your objectives are State the function of support structures and epithelia of the bronchial tree
Respiratory Physiology 2 Session Objectives. What you will cover Gaseous Exchange Control of Breathing Rate Your objectives are State the function of support structures and epithelia of the bronchial tree
Respiratory System Review
 KEY THIS TEST WILL BE COMPLETED IN ONE CLASS PERIOD MONDAY, MARCH 10. 2014 Respiratory System Review Name A. Directions: Fill in the blank with the appropriate vocabulary word or words (several examples
KEY THIS TEST WILL BE COMPLETED IN ONE CLASS PERIOD MONDAY, MARCH 10. 2014 Respiratory System Review Name A. Directions: Fill in the blank with the appropriate vocabulary word or words (several examples
Quality Control of Pulmonary Diagnostic Systems
 Quality Control of Pulmonary Diagnostic Systems James P. Sullivan, BA, RPFT Pulmonary Diagnostic Laboratories Memorial Sloan Kettering Cancer Center New York, New York QA, QC and QI: what s the difference?
Quality Control of Pulmonary Diagnostic Systems James P. Sullivan, BA, RPFT Pulmonary Diagnostic Laboratories Memorial Sloan Kettering Cancer Center New York, New York QA, QC and QI: what s the difference?
Initiation and Management of Airway Pressure Release Ventilation (APRV)
") Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Initiation and Management of Airway Pressure Release Ventilation (APRV) Eric Kriner RRT Pulmonary Critical Care Clinical Specialist Pulmonary Services Department Medstar Washington Hospital Center Disclosures
Cardiopulmonary Physical Therapy. Haneul Lee, DSc, PT
 Cardiopulmonary Physical Therapy Haneul Lee, DSc, PT OBJECTIVE 1. Explain the principle physiological function of the pulmonary system 2. Outline the major anatomical components of the respiratory system.
Cardiopulmonary Physical Therapy Haneul Lee, DSc, PT OBJECTIVE 1. Explain the principle physiological function of the pulmonary system 2. Outline the major anatomical components of the respiratory system.
Health Professional Info
 Health Professional Info Mouthpiece Ventilation (MPV) What is MPV? MPV is a less intrusive form of noninvasive ventilation that uses a portable home mechanical ventilator (HMV) with a single-limb open-circuit
Health Professional Info Mouthpiece Ventilation (MPV) What is MPV? MPV is a less intrusive form of noninvasive ventilation that uses a portable home mechanical ventilator (HMV) with a single-limb open-circuit
Basics of Mechanical Ventilation. Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity
 Basics of Mechanical Ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Overview of topics 1. Goals 2. Settings 3. Modes 4. Advantages and disadvantages
Basics of Mechanical Ventilation Dr Shrikanth Srinivasan MD,DNB,FNB,EDIC Consultant, Critical Care Medicine Medanta, The Medicity Overview of topics 1. Goals 2. Settings 3. Modes 4. Advantages and disadvantages
Let s talk about Capnography
 Let s talk about Capnography This is one of a series of articles by Keith Simpson BVSc MRCVS MIET (Electronics) discussing the practical aspects of some common monitoring techniques. Capnometry is the
Let s talk about Capnography This is one of a series of articles by Keith Simpson BVSc MRCVS MIET (Electronics) discussing the practical aspects of some common monitoring techniques. Capnometry is the
Paul V. Jennemann Maryland Radon Laboratory, Inc Corporate Court, Suite E Ellicott City, MD 21042
 RADON VS PROGENY Paul V. Jennemann Maryland Radon Laboratory, Inc. 3220 Corporate Court, Suite E Ellicott City, MD 21042 1. INTRODUCTION Any one who has taken a radon training course should be familiar
RADON VS PROGENY Paul V. Jennemann Maryland Radon Laboratory, Inc. 3220 Corporate Court, Suite E Ellicott City, MD 21042 1. INTRODUCTION Any one who has taken a radon training course should be familiar
Body plethysmography e Its principles and clinical use
 Respiratory Medicine (2011) 105, 959e971 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/rmed REVIEW Body plethysmography e Its principles and clinical use C.P. Criée a, *,
Respiratory Medicine (2011) 105, 959e971 available at www.sciencedirect.com journal homepage: www.elsevier.com/locate/rmed REVIEW Body plethysmography e Its principles and clinical use C.P. Criée a, *,
Selecting the Ventilator and the Mode. Chapter 6
 Selecting the Ventilator and the Mode Chapter 6 Criteria for Ventilator Selection Why does the patient need ventilatory support? Does the ventilation problem require a special mode? What therapeutic goals
Selecting the Ventilator and the Mode Chapter 6 Criteria for Ventilator Selection Why does the patient need ventilatory support? Does the ventilation problem require a special mode? What therapeutic goals
Human Respiration Laboratory Experiment By
 Human Respiration Laboratory Experiment By Alison L., Thurow, Brittany Baierlein, Rachel C. Holsinger and Robin L. Cooper Department of Biology, University of Kentucky, Lexington, KY 40506 0225, USA. Purpose:
Human Respiration Laboratory Experiment By Alison L., Thurow, Brittany Baierlein, Rachel C. Holsinger and Robin L. Cooper Department of Biology, University of Kentucky, Lexington, KY 40506 0225, USA. Purpose:
 Question 1: Define vital capacity. What is its significance? Vital capacity is the maximum volume of air that can be exhaled after a maximum inspiration. It is about 3.5 4.5 litres in the human body. It
Question 1: Define vital capacity. What is its significance? Vital capacity is the maximum volume of air that can be exhaled after a maximum inspiration. It is about 3.5 4.5 litres in the human body. It
CARDIOVIT AT-104 ergospirometry
 E D E R I T Z M A N U F A C T U R E D I N A N D S W I G N S E D L A N D CARDIOVIT AT-104 ergospirometry Cardiopulmonary exercise tests (CPET) with touch screen by SCHILLER it s the experience that counts.
E D E R I T Z M A N U F A C T U R E D I N A N D S W I G N S E D L A N D CARDIOVIT AT-104 ergospirometry Cardiopulmonary exercise tests (CPET) with touch screen by SCHILLER it s the experience that counts.
APRV: Moving beyond ARDSnet
 APRV: Moving beyond ARDSnet Matthew Lissauer, MD Associate Professor of Surgery Medical Director, Surgical Critical Care Rutgers, The State University of New Jersey What is APRV? APRV is different from
APRV: Moving beyond ARDSnet Matthew Lissauer, MD Associate Professor of Surgery Medical Director, Surgical Critical Care Rutgers, The State University of New Jersey What is APRV? APRV is different from
Physiology (3) Pulmonary Function Test:
 Pulmonary Function Test:") Pulmonary Function Test: Today we will continue with the pulmonary function test, and the question is: why do we do pulmonary function tests for patients? Can pulmonary function tests tell us what type
Pulmonary Function Test: Today we will continue with the pulmonary function test, and the question is: why do we do pulmonary function tests for patients? Can pulmonary function tests tell us what type
Blease900 Ventilator PATIENT CENTERED VENTILATION
 Blease900 Ventilator PATIENT CENTERED VENTILATIN PATIENT CENTERED VENTILATIN From the first Blease/Manley ventilator sixty years ago, Spacelabs Healthcare has built a heritage of innovative and intuitive
Blease900 Ventilator PATIENT CENTERED VENTILATIN PATIENT CENTERED VENTILATIN From the first Blease/Manley ventilator sixty years ago, Spacelabs Healthcare has built a heritage of innovative and intuitive
Unit 15 Manual Resuscitators
 15-1 Unit 15 Manual Resuscitators GOAL On completion of this unit, the student should comprehend the proper operation of self-inflating resuscitation bags, flow-inflating resuscitation bags and gas-powered
15-1 Unit 15 Manual Resuscitators GOAL On completion of this unit, the student should comprehend the proper operation of self-inflating resuscitation bags, flow-inflating resuscitation bags and gas-powered
Chapter 4: Ventilation Test Bank MULTIPLE CHOICE
 Instant download and all chapters Test Bank Respiratory Care Anatomy and Physiology Foundations for Clinical Practice 3rd Edition Will Beachey https://testbanklab.com/download/test-bank-respiratory-care-anatomy-physiologyfoundations-clinical-practice-3rd-edition-will-beachey/
Instant download and all chapters Test Bank Respiratory Care Anatomy and Physiology Foundations for Clinical Practice 3rd Edition Will Beachey https://testbanklab.com/download/test-bank-respiratory-care-anatomy-physiologyfoundations-clinical-practice-3rd-edition-will-beachey/
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo
 Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
Test Bank for Pilbeams Mechanical Ventilation Physiological and Clinical Applications 6th Edition by Cairo Link full download: http://testbankair.com/download/test-bank-for-pilbeams-mechanicalventilation-physiological-and-clinical-applications-6th-edition-by-cairo/
Lung Volumes and Capacities
 Lung Volumes and Capacities Normally the volume of air entering the lungs during a single inspiration is approximately equal to the volume leaving on the subsequent expiration and is called the tidal volume.
Lung Volumes and Capacities Normally the volume of air entering the lungs during a single inspiration is approximately equal to the volume leaving on the subsequent expiration and is called the tidal volume.
 Advanced nasal CPAP system www.hamilton-medical.com/arabella Noninvasive, low-cost, effective and safe Neonatal nasal CPAP therapy Nasal CPAP therapy aims to support neonates, especially pre-term and
Advanced nasal CPAP system www.hamilton-medical.com/arabella Noninvasive, low-cost, effective and safe Neonatal nasal CPAP therapy Nasal CPAP therapy aims to support neonates, especially pre-term and
Capnography in the Veterinary Technician Toolbox. Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA
 Capnography in the Veterinary Technician Toolbox Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA What are Respiration and Ventilation? Respiration includes all those chemical and physical
Capnography in the Veterinary Technician Toolbox Katie Pinner BS, LVT Bush Advanced Veterinary Imaging Richmond, VA What are Respiration and Ventilation? Respiration includes all those chemical and physical
Device overview. 6 Breathing circuit connection. Note: When the remote control foot pedal is connected, the manual switch is disabled.
 CoughAssist E70 Quick start guide 1 2 3 4 5 Device overview Starting therapy Modifying therapy settings Monitoring view and icons 6 7 Suggested guidelines for therapy Device menu Mask fitting 1 Device
CoughAssist E70 Quick start guide 1 2 3 4 5 Device overview Starting therapy Modifying therapy settings Monitoring view and icons 6 7 Suggested guidelines for therapy Device menu Mask fitting 1 Device
PROBLEM SET 9. SOLUTIONS April 23, 2004
 Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Harvard-MIT Division of Health Sciences and Technology HST.542J: Quantitative Physiology: Organ Transport Systems Instructors: Roger Mark and Jose Venegas MASSACHUSETTS INSTITUTE OF TECHNOLOGY Departments
Principles of Mechanical Ventilation: A Graphics-Based Approach
 Principles of Mechanical Ventilation: A Graphics-Based Approach Steven M. Donn, MD, FAAP Professor of Pediatrics Neonatal-Perinatal Medicine C.S. Mott Children s Hospital University of Michigan Health
Principles of Mechanical Ventilation: A Graphics-Based Approach Steven M. Donn, MD, FAAP Professor of Pediatrics Neonatal-Perinatal Medicine C.S. Mott Children s Hospital University of Michigan Health
Physiology - lecture 3
 Physiology - lecture 3 Residual Volume (RV):the amount of gas remaining in the lung at the end of a maximal exhalation Tidal Volume (TV):the volume of gas inhaled and exhaled during one respiratory cycle.
Physiology - lecture 3 Residual Volume (RV):the amount of gas remaining in the lung at the end of a maximal exhalation Tidal Volume (TV):the volume of gas inhaled and exhaled during one respiratory cycle.
VENTIlogic LS VENTIlogic plus. 100 % Mobility and Reliability in IV and NIV
 VENTIlogic LS VENTIlogic plus 100 % Mobility and Reliability in IV and NIV VENTIlogic VENTIlog LS Your Requirements for Reliability and Mobility are Our Benchmark. VENTIlogic LS and VENTIlogic plus are
VENTIlogic LS VENTIlogic plus 100 % Mobility and Reliability in IV and NIV VENTIlogic VENTIlog LS Your Requirements for Reliability and Mobility are Our Benchmark. VENTIlogic LS and VENTIlogic plus are
Respiratory Response to Physiologic Challenges. Evaluation copy
 Respiratory Response to Physiologic Challenges Computer 20 The respiratory cycle of inspiration and expiration is controlled by complex mechanisms involving neurons in the cerebral cortex, brain stem,
Respiratory Response to Physiologic Challenges Computer 20 The respiratory cycle of inspiration and expiration is controlled by complex mechanisms involving neurons in the cerebral cortex, brain stem,
Technical Data and Specifications
 Technical Data and Specifications INTENDED USE Ventilator designed to provide Invasive and Non-invasive ventilation for the critical care management of adult, pediatric and neonate-infant (including premature)
Technical Data and Specifications INTENDED USE Ventilator designed to provide Invasive and Non-invasive ventilation for the critical care management of adult, pediatric and neonate-infant (including premature)
Mechanical Ventilation
 Mechanical Ventilation Understanding Modes Rob Chatburn, RRT-NPS, FAARC Research Manager Respiratory Therapy Cleveland Clinic Associate Professor Case Western Reserve University 1 Overview Characteristics
Mechanical Ventilation Understanding Modes Rob Chatburn, RRT-NPS, FAARC Research Manager Respiratory Therapy Cleveland Clinic Associate Professor Case Western Reserve University 1 Overview Characteristics
PROCEDURE (TASK): ROUTINE VENTILATOR CHECK. 5. Verifies current ventilator Insures correspondence between physician's
: ROUTINE VENTILATOR CHECK. 5. Verifies current ventilator Insures correspondence between physician's") PROCEDURE (TASK): ROUTINE VENTILATOR CHECK I. KEY PERFORMANCE ELEMENTS Procedural Element (Step): Description of Performance: 5. Verifies current ventilator Insures correspondence between physician's settings
PROCEDURE (TASK): ROUTINE VENTILATOR CHECK I. KEY PERFORMANCE ELEMENTS Procedural Element (Step): Description of Performance: 5. Verifies current ventilator Insures correspondence between physician's settings
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Talmor D, Sarge T, Malhotra A, et al. Mechanical ventilation
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Talmor D, Sarge T, Malhotra A, et al. Mechanical ventilation
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES
 INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES") INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
INTRODUCTION TO BI-VENT (APRV) INTRODUCTION TO BI-VENT (APRV) PROGRAM OBJECTIVES PROVIDE THE DEFINITION FOR BI-VENT EXPLAIN THE BENEFITS OF BI-VENT EXPLAIN SET PARAMETERS IDENTIFY RECRUITMENT IN APRV USING
VT PLUS HF performance verification of Bunnell Life-Pulse HFJV (High Frequency Jet Ventilator)
") VT PLUS HF performance verification of Bunnell Life-Pulse HFJV (High Frequency Jet Ventilator) VT PLUS HF provides a special mode for evaluating the performance of high frequency ventilators while connected
VT PLUS HF performance verification of Bunnell Life-Pulse HFJV (High Frequency Jet Ventilator) VT PLUS HF provides a special mode for evaluating the performance of high frequency ventilators while connected
Mechanical power and opening pressure. Fellowship training program Intensive Care Radboudumc, Nijmegen
 Mechanical power and opening pressure Fellowship training program Intensive Care Radboudumc, Nijmegen Mechanical power Energy applied to the lung: Ptp * V (Joule) Power = Energy per minute (J/min) Power
Mechanical power and opening pressure Fellowship training program Intensive Care Radboudumc, Nijmegen Mechanical power Energy applied to the lung: Ptp * V (Joule) Power = Energy per minute (J/min) Power
Respiratory Physiology. ED Primary Teaching
 Respiratory Physiology ED Primary Teaching Functions of the respiratory system Gas exchange with O2 and CO2 Surfactant production Defence - IgA and macrophages Filer - pollutants and thromboembolism Metabolises
Respiratory Physiology ED Primary Teaching Functions of the respiratory system Gas exchange with O2 and CO2 Surfactant production Defence - IgA and macrophages Filer - pollutants and thromboembolism Metabolises
8. Pulmonary Function Testing
 8. Pulmonary Function Testing Fu 95 Rolf M. Schlegelmilch, Rüdiger Kramme Pulmonary function tests (PFT) examine the functionality of the lungs. This chapter describes the working principles of major test
8. Pulmonary Function Testing Fu 95 Rolf M. Schlegelmilch, Rüdiger Kramme Pulmonary function tests (PFT) examine the functionality of the lungs. This chapter describes the working principles of major test
Department of Biology Work Sheet Respiratory system,9 class
 I. Name the following : Department of Biology Work Sheet Respiratory system,9 class 1. A muscular sheet separating the thoracic and abdominal cavities. 2. A respiratory tube supported by cartilaginous
I. Name the following : Department of Biology Work Sheet Respiratory system,9 class 1. A muscular sheet separating the thoracic and abdominal cavities. 2. A respiratory tube supported by cartilaginous
Panther 5 Acute Care Ventilator
 1 HIGHLIGHTS High performance and advanced features target the ICU environment Utilizes an internal blower with a specially designed flow control valve removing the need for using compressed air without
1 HIGHLIGHTS High performance and advanced features target the ICU environment Utilizes an internal blower with a specially designed flow control valve removing the need for using compressed air without
Inspire rpap REVOLUTION FROM THE FIRST BREATH
 Inspire rpap TM REVOLUTION FROM THE FIRST BREATH The Inspire rpap The Inspire rpap is a revolutionary, non-invasive system for the initial stabilisation and resuscitation of infants. TM Its innovative,
Inspire rpap TM REVOLUTION FROM THE FIRST BREATH The Inspire rpap The Inspire rpap is a revolutionary, non-invasive system for the initial stabilisation and resuscitation of infants. TM Its innovative,
THE MECHANICS of RESPIRATION. Introduction
 THE MECHANICS of RESPIRATION Dr. James Duffin Departments of Physiology and Anaesthesia General Learning Objectives: 1. How is air moved into and out of the lungs? 2. What mechanical factors affect the
THE MECHANICS of RESPIRATION Dr. James Duffin Departments of Physiology and Anaesthesia General Learning Objectives: 1. How is air moved into and out of the lungs? 2. What mechanical factors affect the
LUNG CLEARANCE INDEX. COR-MAN IN Issue A, Rev INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark
 LUNG CLEARANCE INDEX METHOD COR-MAN-0000-008-IN Issue A, Rev. 3 2013-07-01 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
LUNG CLEARANCE INDEX METHOD COR-MAN-0000-008-IN Issue A, Rev. 3 2013-07-01 INNOVISION ApS Skovvænget 2 DK-5620 Glamsbjerg Denmark Tel.: +45 65 95 91 00 Fax: +45 65 95 78 00 info@innovision.dk www.innovision.dk
VENTIlogic LS VENTIlogic plus. 100 % Mobility and Reliability in IV and NIV
 VENTIlogic LS VENTIlogic plus 100 % Mobility and Reliability in IV and NIV VENTIlogic LS VENTIlogic plus Your requirements for reliability and mobility are our benchmark. VENTIlogic LS and VENTIlogic plus
VENTIlogic LS VENTIlogic plus 100 % Mobility and Reliability in IV and NIV VENTIlogic LS VENTIlogic plus Your requirements for reliability and mobility are our benchmark. VENTIlogic LS and VENTIlogic plus
The Respiratory System
 Essentials of Human Anatomy & Physiology Elaine N. Marieb Seventh Edition Chapter 13 The Respiratory System Slides 13.1 13.30 Lecture Slides in PowerPoint by Jerry L. Cook Organs of the Respiratory system
Essentials of Human Anatomy & Physiology Elaine N. Marieb Seventh Edition Chapter 13 The Respiratory System Slides 13.1 13.30 Lecture Slides in PowerPoint by Jerry L. Cook Organs of the Respiratory system
Virginia Beach EMS. Oxylator EMX. Debra H. Brennaman, RN, MPA, NREMT-P
 Virginia Beach EMS Oxylator EMX Debra H. Brennaman, RN, MPA, NREMT-P Oxylator EMX Overview Patient responsive oxygen powered resuscitation / ventilation device intended to provide emergency ventilatory
Virginia Beach EMS Oxylator EMX Debra H. Brennaman, RN, MPA, NREMT-P Oxylator EMX Overview Patient responsive oxygen powered resuscitation / ventilation device intended to provide emergency ventilatory